서 론
2016
년 통계청에 의하면 심장질환에 의한 사망률은41
.1
%이다. 이 는 총 사망원인 중2
위로,10
년 전에3
위에 비해 순위가 상승하였 다.1) 이상지질혈증은 심혈관질환의 주요 위험인자이므로 이상지질 혈증을 관리하는 것이 무엇보다 중요해졌다.2016
년 국민건강영양조사에 의하면 이상지질혈증 유병률은
2016
년 남자19
.3
%, 여자20
.2
% 이고, 남녀 모두 증가 추세로2005
년에 비해2016
년에는2
.5
배 증가 하였다.2)이상지질혈증의 치료 목표는 심혈관계 위험인자에 따라 위험군 을 분류하고 약물 치료 및 생활습관 개선을 하는 것이다. 운동요법 은 이상지질혈증 치료의 한 축으로써 크게 유산소 운동과 근력 운
Received July 24, 2018 Revised December 27, 2018 Accepted September 2, 2019
Corresponding author Jae-Seo Park
Tel: +82-2-2228-2333, Fax: +82-2-362-2473 E-mail: [email protected]
ORCID: http://orcid.org/0000-0002-8560-350X
Copyright © 2019 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Original Article
https://doi.org/10.21215/kjfp.2019.9.5.426 eISSN 2233-9116
Korean J Fam Pract. 2019;9(5):426-430
Korean Journal of Family Practice
KJFP
근력 운동 일수와 혈중 지질의 연관성: 국민건강영양조사 2016–
2018년
박재서*
연세대학교 의과대학 가정의학교실
Association between Number of Days of Muscle Strengthening Activity and Serum Lipid:
The Seventh Korea National Health and Nutrition Examination Survey, 2016–2018
Jae-Seo Park*
Department of Family Medicine, Yonsei University College of Medicine, Seoul, Korea
Background: According to Statistics Korea estimates (2016), the mortality rate associated with heart disease is 41.1%. Dyslipidemia is a major risk factor
for heart disease and warrants timely treatment. Muscle strengthening activity is one of the best therapeutic interventions for low-risk treatment groups. This study aimed to investigate the association between the number of days of muscle strengthening activity and serum lipid levels.Methods: We analyzed data obtained from the Korea National Health and Nutrition Examination Survey (2016−2018). Subjects were categorized into 3
groups based on the number of days of muscle strengthening activity performed (never, 1–2 days, ≥3 days). The association between muscle strengthening activity and serum lipid levels was determined using covariance analysis after adjusting for variables.Results: A statistically significant difference was observed among the 3 groups with respect to serum triglyceride and high-density lipoprotein (HDL)-
