서 론
용적변조 회전방사선치료(Volumetric modulated arc therapy)는 겐트리 회전, MLC(Multileaf collimator)움직임, 선량률이 연동되어 방사선이 조사되는 방법이며 정상조직 에 대한 선량을 최소화 하면서 치료부위에 매우 정교하고 균 일한 선량분포를 만들 수 있다. 또한 선량을 전달하기 위한 MU(Monitor Unit)이 감소하여 세기변조 방사선치료에 비해 빠른시간에 선량전달이 가능한 장점을 가지고 있다.1-4)
하지만 흉ㆍ복부에 위치한 내부장기는 환자의 호흡에 따 라 위치가 변화하기 때문에 치료계획용표적체적(Planning target volume, PTV) 결정시 장기의 움직임을 고려하여 확 장하게 되는데, 이는 종양에 인접한 정상조직이 받는선량이 증가하게 되어 부작용을 발생시키게 된다.5) 이러한 이유로 용적변조 회전방사선치료의 적용범위에 제한이 되어왔지만 최근 방사선치료기술의 발전으로 호흡연동 용적변조 회전 방사선치료(Gated Volumetric modulated arc therapy)가 가 능해짐에 따라 흉・복부등 호흡에 따른 내부장기의 움직임 이 큰 부위의 치료시 호흡주기의 일정부분에서만 방사선이 조사됨으로써 종양과 정상장기의 intrafraction motion에 따 른 internal margin을 줄여 정상장기에 대한 불필요한 방사 선 조사를 최소화 할 수 있게 되었다.6)
본 논문은 2014년 4월 9일 접수하여 2014년 5월2일 채택되었음.
책임저자 : 전수동, 서울아산병원 방사선종양학과 서울특별시 송파구 올림픽로43길 88 Tel : 02) 3010-4413
E-mail : [email protected]
호흡연동 용적변조 회전방사선치료에서 호흡주기에 따른 선량전달 정확성 검증
서울아산병원 방사선종양학과
목 적 :호흡연동 용적변조 회전방사선치료(Gated Volumetric Modulated Arc Therapy)에서 환자의 호흡주기 변화에 따른 선량전달의 정확성을 검증하고자 한다.
대상 및 방법 :실험에는 TrueBeam STxTM(Varian Medical Systems, Palo Alto, CA)치료기를 사용하였다. 인체모형등가팬텀(Rando Phantom, Alderson Resarch Laboratories Inc. Stamford. CT, USA)의 전산화단층영상에 전산화치료계획시스템(Eclipse 10.0, Varian, USA)을 이용하여 10 MV FFF(Flatenning Filter Free), 선량률 1200 MU/min으로 1500 cGy/fx(Case1, 2, 3)과 220 cGy/fx(Case4, 5, 6)의 치료계획을 수립하였다.
QUASAR™ Respiratory Motion Phantom(Modus Medical Devices Inc)을 이용하여 1.5, 2.5, 3.5, 4.5 sec의 일정한 호흡주기와 평균호흡주기가 2.2, 3.5 sec인 환자의 호흡주기를 재현하였고 위상모드 30~70% 구간에서 방사선이 조사되도록 설정하였다. 각각의 호흡 조건에서 2차원 이온 전리함 배열 검출기(I’mRT Matrixx, IBA Dosimetry, Germany)와 MultiCube Phantom(IBA Dosimetry, Germany)을 이용하여 측정하였고 세기변 조 방사선치료 분석 프로그램(OmniPro I’mRT, IBA Dosimetry, Germany)을 이용하여 Gamma pass rate(3 mm, 3%)을 비교하였다.
결 과 :Case 1, 2, 3, 4, 5, 6의 Gamma pass rate은 일정한 호흡주기 1.5 sec에서 100.0, 97.6, 98.1, 96.3, 93.0, 94.8%, 2.5 sec에서 98.8, 99.5, 97.5, 99.5, 98.3, 99.6%, 3.5 sec에서 99.6, 96.6, 97.5, 99.2, 97.8, 99.1%, 4.5 sec에서 99.4, 96.3, 97.2, 99.0, 98.0, 99.3%의 결과를 보였다. 환자의 호흡을 재현한 경우 평균 호흡주기 2.2 sec에서는 97.7, 95.4, 96.2, 98.9, 96.2, 98.4%, 3.5 sec에서는 97.3, 97.5, 96.8, 100.0, 99.3 99.8%의 결과를 보였다.
