Ureteral herniation occurring through the sciatic fora- men is rare, and its etiology is varied. It is difficult to identify ureteral sciatic herniation with a physical exam- ination, and the condition can cause variable degrees of urinary obstruction. Thus, diagnosis and treatment of the disorder are important. We present a case of ureteral sciatic herniation with hydronephrosis, which was treat- ed by double J catheter placement. Intravenous urogra- phy (IVU) showed a curved, laterally displaced ureter and CT images clearly depicted a herniated ureter through the sciatic foramen. The patient was treated transiently with a double J catheter.
Case Report
A 74-year-old woman was admitted to our hospital in 2005 with a voiding difficulty. The patient had diabetes mellitus, hypertension, and a history of myocardiac in-
J Korean Radiol Soc 2008;59:201-204
─ 201 ─
Ureteral Sciatic Hernia: A Case Report1
So Young Choi, M.D., Hyun Young Han, M.D., Suk Jin Park, M.D., Hyoung Shim Choe, M.D., Eun Tak Kim, M.D.2
1Department of Radiology, Eulji University Hospital
2Department of Urology, Eulji University Hospital Received May 9, 2008 ; Accepted July 17, 2008
Address reprint requests to : Hyun Young Han, M.D., Department of Radiology, Eulji University Hospital, 1306 Dunsan-dong, Seo-gu, Daejeon 302-799, South Korea
Tel. 82-42-611-3563 Fax. 82-42-611-3590 E-mail: [email protected]
A ureteral hernia that occurs through the sciatic foramen is very rare. We present a case of a ureteral sciatic hernia with hydronephrosis. Intravenous urography (IVU) showed the presence of a curved, laterally displaced ureter, and computed tomogra- phy (CT) clearly depicted the herniated ureter through the sciatic foramen. The patient was treated transiently with a double J catheter.
Index words :Ureter Hernia
Hydronephrosis
Tomography, X-Ray Computed
Fig. 1. Intravenous urography shows a loop of the left distal ureter coursing laterally and then medially (arrow). This is known as a “curlicue” ureter, a characteristic finding of ureter- al sacral herniation.
farction. The patient also had a compression fracture of the L2 vertebra, which was treated by percutaneous vertebroplasty. In addition, the patient had a hysterecto- my due to uterine prolapse. A plain supine radiograph of the abdomen (KUB) showed round radiopacity near the left sacroiliac joint; thus, a double dose IVU was per- formed. The left distal ureter was seen with a loop, coursing laterally and then medially, that is a character- istic finding of a ureteral sacral hernia (Fig. 1). However, the physician failed to notice any IVU abnormality, and the patient was diagnosed as having a neurogenic blad- der or overflow incontinence.
Two years later, the patient was readmitted due to fever, voiding difficulty, nausea and vomiting.
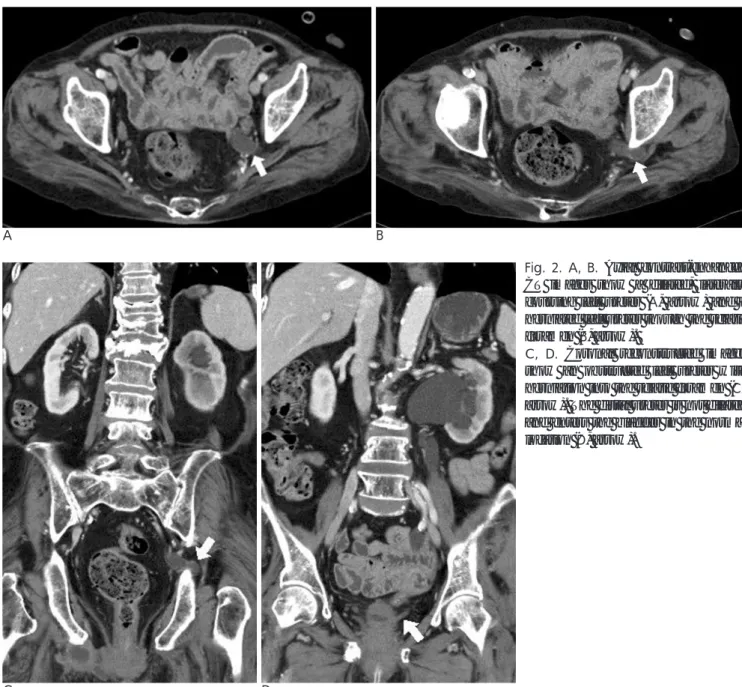
Urinalysis showed microscopic pyuria and hematuria, and a contrast-enhanced CT scan showed a dilated and laterally displaced left ureter (Fig. 2A). The left ureter was obstructed and had herniated through the sciatic foramen (Fig. 2B, C), and the left kidney showed hy- dronephrosis, mild atrophy and reduced parenchymal enhancement. However, the ureteral segment distal to the sciatic foramen was collapsed and entered the blad- der in the normal location (Fig. 2D). The urologist placed a 6-French double J catheter under endoscopic guidance and the herniated left ureter was reducted (Fig. 3). Subsequently, the patient experienced symptom relief. The patient was being treated transiently with a double J catheter.
