Korean Circulation Journal
Introduction
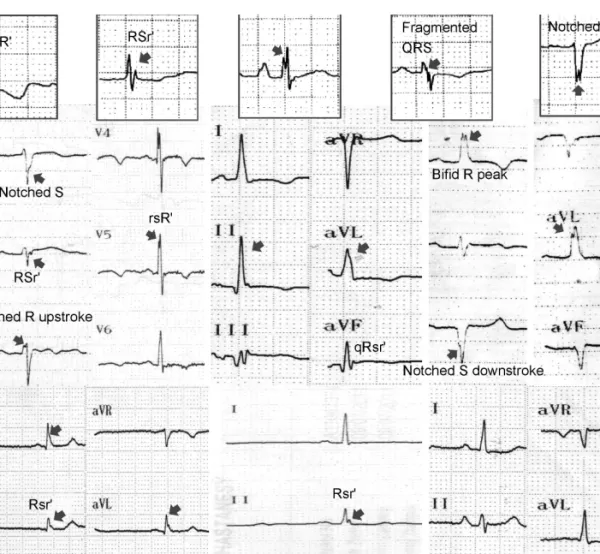
Fragmented QRS complexes (fQRS) are frequently seen on the surface electrocardiograms (ECGs) with a narrow or wide QRS com-
Print ISSN 1738-5520 • On-line ISSN 1738-5555
Absence and Resolution of Fragmented QRS Predict Reversible Myocardial Ischemia With Higher Probability of ST Segment Resolution in Patients With ST Segment Elevation
Myocardial Infarction
Mustafa Cetin, MD 1 , Sinan Altan Kocaman, MD 1 , Tuncay Kiris, MD 2 , Turan Erdogan, MD 3 , Aytun Canga, MD 1 , Murtaza Emre Durakoglugil, MD 3 , Yüksel Çiçek, MD 3 , Sitki Dogan, MD 1 , and Omer Satiroglu, MD 3
1
Department of Cardiology, Rize Education and Research Hospital, Rize,
2
Department of Cardiology, Ordu State Hospital, Ordu,
3