결 론 : 2.5 sec이상의 일정한 호흡주기와 환자의 호흡을 재현한 실험에서 Gamma pass rate 95%이상의 임상적으로 신뢰할 만한 결과를 보였 다. 일정한 호흡주기 1.5 sec의 Case 5, 6 에서 93.0, 94.8%의 결과를 보였으나 100명의 환자 호흡주기 분석 결과 1.5 sec의 호흡을 지속했던 경 우는 없었던 점으로 보아 대부분의 호흡조건에서 정확한 선량전달이 가능함을 확인 하였다. 다만 극히 짧은 호흡주기로 인한 오차발생 가능성을 배 제할 수 없기 때문에 치료전 선량전달 정확성 검증이 선행되어야 하며 모의치료시 환자 교육으로 안정된 호흡을 유지하고 정확한 모니터링을 통해 치료중 환자 호흡변화에 대처한다면 더욱 안정적이고 정확한 치료가 이루어질 것으로 사료된다.
핵심용어 :호흡연동 용적변조 회전방사선치료, 감마지수법
전수동, 배선명, 윤인하, 강태영, 백금문
하지만 호흡연동 용적변조 회전방사선치료는 최적화된 각각의 변수들이 환자의 호흡신호에 따라 주기적으로 멈추 며 Beam on/off를 반복하는 매우 복잡하고 정교한 선량전달 과정이 요구되기 때문에 선량전달과정에서 계획된 선량의 정확도를 떨어뜨릴 수 있는 가능성을 완전히 배제할 수 없으 며 각기 다른 호흡주기에 대한 선량적 영향 또한 불확실하 다.7)
따라서 본 연구에서는 2차원 이온 전리함 배열 검출기를 이용하여 호흡연동 용적변조 회전방사선치료에서 호흡주기 에 따른 선량전달의 정확성을 검증하여 치료의 신뢰도를 확 보하고자 한다.8-10)
대상 및 방법
1. 실험 재료
- TrueBeam STxTM (Varian Medical Systems, Palo Alto, CA)
- 전산화 치료계획 시스템 (Eclipse treatment planning system Version 10.0, Varian, USA)
- 2차원 이온 전리함 배열 검출기 (I’mRT MatriXX Version 1.6, IBA Dosimetry, Germany)
- MultiCube Phantom (IBA Dosimetry, Germany) - 세기변조 방사선치료 분석 프로그램 (OmniPro I’mRT
system software Version 1.7b, IBA Dosimetry, Germany)
- 인체모형등가팬텀 (Rando Phantom, Alderson Resarch Laboratories Inc. Stamford. CT, USA)
- QUASAR™ Respiratory Motion Phantom (Modus Medical Devices Inc)