So Young Choi, et al: Ureteral Sciatic Hernia
─ 202 ─
A B
C D
Fig. 2. A, B. Axial contrast-enhanced CT images show a dilated, laterally coursing left ureter (A, arrow) and a herniated left ureter though the sciatic foramen (B, arrow).
C, D. Coronal reconstructed images show an obstructed left ureter with herniation into the sciatic foramen (C, arrow). The distal ureter is not dilated and enters the bladder in the normal location (D, arrow).
Discussion
The sacrospinous ligament divides the sciatic notch in- to the greater and lesser sciatic foramen. The greater sci- atic foramen is bounded by the ilium laterally, by the sacrum and sacrotuberous ligament medially and by the sacrospinous ligament inferiorly (1-3).
A ureterosciatic hernia is very uncommon, and only 25 cases of a ureterosciatic hernia have been reported in the clinical literature since 1947 (4). There have been no reported cases so far in Korea.
A sciatic hernia describes the protrusion of the peri- toneal sac through the sciatic foramen, and most hernias occur through the greater sciatic foramen (3). Sciatic her- nial sacs have been reported to contain the small intes- tine, Meckel’s diverticulum, omentum, colon, ovary and ureter (2, 5). Predisposing factors include neuro- muscular disease and cachexia that can cause pyri- formis muscle atrophy (6). A congenital pelvic fascia de- fect can also cause ureteral sciatic herniation, which seems to occur more frequently in women due to a larg- er sciatic foramen and a wider pelvis (7).
It is difficult to identity ureteral sciatic herniation with
a physical examination as the gluteal muscles overly the sciatic foramen (2, 7, 8). Moreover, as the disorder can cause urinary obstruction, diagnosis is important. Our case was revealed by hydronephrosis, because the diag- nosis was not made after the initial IVU examination.
Diagnoses can be made by the use of IVU, retrograde urography or CT imaging. In particular, CT imaging can clearly depict herniated ureters through the sciatic fora- men. The characteristic finding of a ureteral sciatic her- nia is a curled ureter seen on IVU, which shows ureter displacement laterally, inferiorly, and posteriorly (3). In fact, a ureteral sciatic hernia was referred to as a
“curlicue” ureter by Beck in 1952.
The patient was being treated with retrograde double J catheter insertion under endoscopic guidance. Double J catheter placement can provide rigidity to the ureter, re- ducing the hernia. Whether this could be considered a fundamental treatment is questionable. After removal of the catheter, surgical repair might be necessary. Surgical options include reduction of the hernia, excision of the length of the redundant ureter and reimplantation (2, 9).
In summary, ureteral herniation through the sciatic foramen is very rare, and it can be diagnosed by IVU and CT imaging based on the characteristic findings and location.
References
1. Pollack HM, Popky GL, Blumerg ML. Hernias of the ureter. An anatomic roentgenographic study. Radiology 1975;117:275-281 2. Lebowitz RL. Ureteral sciatic hernia. Pediatr Radiol 1973;1:178-182 3. Weintraub JL, Pappas GM, Romano WJ, Kirsch MJ, Spencer W.
Percutaneous reduction of ureterosciatic hernia. AJR Am J Roentgenol 2000;175:181-182
4. Loffroy R, Bry J, Guiu B, Dubruille T, Michel F, Cercueil JP, et al.
Ureterosciatic hernia: a rare cause of ureteral obstruction visual- ized by multislice helical computed tomography. Urology 2007;69:385. e1-e3
5. Arat A, Haliloglu M. Ureteral-sciatic hernia in a child demonstrat- ed by voiding cystography. J Urol 1998;160:157-158
6. Stockle M, Muller SC, Riedmiller H. Ureterosciatic hernia. A rare cause of pyonephrosis. Eur Urol 1989;16:463-465
7. Noller MW, Noller DW. Ureteral sciatic hernia demonstrated on retrograde urography and surgically repaired with Boari flap tech- nique. J Urol 2000;164:776-777
8. Spring DB, Vandeman F, Watson RA. Computed tomographic demonstration of ureterosciatic hernia. AJR Am J Roentgenol 1983;141:579-580
9. Rommel FM, Boline GB, Huffnagle HW. Ureterosciatic hernia: an anatomical radiographic correlation. J Urol 1993;150:1232-1234 J Korean Radiol Soc 2008;59:201-204
─ 203 ─ Fig. 3. KUB after 6-Fr double J catheter placement in the left ureter. After catheter placement, the herniated left ureter is re- ducted, but it shows slightly lateral coursing.
So Young Choi, et al: Ureteral Sciatic Hernia
─ 204 ─
대한영상의학회지 2008;59:201-204
요관좌골공탈장: 증례 보고1
1을지대학병원 영상의학과교실
2을지대학병원 비뇨기과학교실
최소영・한현영・박숙진・최형심・김은탁2
요관좌골공 탈장은 매우 드문 질환이다. 저자들은 수신증을 동반한 요관 좌골공 탈장 1예를 경험하였기에 이를 보고하고자 한다. 경정맥 요로정맥술과 컴퓨터 단층 촬영에서 하부 요관이 좌골공을 통해 탈출 되어 있는 것을 확 인할 수 있었다. 환자는 현재 double J catheter 삽입으로 일시적인 치료를 받고 있다.