cholesterol levels (P=0.007 and 0.047, respectively). However, no significant differences were observed in the total serum cholesterol and low- density lipoprotein cholesterol levels (P=0.824 and 0.396, respectively).Conclusion: A statistically significant difference was observed among the 3 groups with respect to serum triglyceride and HDL-cholesterol levels. This is
a significant observation and serves as the rationale for the inclusion of muscle strengthening activity in the Korean guidelines for the management of dyslipidemia (2015). Further studies are warranted to conclusively establish the optimal quantity and quality of physical activity required for individuals with dyslipidemia.Keywords: Muscle Strengthening Activity; Physical Activity; Serum Lipid; Dyslipidemia
박재서. 근력운동 일수와 혈중 지질의 연관성
Korean Journal of Family PracticeKJFP
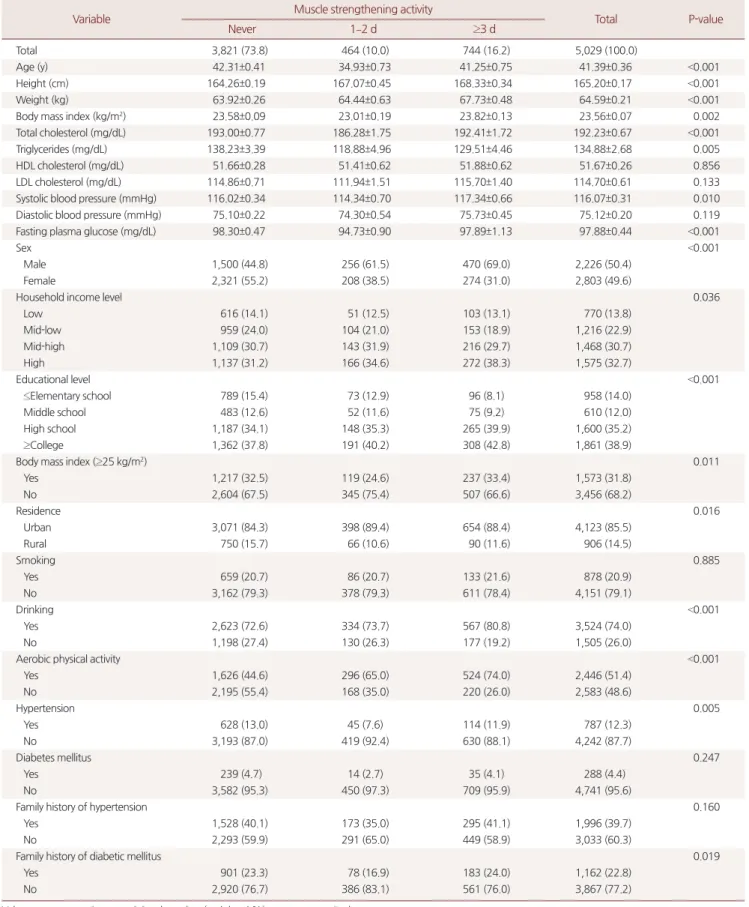
Table 1. Baseline characteristics of muscle strengthening activity groups
Variable Muscle strengthening activity
Total P-value
Never 1–2 d ≥3 d
Total 3,821 (73.8) 464 (10.0) 744 (16.2) 5,029 (100.0)
Age (y) 42.31±0.41 34.93±0.73 41.25±0.75 41.39±0.36 <0.001
Height (cm) 164.26±0.19 167.07±0.45 168.33±0.34 165.20±0.17 <0.001
Weight (kg) 63.92±0.26 64.44±0.63 67.73±0.48 64.59±0.21 <0.001
Body mass index (kg/m2) 23.58±0.09 23.01±0.19 23.82±0.13 23.56±0.07 0.002
Total cholesterol (mg/dL) 193.00±0.77 186.28±1.75 192.41±1.72 192.23±0.67 <0.001
Triglycerides (mg/dL) 138.23±3.39 118.88±4.96 129.51±4.46 134.88±2.68 0.005
HDL cholesterol (mg/dL) 51.66±0.28 51.41±0.62 51.88±0.62 51.67±0.26 0.856
LDL cholesterol (mg/dL) 114.86±0.71 111.94±1.51 115.70±1.40 114.70±0.61 0.133
Systolic blood pressure (mmHg) 116.02±0.34 114.34±0.70 117.34±0.66 116.07±0.31 0.010
Diastolic blood pressure (mmHg) 75.10±0.22 74.30±0.54 75.73±0.45 75.12±0.20 0.119
Fasting plasma glucose (mg/dL) 98.30±0.47 94.73±0.90 97.89±1.13 97.88±0.44 <0.001
Sex <0.001
Male 1,500 (44.8) 256 (61.5) 470 (69.0) 2,226 (50.4)