2. 실험 방법
실험에 사용한 Truebeam STxTM은 FFF(Flatenning Filter Free)의 광자선이 추가되었고 최대 2400MU/min 까지의 선 량률이 가능하다. 또한 HDMLC(High Definition Multileaf collimator)가 장착되었으며 용적변조회전방사선치료에 Jaw tracking기법의 적용이 가능한 장비이다.[Fig. 1]
인체모형등가팬텀의 전산화단층영상에 전산화 치료계획
Fig 1. TrueBeamTM(Varian Medical Systems, Palo Alto, CA)
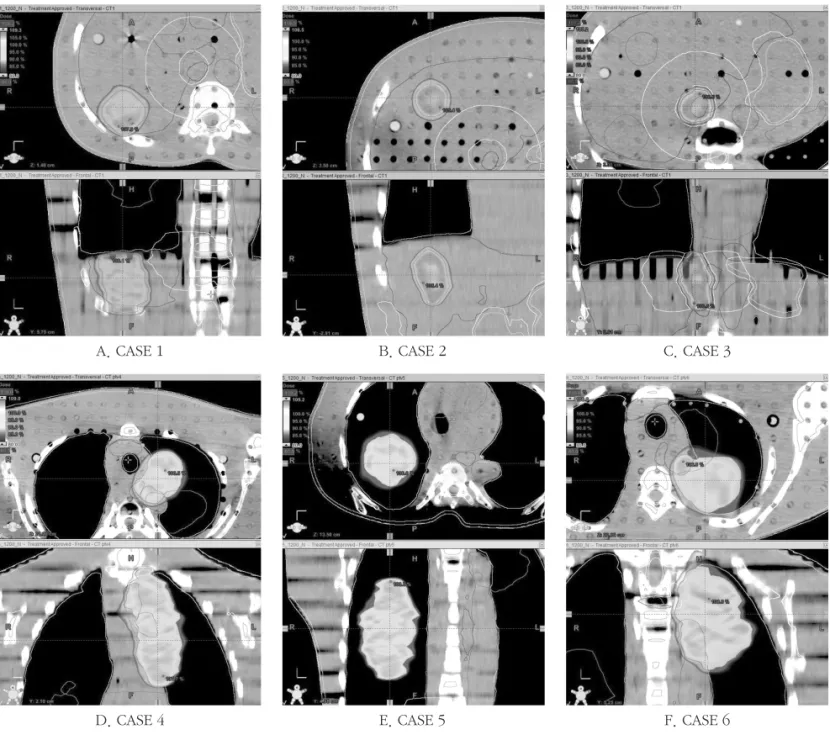
A. CASE 1 B. CASE 2 C. CASE 3
Fig 2. Treatment plan of each cases (A. CASE1, B. CASE2, C. CASE3, D. CASE4, E. CASE5, F. CASE6)
D. CASE 4 E. CASE 5 F. CASE 6
Table 1. Plan Information of each cases
CASE1 57.6 10X FFF 1200 1500 1414/1410
CASE2 22.1 10X FFF 1200 1500 1471/1472
CASE3 20.4 10X FFF 1200 1500 1762/1763
CASE4 214.3 10X FFF 1200 220 226/226
CASE5 203.7 10X FFF 1200 220 215/215
CASE6 189.6 10X FFF 1200 220 212/212
PTV volume(cm3) Energy Dose rate(MU/min) Dose(cGy/fx) MU(Field1/Field2)
Fig 3. Verification plan of each cases (A. CASE1, B. CASE2, C. CASE3, D. CASE4, E. CASE5, F. CASE6)
A. CASE 1 B. CASE 2 C. CASE 3
D. CASE 4 E. CASE 5 F. CASE 6
Fig 4. Analysis of the respiratory period for 100 Gated VMAT patient cases
시스템을 이용하여 10 MV FFF, 선량률 1200 MU/min, 2 Arc 인 1500 cGy/fx (Case1, 2, 3)과 220 cGy/fx (Case4, 5, 6)의 용적변조 회전방사선치료계획을 수립하였다.[Table 1, Fig. 2]
총 6개의 치료계획은 호흡연동 적용유무를 제외하고 모두 동일한 과정으로 수립하였다.
