투고일: 2014년 12월 19일, 심사일: 2015년 1월 6일, 게재확정일: 2015년 1월 6일 책임저자:이지인, 대구시 동구 아양로 99
(701-724) 대구파티마병원 재활의학과 Tel: 053) 940-7823, Fax: 053) 940-7628 E-mail: [email protected]
Copyrights ⓒ The Korean Dysphagia Society, 2015.
침흘림에 대한 보툴리눔 톡신 치료
이지인
대구파티마병원 재활의학과
Botulinum Toxin Treatment for Sialorrhea
Zee-Ihn Lee, M.D., Ph.D.
Department of Rehabilitation Medicine, Daegu Fatima Hospital, Daegu, Korea
Sialorrhea is a distressing symptom for the patients with neurological conditions including cerebral palsy, parkinson's disease, amyotrophic lateral sclerosis and stroke, and it is mainly related to the disturbance in oral motor control rather than the excessive production of saliva in that patients. It can lead to some medical issues like oral hygiene, dentition and perioral dermatitis, and have a negative impact on social interaction. Also, the posterior drooling can cause coughing, choking and even serious respiratory complications such as aspiration pneumonia. A range of inter- ventions, which are behavioral approach, pharmacologic approach, botulinum toxin (BoTN) injection, radiotherapy or surgery, exist that aim to reduce sialorrhea but there is a lack of consensus on management approach. Over the last decade, the injection of BoTN to salivary glands has emerged as a promising method to reduce sialorrhea and has been accepted as an effective and safe treatment in patients with neurological condition. Recently, several re- searchers tried to develop an international consensus statement, providing expert recommendations on assessment, intervention with BoTN, and aftercare for both pediatric and adult drooling. Sialorrea will be best managed by a multidisciplinary team, starting with a conservative approach and then leading to more invasive procedures as appropriate. (JKDS 2015;5:1-6)
Keywords: Sialorrhea, Salivary gland, Botulinum toxin injection
서론
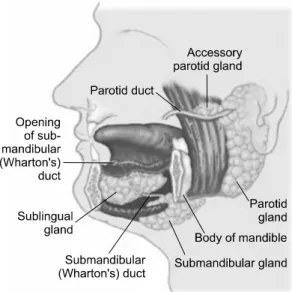
침은 각각 한 쌍 씩의 귀밑샘(parotid gland), 턱밑샘 (submandibular gland) 및 혀밑샘(sublingual gland)과 이외에 수백개의 상부 소화기관 주변 작은 침샘들에서 생성 되고 성인은 하루에 1리터, 소아는 0.5리터 정도의 침을 분 비하게 된다.(Fig. 1)
침 조절은 일반적으로 생후 15-18개월 사이에 가능하게
되므로 신생아에서의 침 흘림은 정상적인 현상이나 4세 이 후에도 지속된다면 비정상적인 침 흘림으로 고려하게 된다1. 신경학적 손상이 있는 환자들에서는 과도한 침의 생성보다 는 구강운동기능의 미숙으로 인한 침 흘림이 더 흔히 그리 고 더 심하게 일어나는 것으로 알려져 있고 운동 신경원성 질환 환자들의 50%, 파킨슨병 환자들에서는 30% 이상, 뇌 성마비 환자들에서는 58%에서 침흘림을 보인다는 보고들 이 있다2-4.
Fig. 1. Three major salivary glands and courses of salivary ducts.
침 흘림은 불쾌한 냄새, 의복이나 가구의 오염, 반복적 자극에 의한 피부손상 등 여러 가지 위생상 문제를 초래 할뿐만 아니라, 환자들의 사회적 상호작용과 자존심에 문제 를 일으키는 등의 부작용을 초래하게 되고 후방 침 흘림의 경우에는 삼킴 장애가 있는 환자들에서 기침, 구역, 구토 혹은 때때로 기도 흡인 등이 일어나게 되거나 심한 경우 흡인성 폐렴과 같은 심각한 문제를 야기할 수도 있다5-8.