Female 2,321 (55.2) 208 (38.5) 274 (31.0) 2,803 (49.6)
Household income level 0.036
Low 616 (14.1) 51 (12.5) 103 (13.1) 770 (13.8)
Mid-low 959 (24.0) 104 (21.0) 153 (18.9) 1,216 (22.9)
Mid-high 1,109 (30.7) 143 (31.9) 216 (29.7) 1,468 (30.7)
High 1,137 (31.2) 166 (34.6) 272 (38.3) 1,575 (32.7)
Educational level <0.001
≤Elementary school 789 (15.4) 73 (12.9) 96 (8.1) 958 (14.0)
Middle school 483 (12.6) 52 (11.6) 75 (9.2) 610 (12.0)
High school 1,187 (34.1) 148 (35.3) 265 (39.9) 1,600 (35.2)
≥College 1,362 (37.8) 191 (40.2) 308 (42.8) 1,861 (38.9)
Body mass index (≥25 kg/m2) 0.011
Yes 1,217 (32.5) 119 (24.6) 237 (33.4) 1,573 (31.8)
No 2,604 (67.5) 345 (75.4) 507 (66.6) 3,456 (68.2)
Residence 0.016
Urban 3,071 (84.3) 398 (89.4) 654 (88.4) 4,123 (85.5)
Rural 750 (15.7) 66 (10.6) 90 (11.6) 906 (14.5)
Smoking 0.885
Yes 659 (20.7) 86 (20.7) 133 (21.6) 878 (20.9)
No 3,162 (79.3) 378 (79.3) 611 (78.4) 4,151 (79.1)
Drinking <0.001
Yes 2,623 (72.6) 334 (73.7) 567 (80.8) 3,524 (74.0)
No 1,198 (27.4) 130 (26.3) 177 (19.2) 1,505 (26.0)
Aerobic physical activity <0.001
Yes 1,626 (44.6) 296 (65.0) 524 (74.0) 2,446 (51.4)
No 2,195 (55.4) 168 (35.0) 220 (26.0) 2,583 (48.6)
Hypertension 0.005
Yes 628 (13.0) 45 (7.6) 114 (11.9) 787 (12.3)
No 3,193 (87.0) 419 (92.4) 630 (88.1) 4,242 (87.7)
Diabetes mellitus 0.247
Yes 239 (4.7) 14 (2.7) 35 (4.1) 288 (4.4)
No 3,582 (95.3) 450 (97.3) 709 (95.9) 4,741 (95.6)
Family history of hypertension 0.160
Yes 1,528 (40.1) 173 (35.0) 295 (41.1) 1,996 (39.7)
No 2,293 (59.9) 291 (65.0) 449 (58.9) 3,033 (60.3)
Family history of diabetic mellitus 0.019
Yes 901 (23.3) 78 (16.9) 183 (24.0) 1,162 (22.8)
No 2,920 (76.7) 386 (83.1) 561 (76.0) 3,867 (77.2)
Values are presented as unweighted number (weighted %) or mean±standard error.
HDL, high-density lipoprotein; LDL, low-density lipoprotein.
P-values are from Rao-scott χ2 test or ANOVA.
Original Article
Korean Journal of Family Practice
Jae-Seo Park. Association between Muslce Strengthening Activity and Serum Lipid
Korean Journal of Family Practice
KJFP