측정된 선량분포와의 비교를 위해 용적변조회전 방사선 치료계획을 품질관리용 치료계획으로 변환하고 관상면 방
향의 선량 평가면을 픽셀 크기 512×512, 매트릭스 크기 40
×40 ㎠의 DICOM(Digital Imaging and Communications in Medicine) 파일형식으로 변환하여 사용하였다.[Fig. 3]
호흡이 연동된 경우의 실험조건 설정을 위해 본원에서 2012년 4월 ~ 2013년 4월까지 호흡연동 용적변조 회전방사 선치료를 받은 임의의 환자 100명의 4DCT(4-dimensional Computed Tomographygraphy)촬영동안의 호흡주기를 분석 Fig 5. QUASAR™ Respiratory Motion Phantom(Modus Medical Devices Inc)
A. 1.5 sec B. 2.5 sec
C. 3.5 sec D. 4.5 sec
E. 2.2 sec (Min : 1.6 sec, Max : 3.8 sec) F. 3.5 sec (Min : 3.1 sec, Max : 4.0 sec) Fig 6. Respiratory Signal (A. 1.5 sec, B. 2.5 sec, C. 3.5 sec, D. 4.5 sec)
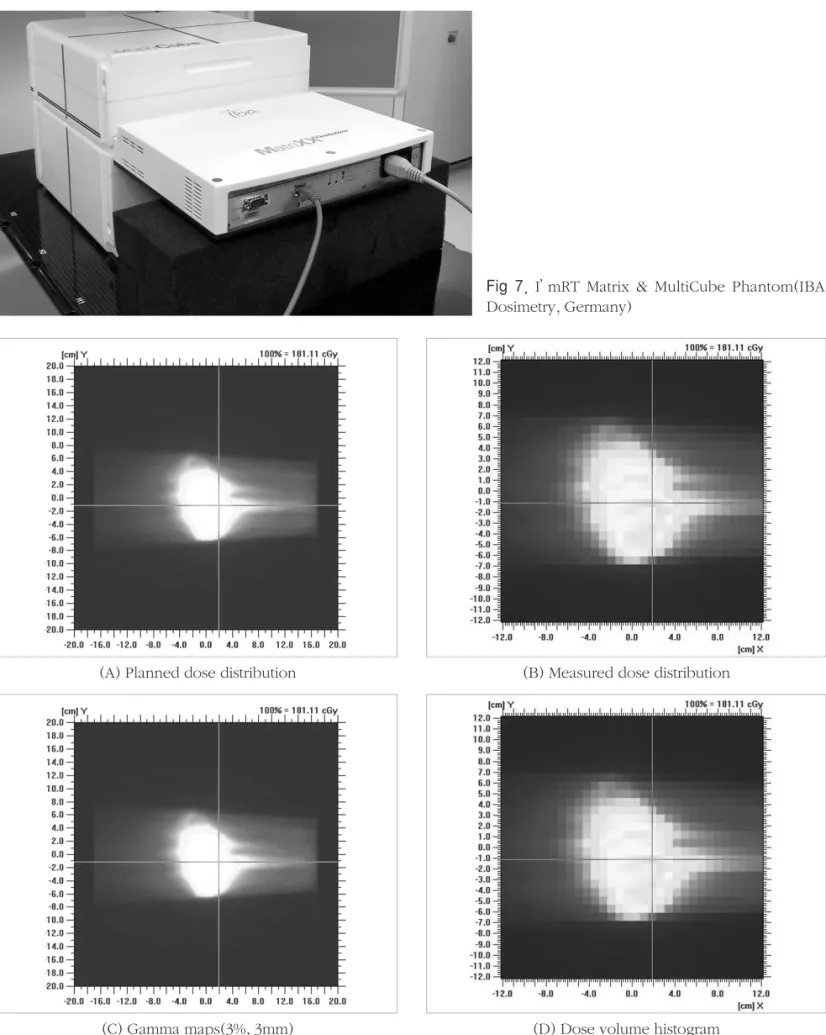
Fig 7. I’mRT Matrix & MultiCube Phantom(IBA Dosimetry, Germany)
Fig 8. Comparison of (A) planned dose distribution and (B) measured dose distributions, (C) gamma maps(3%, 3mm) and (D) dose volume histogram for one of the case
(A) Planned dose distribution (B) Measured dose distribution
(C) Gamma maps(3%, 3mm) (D) Dose volume histogram
하였다. 분석결과 평균 호흡주기는 3.5 sec에서 많은 분포를 보였고 가장 짧은 평균호흡주기는 2.2 sec였다. 또한 일시적 으로 나타났던 가장 짧았던 호흡주기는 1.5 sec였다.[Fig. 4]
분석한 결과를 바탕으로 QUASAR™ Respiratory Motion Phantom을 이용하여 1.5, 2.5, 3.5, 4.5 sec의 일정한 호흡주 기와 평균호흡주기 2.2 sec (최소 : 1.6 sec, 최대 : 3.8 sec)와 3.5 sec (최소 : 3.1 sec, 최대 : 4.0 sec)를 보였던 환자의 호 흡주기를 재현하여 적용하였고 위상모드 30~70% 구간에서 방사선이 조사되도록 설정하였다.[Fig. 5, 6]