그러므로 이러한 침 흘림에 대하여 행동요법, 약물치료, 보툴리눔 톡신 주사, 방사선 치료 및 수술 등의 여러 가지 치료 방법들이 사용되어왔으나 현재까지 이 중 어떤 방법이 가장 효과적인지에 대한 확실한 근거가 제시되지는 못하고 있다. 최근 수십년 간 보툴리눔 톡신의 침샘 내 주사 방법 이 침 흘림을 개선시키는데 유용한 방법으로 알려지기 시작 하였고 효과와 안정성에 대한 과학적 근거가 제시되고 있으 며 일부 연구자들에 의해 보툴리눔 톡신 주사 및 주사 이후 처치 등에 대한 기준을 전문가들에게 제공하기 위한 국제적 으로 합의된 의견이 개발되기도 하였다4,9.
본론
1. 침 흘림(sialorrhea)의 정의 및 원인
침 흘림에 대한 다양한 정의가 제시되어왔으나 Blasco 등과 Reddihough 등에 의하면 침 흘림이란 입 밖으로 의 도하지 않은 침의 소실이 일어나는 현상을 말하고 이를 전 방 침 흘림(anterior drooling)이라고 정의하며, 한편 침 흘 림의 원인과 이로 이해 야기되는 문제들에 대한 이해 및
샘으로부터 약 65%, 귀밑샘으로부터 약 23%의 침이 생성 되게 된다. 귀밑샘은 장액 세포(serous cell)로 이루어져 있 고 턱밑샘과 혀밑샘은 장액 세포와 점액 세포(mucous cell)로 이루어져있으나 턱밑샘은 장액 세포가 더 많은 반 면 혀밑샘은 점액 세포가 더 많다. 침이 끈적거리며 점도가 높은 것은 점액 세포의 분비 때문이다.
병적인 침 흘림은 다양한 원인에 의해 일어날 수 있고 이중 만성적인 침 흘림은 대설증(macroglossia)과 같은 해 부학적 구조의 이상, 약물이나 감염으로 인한 침 분비의 과 다, 뇌성마비, 뇌졸중, 파킨슨병, 지능저하, 근위축성 측삭 경화증과 같은 신경학적 손상 환자 등에서 발생한다10. 2. 침 흘림의 평가
적절한 치료를 위하여 침 흘림에 대한 평가는 정확히 이 루어질 필요가 있다. 침 흘림에 대한 평가 방법으로는 환자 나 보호자에 의해 보고되는 주관적 척도로서 Drooling rating scale, Drooling frequency and severity scale, Visual analogue scale, Drooling impact scale, Global impression of change 등이 있고(Appendix), 객관적 척 도로서 치과용 솜의 무게 측정과 같이 침 분비량을 측정하 는 방법, 떨어지는 침 방울수를 세는 것과 같이 직접 침 흘림을 관찰하는 방법, 사용된 휴지나 턱받이의 수를 세는 방법 등 다양한 방법이 있다. 또한 후방 침 흘림에 의한 흡인을 확인하기 위해서 sialogram (Fig. 2)과 같은 방사선 동위원소를 이용한 검사 방법도 있다.
3. 침 흘림에 대한 보툴리눔 톡신 치료
보툴리눔 톡신은 Clostridium botulinum에 의해 만들어 지는 신경 독소로 중쇄(heavy chain)와 경쇄(light chain) 로 구성되어 있고 신경-샘 접합부에 도달하게 되면 신경 말 단에서 신경 세포 안쪽으로 내재화된 후 경쇄가 아세틸콜린 의 유리에 관여하는 SNARE (Soluble N-ethylmaleimide- sensitive factor attachment protein receptor) 단백질 복 합체에 결합하면서 단백 분해를 일으켜서 아세틸콜린 소포
Fig. 2. Sialogram. (A) Normal, (B) Saliva aspiration through trachea and bronchi.
Fig. 3. Mechanism of Botulinum toxin action.
