ISSN 0378-6471 (Print)⋅ISSN 2092-9374 (Online)
http://dx.doi.org/10.3341/jkos.2016.57.1.161
Case Report
한 눈 상전장애로 나타난 전신홍반루푸스 1예
Systemic Lupus Erythematosus Presenting as Monocular Elevation Deficiency
김승우⋅김용현⋅정승아
Seung Woo Kim, MD, Yong Hyun Kim, MD, Seung Ah Chung, MD, PhD
아주대학교 의과대학 안과학교실
Department of Ophthalmology, Ajou University School of Medicine, Suwon, Korea
Purpose: To report a case of monocular elevation deficiency as the presenting manifestation of systemic lupus erythematosus (SLE).
Case summary: A 23-year-old, otherwise healthy female presented with a 3-day history of vertical diplopia and headache. She had a left hypotropia, which worsened in adduction and supra-duction and a profound inferior oblique underaction (-3). Magnetic resonance imaging showed an enhancement around the left superior oblique muscle and multiple infarctions in the left midbrain.
On repetitive serological tests, anemia, lymphopenia, and anti-phospholipid antibody were positive. A presumptive diagnosis was a myositis of left superior oblique muscle and hyper-coagulation related with anti-phospholipid antibody. Two months after high-dose steroid treatment, the vertical diplopia was resolved. Five months later, the left hypotropia recurred as a more severe form with the inability to elevate the left eye in all directions. In addition, the infarction associated with vasculitis recurred in the left midbrain. As the treatment with high-dose steroid failed to relieve her ocular symptoms, recession of the left inferior rectus was performed 8 months later. One month after the surgery, she developed multiple lesions of erythematous nodosa with tenderness. Skin biopsy of the lesion in the fingers showed the histological findings consistent with lupus.
Conclusions: Eye movement abnormality can be an initial manifestation of SLE, which should be considered as a differential di- agnosis especially in young female patients.
J Korean Ophthalmol Soc 2016;57(1):161-166
Key Words: Anti-phospholipid antibody, Monocular elevation deficiency, Systemic lupus erythematosus
■Received: 2015. 6. 26. ■ Revised: 2015. 8. 6.
■Accepted: 2015. 10. 1.
■Address reprint requests to Seung Ah Chung, MD, PhD Department of Ophthalmology, Ajou University Hospital, #164 World cup-ro, Yeongtong-gu, Suwon 16499, Korea
Tel: 82-31-219-5257, Fax: 82-31-519-5259 E-mail: [email protected]
ⓒ2016 The Korean Ophthalmological Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
전신홍반루푸스(systemic lupus erythematosus)는 만성 특발성 염증질환으로, 과도한 자가면역항체 생성과 면역반 응을 특징으로 한다. 피부, 관절, 신장, 심장, 중추 신경계를 비롯한 거의 모든 신체부위를 침범하여 다양한 임상양상을 보이며, 증상의 악화와 완화를 반복한다. 환자의 90%가 여 성이고, 특히 젊은 가임기 여성에서 흔하게 발생한다.1-3