2차원 이온 전리함 배열 검출기(평판형 전리함 수 : 1020 개, 범위 : 24.4 × 24.4 ㎠, 용적 : 0.08 ㎤, 직경 : 4.5 mm, 높 이 : 5 mm, 배열간격 : 7.62 mm 가로, 세로 일정한 간격으로 32개씩 배열)와 MultiCube Phantom을 사용하여 각 호흡조 건에서 2회씩 측정하였다.[Fig. 7]
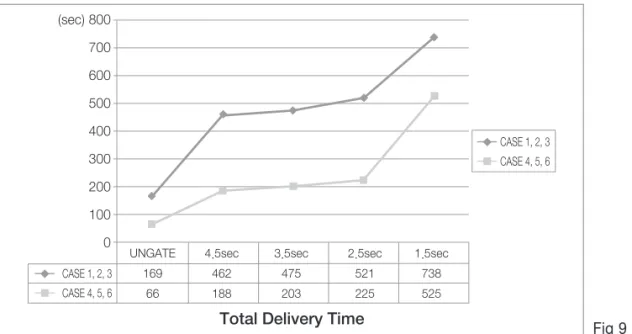
또한, 호흡조건의 변화에 따른 조사시간의 차이를 확인하 기 위하여 1500 cGy/fx가 조사되는 CASE 1, 2, 3의 기록과 220 cGy/fx가 조사되는 CASE 4, 5, 6의 기록을 평균하였다.
3. 연구결과의 분석
각 조건에서 측정된 선량분포와 계획된 선량분포의 차이 를 분석하기 위해 세기변조 방사선치료 분석 프로그램 (OmniPro I’mRT system software Version 1.7b, IBA Dosimetry, Germany)을 사용하였다.
선량에 대한 차이(dose difference, DD)와 거리상의 일치 (distance to agreement, DTA)에 대하여 이원화 된 정량적 평가방법으로 Gamma pass rate(3 mm, 3%)의 차이를 분석
하였다.11-12)[Fig. 8]
결 과
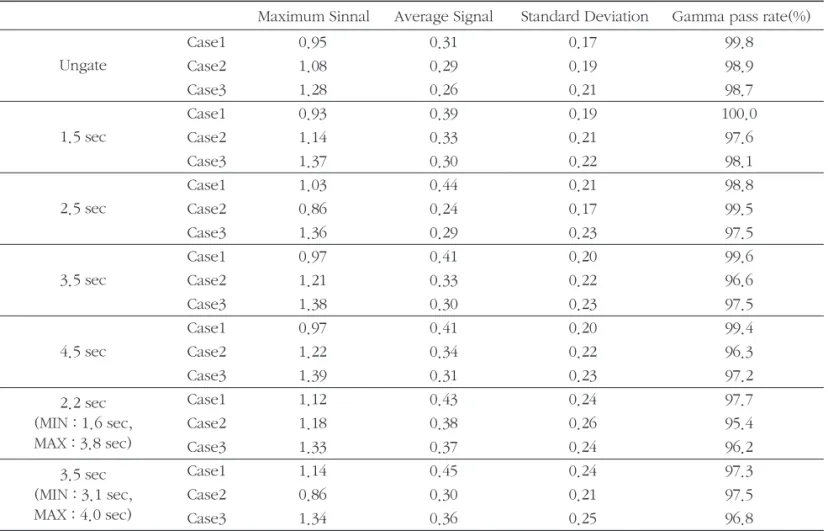
Case 1, 2, 3, 4, 5, 6의 Gamma pass rate은 호흡이 연동되 지 않은 조건에서 99.8, 98.9, 98.7, 99.3, 98.9, 98.8%, 일정 한 호흡주기 1.5 sec에서는 100.0, 97.6, 98.1, 96.3, 93.0,
Table 2. Measured data of Case 1, 2, 3
Case1 0.95 0.31 0.17 99.8
Case2 1.08 0.29 0.19 98.9
Case3 1.28 0.26 0.21 98.7
Case1 0.93 0.39 0.19 100.0
Case2 1.14 0.33 0.21 97.6
Case3 1.37 0.30 0.22 98.1
Case1 1.03 0.44 0.21 98.8
Case2 0.86 0.24 0.17 99.5
Case3 1.36 0.29 0.23 97.5
Case1 0.97 0.41 0.20 99.6
Case2 1.21 0.33 0.22 96.6
Case3 1.38 0.30 0.23 97.5
Case1 0.97 0.41 0.20 99.4
Case2 1.22 0.34 0.22 96.3
Case3 1.39 0.31 0.23 97.2
Case1 1.12 0.43 0.24 97.7