동으로 나눌 수 있다. 유산소 운동은 일반적으로 신체의 산소 소비 를 증대시키는 운동법으로 속보, 조깅, 수영 같은 운동을 말하며, 근력 운동은
10
초 이내의 짧은 운동으로 팔굽혀펴기, 단거리 달리기 등 순간적인 힘을 쓰는 운동 방법을 말한다. 기존 연구에 따르면 유 산소 운동은 중성지방을 낮추며 총콜레스테롤과 저밀도 콜레스테 롤(low-density lipoprotein cholesterol
,LDL-C
)을 낮추며 고밀도 콜레 스테롤(highdensity lipoprotein cholesterol
,HDL-C
)을 높이는 효과가 있는 반면,3,4) 근력 운동의 효과에 대해서는 논란이 있다.5,6) 이전 연 구 결과에서 일관되지 않은 다양한 결과를 보였으며 특히 국내에서 관련 연구가 미미하였다. 따라서 본 연구에서 이상지질혈증 치료에 서 운동치료의 이론적 근거를 제시하고자 근력 운동과 혈중 지질 농도와의 관계를 알아보고자 한다.방 법
1. 연구 대상
본 연구는 국민건강영양조사 제
7
기1
차년도(2016
년) 자료에 가중 치를 적용하여 사용하였다. 분석 대상은12
세 이상으로 하였고, 이 상지질혈증 치료중인 경우, 연구변수에 결측값이 있는 경우는 배제 하였다. 최초 대상자8
,150
명 중 만12
세 이상인 경우는6
,981
명이었 고, 이 중 이상지질혈증 치료중인 자를 제외하면6
,270
명이었다. 최종 적으로 이 중 연구변수에 결측값이 없는5
,029
명을 대상자로 하였다.이는 우리나라 인구수 대비 산출된 가중치를 적용하면 총
35
,679
,620
명에 해당한다.2. 조사 방법
1) 근력 운동 횟수
만
12
세 이상에서 건강 설문조사를 통해 조사하였다. 근력 운동 은 최근1
주일 동안 팔굽혀펴기, 윗몸 일으키기, 아령, 역기, 철봉 등 의 근력 운동을 말한다. 건강 설문조사상에서는 전혀 하지 않음에 서1
일,2
일,3
일,4
일,5
일 이상, 비해당(소아), 모름 및 무응답으로 구성되었다.2) 혈액 검사
혈액 검사는 공복 상태에서 채혈하여 공복 혈당, 총콜레스테롤,
HDL
콜레스테롤, 중성지방,LDL
콜레스테롤을 측정하였다. 특히HDL
콜레스테롤 자료의 측정 소급성 평가를 위해 미국 질병통제센 터 지질 표준화 프로그램(lipid standardization program
)으로부터 도 출된 전환식(HDL
원자료×1
.010–3
.172
)으로 보정한HDL
콜레스테 롤 값을 분석에 적용하였다.7)3. 통계학적 분석
분석 프로그램은
IBM SPSS Statistics for Windows
,Version 23
.0
(SPSS Inc
.,Chicago
,IL
,USA
)을 사용하였고, 복합표본설계에 맞는 방법으로 분석을 실시하였다. 근력 운동과 관련하여 연구 대상자들 을 주0
일 근력 운동, 주1–2
일 근력 운동, 주3
일 이상 근력 운동하 는3
개 집단으로 범주화하였으며, 통계처리 내용은 다음과 같다.첫째, 대상자 특성을 확인하기 위해 근력 운동 일수에 따른 범주 형 변수의 빈도와 가중 백분율을 제시하고
Rao-Scott
보정을 적용한 카이제곱검정(chi-square test
)을 실시하였으며, 연속형 변수의 평균과 표준오차를 제시하고 분산분석(ANOVA
)을 실시하였다.둘째, 근력 운동 일수에 따른 혈중 지질수치의 차이를 확인하기 위해 공분산분석(
ANCOVA
)을 실시하였다. 나이, 성별, 흡연, 음주, 비만, 유산소운동 실천 여부, 고혈압 진단여부, 당뇨 진단여부, 고혈 압 가족력, 당뇨 가족력, 동/읍면, 소득 사분위수, 교육수준 변수를 보정하였다.결 과
1. 연구 대상자의 특성
연구 대상자의 특성은
Table 1
에 정리되어 있다. 총 대상자는5
,029
명(100
.0
%)이었다. 근력 운동을 전혀 하지 않은 경우는3
,821
명 (73
.8
%)이었다. 주1–2
일 근력 운동을 한 경우464
명(10
.0
%)이었고 주3
일 이상 근력 운동을 한 경우744
명(16
.2
%)이었다.나이, 신장, 몸무게, 체질량 지수, 유산소운동 실천 여부, 총콜레 스테롤, 중성지방, 공복 혈당, 고혈압 진단 여부, 동/읍면, 소득 사분 위수, 교육수준 변수들은 근력 운동 세 집단 간 통계적으로 유의한 차이를 보였던 반면