전신홍반루푸스 환자의 30-66%에서 안과적 증상을 동반 하며, 질병의 활성도(activity)가 높을 때 안과 증상이 나타 나는 것으로 알려져 있다.1,2 가장 흔한 안과적 동반질환은 건성각결막염(keratoconjuctivitis sicca)이지만, 시력저하를 유발하는 질환으로는 망막혈관염, 혈관폐쇄성 망막병증과 시신경염, 허헐 시신경병증이 흔하다. 이 외에도 눈 전체에 걸쳐 다양한 증상을 보일 수 있고, 뇌신경마비와 같은 신경 안과 증상으로 발현되는 경우도 있다.1-4 국내에서는 망막혈 관폐쇄, 시신경유두 울혈, 일과성 근시, 전안부 병변, 시신 경염, 시신경척수염이 보고되었으나, 안구운동장애가 전신 홍반루푸스의 첫 증상으로 나타난 국내보고는 없었다.4-9 다 만 전신홍반루푸스와 질환의 일부를 공유하는 항인지질항
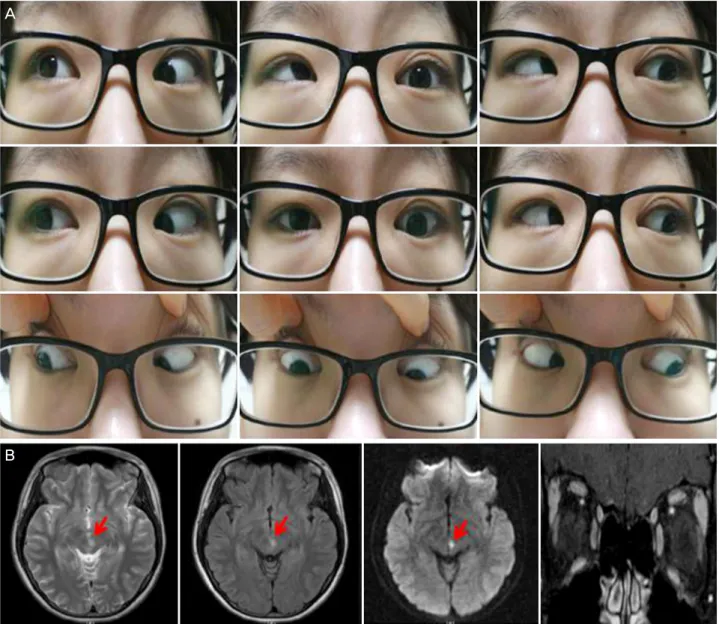
Figure 1. The clinical manifestation and imaging at the initial presentation. (A) Gaze photographs showing a profound inability to
elevate the left eye in adduction. (B) Axial T2-weighted, and diffusion brain magnetic resonance imaging (MRI) views showing fo- cal high-signal intensity with diffusion restriction in the left paramedian midbrain suggesting vasculitis and infarction (red arrows) and orbit MRI view with mild haziness around the left superior oblique muscle (yellow arrow).체 증후군(Anti-phospholipid antibody syndrome)에서 3, 4, 6번 뇌신경의 다발성 마비가 한 차례 보고되었을 뿐이다.10 이에 저자들은 안구운동장애로 발현한 전신홍반루푸스 증 례를 경험하여 국내에서는 처음으로 보고하고자 한다.
증례보고
23세 여자 환자가 3일 전부터 갑자기 시작된 수직복시와 두통을 주소로 본원 응급실로 내원하였다. 5년 전 좌측 난 소의 기형종(teratoma) 제거술을 받은 과거력 이외에는 다 른 특이 병력이 없었다. 양안의 교정시력은 모두 1.0이었고, 안압도 정상이었다. 전안부나 안저에서는 특이소견이 관찰 되지 않았다. 양안 동공의 크기나 반응도 정상이었다.
좌안 윗눈꺼풀 비측에 경한 부종과 압통이 있었고, 좌안 을 상내측으로 움직일 때 심한 통증을 호소하였다. 정면에 서 6 프리즘디옵터(prism diopter, PD) 좌안 하사시가 있었 으며, 우측 주시와 상측 주시에서 각각 16PD로 사시각이 증가하였다. 뚜렷한 좌안 하사근 기능저하(-3)가 있었고 강 제견인검사에서 양성이어서 좌안 브라운증후군에 합당하 였다(Fig. 1A). 복시와 두통 때문에 신경과에서 시행하였던 뇌 자기공명영상에서 좌측 중뇌에서 다발성 경색이 관찰되 었고, 좌안 상사근 주변에 경도의 균일하지 않은 조영증강 소견을 보였다(Fig. 1B). 반복된 혈청학적 검사에서 빈혈과 림프구감소증(Lymphocyte: 1,332/mm3)이 있었고, 항인지 질항체(anti-phospholipid antibody) 중 루푸스 항응고인자 (lupus anticoagulant)가 양성이었다. 또한 homocysteine이
A
B
Figure 2. The clinical manifestation and imaging five months after the initial presentation. (A) Gaze photographs showing five
months after the initial presentation showing a profound inability to elevate the left eye in all directions. (B) Axial T2-weighted, and diffusion brain magnetic resonance imaging (MRI) views showing a new focal high-signal intensity with diffusion restriction in the left paramedian midbrain, more upper segment than previous lesion (red arrows) and orbit MRI view with no remarkable finding in- cluding extraocular muscles.상승(30.7 μMol/L, 정상: 3.7-13.9 μMol/L)되어 있었다. 항 핵항체를 비롯한 각종 자가항체검사와 갑상샘기능검사는 정상이었다. 좌안상사근염과 항인지질항체로 인한 과응고 상태로 의심되어, 고용량 스테로이드 치료를 신경과에서 시행하였다. Methylprednisolone 1 g을 하루 1회 5일간 정 맥 주사 후, prednisolone 50 mg으로 경구 복용을 시작하여 2주 간격으로 감량하였다. 입원기간 중 안구 통증은 소실되 었고, 2개월 뒤 우상방을 제외한 모든 방향에서 정위였으 며, 수직복시를 호소하지 않았다. 재발 방지를 위해 aspirin 복용을 권유하였으나 환자가 자의로 복용하지 않았다.