Case2 1.18 0.38 0.26 95.4
Case3 1.33 0.37 0.24 96.2
Case1 1.14 0.45 0.24 97.3
Case2 0.86 0.30 0.21 97.5
Case3 1.34 0.36 0.25 96.8
Maximum Sinnal Average Signal Standard Deviation Gamma pass rate(%)
Ungate
1.5 sec
2.5 sec
3.5 sec
4.5 sec
2.2 sec (MIN : 1.6 sec, MAX : 3.8 sec)
3.5 sec (MIN : 3.1 sec, MAX : 4.0 sec)
94.8%, 2.5 sec에서는 98.8, 99.5, 97.5, 99.5, 98.3, 99.6%, 3.5 sec에서는 99.6, 96.6, 97.5, 99.2, 97.8, 99.1%, 4.5 sec에 서는 99.4, 96.3, 97.2, 99.0, 98.0, 99.3%의 결과를 보였다.
환자의 호흡을 재현한 경우 평균 호흡주기 2.2 sec에서는 97.7, 95.4, 96.2, 98.9, 96.2, 98.4%, 3.5 sec에서는 97.3, 97.5, 96.8, 100.0, 99.3, 99.8%의 결과를 보였다.[Table 2, 3]
각 실험에서 조사시간의 차이를 확인한 결과 호흡주기가 4.5 sec에서 3.5 sec, 2.5 sec로 짧아지면서 근소한 차이로 조 사시간이 길어지는 양상을 보였으나 1.5 sec로 호흡주기가 짧아지면서 조사시간이 급격하게 길어지는 결과를 보였 다.[Fig. 9]
결 론
호흡연동 용적변조 회전방사선치료는 여러 가지 변수들 이 연동되어 선량이 전달되는 매우 복잡하고 정교한 치료방 법이다. 따라서 환자에게 정확한 선량을 전달하기 위해서는 장비의 성능을 유지하기 위한 정도관리가 기본이 되어야 하
며 환자에게 치료가 진행되기에 앞서 정확한 선량이 전달되 는가에 대한 검증이 반드시 필요하다.13-15)
본 실험을 통하여 2.5 sec이상의 일정한 호흡주기와 환자 의 호흡을 재현한 실험에서 Gamma pass rate 95%이상의 임 상적으로 신뢰할 만한 결과를 보였다. 일정한 호흡주기 1.5 sec의 Case 5, 6 에서 93.0%, 94.8%의 결과를 보였으나 100 명의 환자 호흡주기 분석 결과 가장 짧은 평균호흡주기는 2.2 sec로, 1.5 sec의 짧은호흡을 유지한 경우는 없었던 점으 로 보아 실현 가능한 대부분의 호흡조건에서 정확한 선량전 달이 가능함을 확인 할 수 있었다. 또한 조사시간 분석을 통 해서 2.5 sec 이상의 호흡주기를 유지하는 것이 조사시간에 있어서도 더 효율적인 것을 알 수 있었다.