HDL
,LDL
콜레스테롤 변수는 근력 운동 세 집 단 간에 통계적으로 유의한 차이가 없었다.2. 각 집단 간의 혈중 지질 차이(Table 2)
중성지방의 경우 근력 운동을 전혀 하지 않는 군은 평균
139
.11
, 주1–2
일 근력 운동하는 군은 평균이125
.26
, 주3
일 이상 운동하는 군 은 평균121
.56
으로 나타났으며P-value
는0
.007
로 통계적으로 유의미 한 차이를 보였다.HDL
콜레스테롤의 경우는 근력 운동을 전혀 하지 않는 군은 평 균51
.44
, 주1–2
일 근력 운동하는 군은 평균51
.25
, 주3
일 이상 운 동하는 군은52
.96
으로 나타났으며P-value
는0
.047
로 통계적으로 유 의미한 결과를 보였다.반면 총콜레스테롤의 경우, 근력 운동을 전혀 하지 않는 군은 평 균
192
.34
, 주1–2
일 근력 운동 군은 평균191
.27
, 주3
일 이상 운동 군박재서. 근력운동 일수와 혈중 지질의 연관성
Korean Journal of Family PracticeKJFP
은
192
.34
결과는 보였으나P-value 0
.824
로 통계적으로 유의한 결과 를 보이지 않았다.LDL
콜레스테롤 역시 근력 운동을 전혀 하지 않 는 군은 평균114
.30
, 주1–2
일 근력 운동하는 군은 평균115
.83
, 주3
일 이상 운동군은115
.84
결과는 보였으나P-value 0
.396
로 통계적으 로 유의한 결과를 보이지 않았다.고 찰
본 연구는
2016
년 국민건강영양조사를 이용하여 근력 운동 일수 와 혈중 지질과의 관계에 대해 조사했다. 근력 운동 일수는 전혀 하 지 않음, 주1–2
일, 주3
일 이상으로 나누어 각 연구 대상자의 특성 을 알아본 결과 나이, 신장, 몸무게, 체질량 지수, 유산소운동여부, 총콜레스테롤, 중성지방, 공복 혈당, 고혈압 진단 여부, 동/읍면, 소 득 사분위수, 교육수준는 통계적으로 유의한 차이를 보였으며 이 결과는Table 1
에 정리되어 있다. 근력 운동 군간 중성지방과HDL
콜레스테롤은 통계적으로 유의한 차이를 보였다. 반면 총콜레스테 롤과LDL
콜레스테롤은 통계적으로 유의한 차이를 보이지 않았다.근력운동과 혈중 지질 농도와의 관계에 대한 국외 연구가 많았으 나 통계적 방법에 따라 결과가 다양하게 나와 결과에 대한 논란이 있었고 국내 연구는 미미했다. 근력운동 일수에 따라
HDL
콜레스 테롤과 중성지방의 유의한 차이를 보인 본 연구의 결과는Kelley
등6) 이 수행한 메타분석에서 밝혀진 근력 운동 일수와 혈중 지질과의 관계와 일치하며, 근력운동이 지질 농도 변화에 효과적인 요법이라 는Mann
등8)의 연구 결과와도 유사하다고 할 수 있다. 따라서 본 연 구 결과는 국내 이상지질혈증 진료지침 중 낮은 위험인자군에 속한 약물 치료 대상이 아닌 사람들에게 유산소 운동과 함께 무산소 운 동도 주기적으로 시행해야 한다는 권고 문구의 의학적 근거가 됨으 로써 그 의의가 있다.9) 반면,Elliott
등10)의 연구 결과에 따르면 폐경 후 여성들에서는 근력 운동이 혈중 지질 농도에 유의한 영향을 미 치지 않았다.중성지방은 운동 시 우선적으로 쓰여지는 에너지원으로 운동에 의해 그 수치가 낮아지며, 운동에 의한
HDL
콜레스테롤의 증가는HDL
콜레스테롤 대사의 감소와apo A-1
(HDL
콜레스테롤의 주요 단백질 구성 요소) 합성 증가와 관련이 있다.11,12) 특히 근력 운동의 에너지 소비는 유산소 운동보다 적지만 근력 운동을 통해 근육량 및 높은 휴지기 대사율을 유지해주며 더 나은 인슐린 조절과 글리 코겐을 에너지 대사에 이용하는 대신 지방 대사의 증진을 촉진시켜 혈중 지질 개선효과를 기대할 수 있다는 기존 연구 결과를 통해 본 연구 결과의 기전을 추론해 볼 수 있다.13,14) 또한 높은HDL
콜레스 테롤은LDL
콜레스테롤의 산화를 억제, 항산화제 증가, 염증 감소 기전을 통해 심혈관질환의 위험을 낮춘다는 기존 연구도 있다.15)본 연구는 몇 가지 한계점이 있다. 첫째로, 설문조사를 통해 수집 한 정보이기 때문에 근력 운동의 강도와 횟수에 대해서 제한을 두 지 않고 설문자 주관에 의한 판단에서 오는 오류가 있을 수 있다.