가 세포막 안쪽 표면에 결합하지 못해 연접 틈새(synatic cleft)로 유리되는 것이 방해됨으로써 부교감 신경의 침샘 에서의 분비 작용을 억제하게 된다11,12.(Fig. 3)
1997년 근위축성 측삭 경화증 환자들에서 A형 보툴리눔 톡신의 침샘 내 주사가 침 흘림 증상을 개선시켰다는 연구 가 보고된 이후 근위축성 측삭 경화증, 뇌성마비, 파킨슨병 등의 신경학적 손상 환자들을 대상으로 보툴리눔 톡신 주사 를 시행한 많은 연구들이 보고되고 있고 항 콜린성 약물이 나 수술 등 기존의 방법들에 비해 큰 부작용 없이 효과적으 로 침 흘림 증상을 개선시킬 수 있는 좋은 치료방법으로
인정되고 있다. 그러나 현재까지는 시술 방법, 보툴리눔 톡 신의 적절한 용량, 작용기간, 효과의 평가 방법 및 부작용 등에 대한 특별한 지침이 없는 상태이다. 주사 부위는 해부 학적 표지만을 이용하거나 초음파를 이용하여 확인할 수 있 고 초음파 유도 하에 침샘 내 보툴리눔 톡신 주사를 시행하 는 것에 대하여 일부 연구들에서는 특별한 도움이 되는 것 이 없다고 하였으나9 또 다른 연구들에서는 이 방법이 더욱 정확하고 부작용도 적다고 보고하였다13. 또한 귀밑샘에만 주사한 경우, 턱밑샘에만 주사한 경우, 귀밑샘과 턱밑샘에 주사한 경우에 대한 연구들도 있고 이들의 효과를 비교한
Fig. 4. Ultrasound-guided botulinum toxin injection into salivary gland.
연구들도 시행되었으며 이러한 연구들은 다양한 결과들을 보고하였다14,15. 최근 침흘림에 대한 보툴리눔 톡신 주사에 대한 국제적 합의를 만들고자 한 Reddihough 등에 의하면 초음파 유도 하에 귀밑샘과 턱밑샘에 함께 주사 할 것을 권장하고 있다4.(Fig. 4) 보툴리눔 톡신의 적절한 용량에 대 하여 여러 가지 연구들이 시행되어 왔고 최소 10단위에서 100단위까지 다양한 용량이 사용되었으며 Rodwell 등의 연구에 의하면 여러 연구자들이 침샘 당 사용한 평균 용량 은 25단위 혹은 몸무게 당 2단위이었다고 한다16. 일반적으 로 보툴리눔 톡신의 침 흘림 감소에 대한 효과는 약의 용량 에 비례하는 것으로 알려지고 있다. 보툴리눔 톡신 A와 B 의 효과에 대한 비교 연구들에 의하면 보툴리눔 톡신 A가 더 효과적이라는 결과도 있고 반대로 보툴리눔 톡신 B의 효과가 더 크다는 연구도 있으며 또 다른 연구에 의하면 효과가 나타날 때까지의 시간은 보툴리눔 톡신 B가 더 짧 으나 효과의 지속시간은 비슷하다고 하였다17. Lim 등의 연 구에 의하면 두 종류의 보툴리눔 톡신의 효과에 차이가 있 다는 과학적 근거는 현재까지 없는 것으로 보고하고 있다.
Reddihough 등은 한 가지 형태의 보툴리눔 톡신이 효과가 없을 때 다른 형태의 보툴리눔 톡신을 사용해 볼 것을 권하 기도 한다. 보툴리눔 톡신의 침샘 내 주사 이후 심각한 부 작용이 보고된 적은 없으나 국소적 부종, 구강 건조 및 침의 끈적거림의 심해짐 또는 드물지만 일시적 삼킴장애 등의 경 미한 부작용이 생길 수 있다.
결론
침 흘림의 치료를 고려할 때는 치료의 이득과 위험 사이 에 균형을 잘 확인하고 원치 않는 부작용을 발견할 수 있도 록 환자를 잘 관찰하는 것이 매우 중요할 것이다. 먼저 보 존적인 치료로부터 시작하여 필요하면 점점 더 침습적인 치 료 방법으로 진행하여야 한다.