결과적으로 호흡연동 용적변조 회전방사선치료의 적용 시 환자가 2.5 sec 이상의 호흡주기를 안정적으로 유지할 수 있다면 계획된 선량을 정확히 전달할 수 있고, 치료 시간 또 한 단축시킴으로써 치료중 환자의 자세유지에 이점이 있을 것으로 보인다. 다만 1.5 sec이하의 극히 짧은 호흡주기로 인 한 오차발생 가능성을 완전히 배제 할 수 없기 때문에 치료 전 환자호흡과 치료계획에 대한 선량전달 정확성 검증이 반 Table 3. Measured data of Case 4, 5, 6
Case4 1.10 0.32 0.20 99.3
Case5 0.74 0.38 0.22 98.9
Case6 1.14 0.35 0.19 98.8
Case4 1.58 0.44 0.25 96.3
Case5 1.92 0.57 0.29 93.0
Case6 1.77 0.51 0.29 94.8
Case4 1.07 0.32 0.19 99.5
Case5 1.32 0.39 0.21 98.3
Case6 1.17 0.34 0.18 99.6
Case4 1.14 0.34 0.20 99.2
Case5 1.36 0.42 0.23 97.8
Case6 1.20 0.36 0.20 99.1
Case4 1.17 0.34 0.21 99.0
Case5 1.36 0.42 0.22 98.0
Case6 1.20 0.36 0.20 99.3
Case4 1.14 0.35 0.22 98.9
Case5 1.37 0.43 0.27 96.2
Case6 1.12 0.39 0.22 98.4
Case4 0.91 0.28 0.19 100.0
Case5 1.06 0.35 0.20 99.3
Case6 0.56 0.36 0.20 99.8
Maximum Sinnal Average Signal Standard Deviation Gamma pass rate(%)
Ungate
1.5 sec
2.5 sec
3.5 sec
4.5 sec
2.2 sec (MIN : 1.6 sec, MAX : 3.8 sec)
3.5 sec (MIN : 3.1 sec, MAX : 4.0 sec)
드시 선행 되어야 하며 모의치료시 환자 교육을 통해 안정적 인 호흡을 유지 할 수 있도록 하고, 정확한 모니터링을 통해 치료중 환자 호흡변화에 신속하게 대처한다면 더욱 안정적 이고 정확한 호흡연동 용적변조 회전방사선치료가 이루어 질 것으로 사료된다.
참고문헌
1) Yen-Cho Huang, M.Sc, Chien-Yi Yeh at al.: Clinical practice and evaluation of electronic portal imaging device for VMAT. Medical Dosimetry 2013;38:35-41
2) Anton Mans, Peter Remeijer, Igor Olaciregui-Ruiz at al.:
3D Dosimetric Verification of volumetric modulated arc therapy by portal dosimetry. Radiotherapy and Oncology 2010;94:181-187
3) Stine Korreman, Joakim Medin, Flemming Kjær- Kristoffersen: Dosimetric verification of RapidArc treatment delivery. Acta Oncologica 2009;48:185-191
4) Bedford JL, Warrington AP: Commissioning of volumetric modulated arc therapy (VMAT). Int J Radiat Oncol Biol Phys 2009 Feb 1;73(2):537-45
5) Jiwon Sung, Myonggeun Yoon, Weon Kuu Chung at al.:
Evaluation of the Accuracy for Respiratory-gated RapidArc.
PROGRESS in MEDICAL PHYSICS 2013;June;2;24
6) Ruijiang Li, Edward Mok, Bin Han at al.: Evaluation of the geometric accuracy of surrogate-based gated VMAT using intrafraction kilovoltage x-ray images. Medical Physics 2012;39(5):2686-2693
7) Jiango Qian, Lei Xing, Wu Liu, et al.: Dose verification for respiratory-gated volumetric modulated arc therapy.
Physics In Medicine And Biology 2011;56:4827-4838
8) Giorgia Nicolini, Eugenio Vanetti, Alessandro Clivio at al.: Pre-clinical evaluation of respiratory-gated delivery of volumetric modulated arc therapy with RapidArc.
Physics In Medicine And Biology 2010;55:347-357
9) Ramesh Boggula, Mattias Birkner, Frank Lohr, et al.:
Evaluation of a 2D detector array for patient-specific VMAT QA with different setups. Physics In Medicine And Biology 2011;56: 7163-7177
10) Varatharaj Chandraraj, Sotririos Stathakis, Ravikumar Manickam et al.: Comparison of four commercial devices for RapidArc and sliding window IMRT QA.