둘째로 자료원의 한계로 인해 혈중 지질에 영향을 미칠 수 있는 인 자 중 월간 평균적 지방 섭취량과 같은 지방 관련 식이 관련 변수를 보정할 수 없었다.
본 연구 이후 근력 운동의 횟수와 강도가 혈중 지질 농도에 미치 는 영향 및 지방 식이 등의 변수 제한 등과 같은 더 세세하고 다양 한 연구가 이루어진다면 근력 운동과 혈중 지질의 연관성에 대해 더 명확하게 밝혀져 이상지질혈증 환자들에게 더욱 정확한 운동 처방 및 가이드라인을 제시할 수 있을 것이다.
요 약
연구배경:
2016
년 사망률41
.1
%에 이르는 사망원인은 심장 질환이 다. 심장 질환의 주요 위험인자 중 하나는 이상지질혈증이며, 이상 지질혈증을 적절하게 관리하는 것이 필요하다. 이상지질혈증 치료 군 중 위험성이 낮은 군에게 운동 요법은 좋은 치료법이다. 이에, 본 연구에서는 근력 운동 일수와 혈중 지질과의 연관성에 대해 알아보 Table 2. Association between number of days of muscle strengthening activity and serum lipidVariable Muscle strengthening activity
P-value
Never 1–2 d ≥3 d
Total cholesterol (mg/dL) 192.34±0.74 191.27±1.70 192.34±1.68 0.824
Triglycerides (mg/dL) 139.11±3.43 125.26±4.74 121.56±3.88 0.007
HDL cholesterol (mg/dL) 51.44±0.27 51.25±0.59 52.96±0.57 0.047
LDL cholesterol (mg/dL) 114.30±0.67 115.83±1.49 115.84±1.33 0.396
Values are presented as mean±standard error.
HDL, high-density lipoprotein; LDL, low-density lipoprotein.
All group was adjusted for age, sex, smoking group (current/non-smoker), alcohol group (current/non-drinker), body mass index (≥25 or <25), physical activity as exer- cise (applicability of aerobic exercise on survey), diagnosis of hypertension and diabetes, familial medical history, residence (rural/urban), household income level (low/
mid-low/mid-high/high), education level (≤elementary school/middle school/high school/≥college).
P-values are from ANCOVA.
Jae-Seo Park. Association between Muslce Strengthening Activity and Serum Lipid
Korean Journal of Family Practice
KJFP
고자 한다.
방법: 국민건강영양조사 근력 운동 일수에 대한 설문 및 혈중 지질 검사를 이용하였다. 대상자는 근력 운동 일수에 따라 전혀 하지 않 은 군, 주
1–2
일 운동군, 주3
일 이상 운동군의 세 집단으로 나누었 다. 세 군 간의 혈중 지질의 차이를 확인하기 위해 공분산분석 (ANCOVA
)을 실시하였다.결과: 중성지방과
HDL
콜레스테롤은 세 그룹간 통계적으로 유의한 차이를 보였다(P-value
는 차례로0
.007
,0
.047
). 반면 총콜레스테롤과LDL
콜레스테롤은 세 군간 유의한 차이를 보이지 않았다(P-value
는 차례로0
.824
,0
.396
).결론: 근력 운동 일수에 따른 세 그룹 간에 총콜레스테롤과
HDL
콜레스테롤은 통계적으로 유의미한 차이를 보였으며, 이는 국내 이 상지질혈증 진료지침의 주기적 근력 운동 실시의 근거로서 의미가 있다. 이후 운동의 질과 양에 대한 평가 및 다양한 변수를 고려한 연구가 필요하다.중심단어: 근력 운동; 신체활동; 혈중 지질; 이상지질혈증 CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported
. ORCIDJae-Seo Park
,http
://orcid
.org
/0000-0002-8560-350X
REFERENCES