치료 방법에는 크게 행동 요법, 약물 요법, 수술적 치료 등이 있다. 행동 요법은 침흘림의 정도가 가볍거나 빈도가 적은 경우에만 주로 사용 가능하다. 약물 요법 같은 경우는 구강건조, 변비, 흐린 시력 및 행동변화 등의 부작용들과 신체의 약물에 대한 적응 등의 문제로 장기간 사용에 어려 움이 있으며, 가장 침습적인 수술적 치료는 수술 후 여러 가지 합병증이 발생 가능한 단점이 있다. 이에 비하여 최근 에 신경학적 손상 환자들에서의 침흘림에 대한 치료로서 보 툴리눔 톡신 주사가 효과적이고 안전한 치료 방법임에 대한 많은 증거들이 있다. 그러나 현재까지는 주사부위, 주사 방 법, 주사 용량 및 주사 후 관리 등에 관한 명확한 지침이 없는 상태로 향후 이에 대한 연구들이 지속되어야 할 것이 다.
REFERENCES
1. Blasco PA, Allaire JH. Drooling in the developmentally
disabled: management practices and recommendations.
Consortium on Drooling. Dev Med Child Neurol 1992;
34:849-62.
2. Harriman M, Morrison M, Hay J, Revonta M, Eisen A, Lentle B. Use of radiotherapy for control of sialorrhea in patients with amyotrophic lateral sclerosis. J otolaryngol 2001;30:242-5.
3. Tahmassebi JF, Curzon ME. Prevalence of drooling in children with cerebral palsy attending special schools.
Dev Med Child Neurol 2003;45:613-7.
4. Kalf JG, Smith AM, Bloem BR, Zwarts MJ, Mulleners WM, Munneke M. Botulinum toxin A for drooling in Parkinson's disease:a pilot study to compare submandibular to parotid gland injections. Parkinsonism Relat disord 2007;13:532-4.
5. Blasco PA. Surgical management of drooling. Dev Med Child Neurol 1992;34:368-9.
6. Jongerius PH, van Hulst K, Frank JA. van den Hoogen, Rotteveel JJ. The treatment of posterior drooling by bot- ulinum toxin in a child with cerebral palsy. J Pediatr Gastroenterol Nutr 2005;41:351-3.
7. Reddihough D. Erasmus CE, Johnson H. McKeller GM.
Jongerius PH. Botulinum toxin assessment, intervention and aftercare for paediatric and adult drooling: Interna- tional consensus statement. Eur J Neurol 2010;17(S2):
109-21.
8. Harris SR, Purdy AH. Drooling and its management in cerebral palsy. Dev Med Child Neurol 1987;29:807-11.
9. Lim M, Mace A, Reza Nouraei, Sandhu G. Botulinum toxin in the management of sialorrhea: a systemic
review. Clinical Otolaryngol 2006;31:267-72.
10. Dand P, Sakel M. The management of drooling in motor neuron disease. Int J Palliat Nurs 2010;16:560-4.
11. Dressler D, Adib Saberi F. Botulinum toxin:mechanisms of action. Eur Neurol 2005; 53:3-9.
12. Bhatia KP, Munchau A, Brown P. Botulinum toxin is a useful treatment in excessive drooling in saliva. J Neurol Neurosurg Psychiatry 1999;67:697.
13. Sriskandan N, Moody A, Howlett D. Ultrasound-guided submandibular gland injection of botulinum tosin for hy- persalivation in cerebral palsy. Br J Oral Maxillofac Surg 2010;48:58-60.
14. Savarese R, Diamond M, Elovic E, Millis SR. Intraparotid injection of botulinum toxin A as a treatment to control sialorrhea in children with cerebral palsy. Am J Phys Med Rehabil. 2004;83(4):304-11.
15. Suskind DL, Tilton A. Clinical study of botulinum-A tox- in in the treatment of sialorrhea in children with cere- bral palsy. Laryngoscope 2002;112(1):73-81.
16. Rodwell K, Edwards P, Ware RS, Boyd R. Salivary gland botulinum toxin injections for drooling in children with cerebral palsy and neurodevelopmental disability: a sys- tematic review. Dev Med Child Neurol 2012;54(11):977- 87
17. Guidubaldi A, Fasano A, Ialongo T, Piano C, Pompili M, Mascianà R, et al. Botulinum toxin A versus B in sialor- rhea: aprospective, randomized, double-blind, crossover pilot study in patients with amyotrophic lateral sclerosis or Parkinson's disease. Mov Disord 2011;26:313-9.
2=Occasionally drools 3=Frequently drools 4=Constant drooling
3. Drooling Impact Scale