Journal of Applied Clinical Medical Physics 2011;12:338-349
11) M.Stasi, S. Bresciani, A. Miranti at al.: Pretreatment patient- specific IMRT quality assurance: a correlation study between gamma index and patient clinical dose volume histogram. Medical Physics 2012;Dec;39(12):7626-34
Fig 9. Total delivery time
12) Francisco CH, Silvia VC: A Probability Approach to the Study on Uncertainty Effects on Gamma Index Evaluations in Radiation Therapy. Computational and Mathematical Methods in Medicine 2011; 861869:10
13) Krishna Murthy K: Patient-specific quality assurance of RapidArc treatments: Portal prediction dosimetry compared with phantom studies. Biomedical Imaging and Intervention Journal 2012;8(4):e28
14) Eduard Schreibmann, Anees Dhabaan, Eric Elder at al.:
Patient-specific quality assurance method for VMAT treatment delivery. Medical Physics 2009;Oct;36:4530
15) Giorgia Nicolini, Eugenio Vanetti, Alessandro Clivio at al.: The GLAaS algorithm for portal dosimetry and quality assurance of RapidArc, an intensity modulated rotational therapy. Radiation Oncology 2008;3:24
Purpose :The purpose of this study is to verify the accuracy of dose delivery according to the patient’s breathing cycle in Gated Volumetric Modulated Arc Therapy
Materials and Methods : TrueBeam STxTM(Varian Medical System, Palo Alto, CA) was used in this experiment. The Computed tomography(CT) images that were acquired with RANDO Phantom(Alderson Research Laboratories Inc. Stamford.
CT, USA), using Computerized treatment planning system(Eclipse 10.0, Varian, USA), were used to create VMAT plans using 10MV FFF with 1500 cGy/fx (case 1, 2, 3) and 220 cGy/fx(case 4, 5, 6) of doserate of 1200 MU/min.
The regular respiratory period of 1.5, 2.5, 3.5 and 4.5 sec and the patients respiratory period of 2.2 and 3.5 sec were reproduced with the QUASAR™ Respiratory Motion Phantom(Modus Medical Devices Inc), and it was set up to deliver radiation at the phase mode between the ranges of 30 to 70%.
The results were measured at respective respiratory conditions by a 2-Dimensional ion chamber array detector(I’mRT Matrixx, IBA Dosimetry, Germany) and a MultiCube Phantom(IBA Dosimetry, Germany), and the Gamma pass rate(3 mm, 3%) were compared by the IMRT analysis program(OmniPro I’mRT system software Version 1.7b, IBA Dosimetry, Germany)
Results :The gamma pass rates of Case 1, 2, 3, 4, 5 and 6 were the results of 100.0, 97.6, 98.1, 96.3, 93.0, 94.8% at a regular respiratory period of 1.5 sec and 98.8, 99.5, 97.5, 99.5, 98.3, 99.6% at 2.5 sec, 99.6, 96.6, 97.5, 99.2, 97.8, 99.1% at 3.5 sec and 99.4, 96.3, 97.2, 99.0, 98.0, 99.3% at 4.5 sec, respectively.
When a patient’s respiration was reproduced, 97.7, 95.4, 96.2, 98.9, 96.2, 98.4% at average respiratory period of 2.2 sec, and 97.3, 97.5, 96.8, 100.0, 99.3, 99.8% at 3.5 sec, respectively.
Conclusion :The experiment showed clinically reliable results of a Gamma pass rate of 95% or more when 2.5 sec or more of a regular breathing period and the patient’s breathing were reproduced.
While it showed the results of 93.0% and 94.8% at a regular breathing period of 1.5 sec of Case 5 and 6, it could be confirmed that the accurate dose delivery could be possible on the most respiratory conditions because based on the results of 100 patients’s respiratory period analysis as no one sustained a respiration of 1.5 sec.
But, pretreatment dose verification should be precede because we can’t exclude the possibility of error occurrence due to extremely short respiratory period, also a training at the simulation and careful monitoring are necessary for a patient to maintain stable breathing. Consequently, more reliable and accurate treatments can be administered.
Soo Dong Jeon, Sun Myung Bae, In Ha Yoon, Tae Young Kang, Geum Mun Baek
Dose verification for Gated Volumetric Modulated Arc Therapy according to Respiratory period
Department of Radiation Oncology, ASAN Medical Center, Seoul, Korea
Abstract
Keyword :Gated VMAT, Respiratory period, Gamma index