499
Open Access
Electrocardiography Patterns and the Role of the Electrocardiography Score for Risk Stratification in Acute Pulmonary Embolism
Hyeon Min Ryu, MD
1, Ju Hwan Lee, MD
2, Yong Seop Kwon, MD
3, Sang Hyuk Lee, MD
1, Myung Hwan Bae, MD
1, Jang Hoon Lee, MD
1, Dong Heon Yang, MD
1, Hun Sik Park, MD
1, Yongkeun Cho, MD
1, Shung Chull Chae, MD
1, Jae-Eun Jun, MD
1and Wee-Hyun Park, MD
11
Department of Internal Medicine, Kyungpook National University Hospital, Daegu,
2
Department of Internal Medicine, CHA University, CHA Gumi Medical Center, Gumi,
3
Department of Internal Medicine, Busan St. Mary’s Medical Center, Busan, Korea
ABSTRACT
Background and Objectives: Data on the usefulness of a combination of different electrocardiography (ECG) abnormali- ties in risk stratification of patients with acute pulmonary embolism (PE) are limited. We thus investigated 12-lead ECG patterns in acute PE to evaluate the role of the ECG score in risk stratification of patients with acute PE. Subjects and Methods:
One hundred twenty-five consecutive patients (63±14 years, 56 men) with acute PE who were admitted to Kyungpook Na- tional University Hospital between November 2001 and January 2008 were included. We analyzed ECG patterns and calcu- lated the ECG score in all patients. We evaluated right ventricular systolic pressure (RVSP) (n=75) and RV hypokinesia (n=
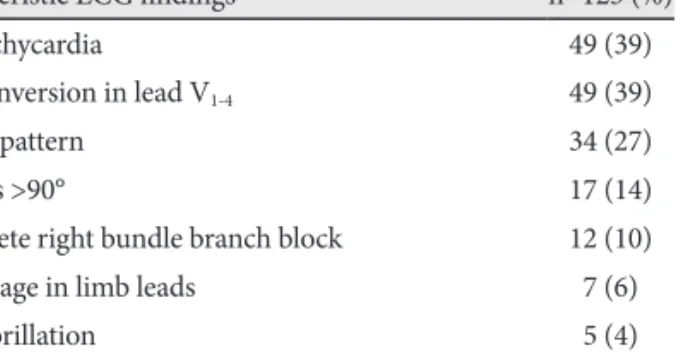
80) using echocardiography for risk stratification of acute PE patients. Results: Among several ECG findings, sinus tachy- cardia and inverted T waves in V
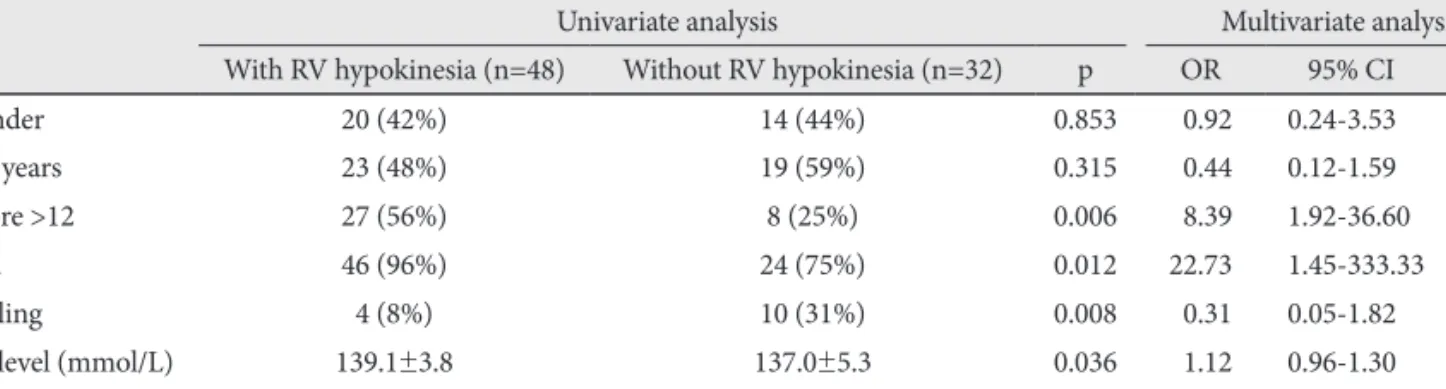
1-4(39%) were observed most frequently. The mean ECG score and RVSP were 7.36±6.32 and 49±21 mmHg, respectively. The ECG score correlated with RVSP (r=0.277, p=0.016). The patients were divided into two groups {high ECG-score group (n=38): ECG score >12 and low ECG-score group (n=87): ECG score ≤12} based on the ECG score, with the maximum area under the curve. RV hypokinesia was observed more frequently in the high ECG-score group than in the low ECG-score group (p=0.006). Multivariate analysis revealed that a high ECG score was an independent predictor of high RVSP and RV hypokinesia. Conclusion: Sinus tachycardia and inverted T waves in V
1-4were commonly observed in acute PE. Moreover, the ECG score is a useful tool in risk stratification of patients with acute PE. (Korean Circ J 2010;40:499-506)
KEY WORDS: Pulmonary embolism; Electrocardiography; Right ventricle; Systolic pressure.
Received: February 25, 2010 Revision Received: March 22, 2010 Accepted: April 14, 2010
Correspondence: Yongkeun Cho, MD, Department of Internal Medi- cine, Kyungpook National University Hospital, 200 Dongdeok-ro, Jung-gu, Daegu 700-721, Korea
Tel: 82-53-420-5528, Fax: 82-53-426-2046 E-mail: [email protected]
cc