5개월 뒤 수 분간의 의식소실과 함께 수직복시가 재발하
였다. 교대프리즘가림검사에서 30PD 좌안 하사시가 정면 에서 있었고, 모든 상전방향에서 좌안 상전이 전혀 되지 않 았다(-4) (Fig. 2A). 강제견인검사에서 뚜렷한 저항은 느껴 지지 않았다. 경도의 좌안 윗눈꺼풀후퇴가 보였고, 얼음검 사에서 눈꺼풀 위치나 안구운동의 변화는 없었다. 그 외에 동공기능을 포함하여 안과적 특이소견은 관찰되지 않았다. 뇌 자기공명영상에서 이전 병변보다 상측 부위 좌측 중뇌 에서 경색이 관찰되었고, 안와에서는 특이소견이 관찰되지 않았다(Fig. 2B). 뇌 혈관조영술에서 뇌혈관 동맥류나 협착 과 같은 특이소견은 관찰되지 않았다. 혈청학적 검사에서 적혈구 침강속도(erythrocyte sedimentation rate, ESR)가 67
A
B
Figure 3. Gross appreance and histological finding of the skin lesions. (A) Photographs showing erythematous discoid rash with ten-
derness and pruritus at 2nd and 3rd fingers (black arrows). (B) Histologic finding of skin lesion showing perivascular lymphocytic infiltration and a few necrotic keratinocytes suggesting lupus erythematosus (HE stain, ×100). HE = Hematoxylin-Eosin.mm/hr로 증가되고(정상: <25 mm/hr), D-dimer가 547 ng/mL 로 증가되어(정상: <500 ng/mL) 있는 것을 제외하고는 각종 자가항체검사와 갑상샘기능검사를 포함하여 정상이었다.
좌측 중뇌 경색이 혈관염이나 항인지질 항체에 의한 과응 고상태가 재발하여 발생한 것으로 판단하여, 이전과 동일 한 용량과 투여방법으로 고용량 스테로이드 치료를 신경과 에서 다시 시행하였다. 하지만 8개월 뒤에도 정면에서 18PD 좌안 하사시와 중등도의 상전장애(-2)가 남아있어서, 점안마취로 좌안 하직근 후전술 5.5 mm를 시행하였다. 수 술 중 시행한 강제견인검사에서 뚜렷한 기계적 제한은 없 었고, 수술을 위해 노출된 하직근 주변에서도 특이 소견이 관찰되지 않았다.
사시수술 1개월 후 압통을 동반한 다발성 홍반이 손에 발생하여 피부과에서 조직검사를 시행하였다. 조직학적 검 사에서 림프구의 혈관주변 침윤소견과 괴사소견이 관찰되 었으며 면역조직화학염색에서 루프스에 합당한 소견이 확 인되었다(Fig. 3). 이후 hydroxychloroquine 복용으로 피부 병변이 소실되었고, 혈전예방효과를 위해 지속적으로 hy- droxychloroquine 200 mg을 복용 중이다. 사시수술 후 17 개월까지 정면과 하방 주시에서 정위였고, 안구운동장애는 보이지 않았으며, 복시, 통증과 같은 증상의 재발은 없었다.
고 찰
본 증례는 평소 건강했던 젊은 여자 환자에서 상사근염
형태의 후천성 브라운증후군이 발생하였고, 5개월 뒤 같은 눈에 3번 뇌신경 윗분지의 부분마비가 발생하여 모든 방향 에서 상전장애(한 눈 상전장애)가 관찰되었다. 전신적으로 는 빈혈과 림프구감소증, 루프스 항응고인자 양성, 의식소 실을 동반한 뇌병변, 원반형 피부병변이 순차적으로 나타 나서 미국 류마티즘 학회의 전신홍반루푸스 진단기준(1997 년 수정)에 합당하였다.
전신홍반루푸스는 환자마다 임상경과가 매우 다양하고, 재발과 완화를 반복하며, 다른 자가면역질환을 동반할 수 도 있어, 진단이 어려운 경우들이 종종 있다.1-3 안구운동장 애가 전신홍반루푸스의 첫 증상으로 나타난 경우로는 눈근 무력증을 동반한 상하전장애, 6번 뇌신경마비, 양안 상사근 염으로 발현한 증례들이 있었다.11-14 반면, 이미 전신홍반루 푸스로 진단된 환자에서 나타난 안구운동장애에 대해서는 보다 많은 보고들이 있었다.1-3 전신홍반루푸스 환자 113명 을 대상으로 한 Keane3의 연구에서, 33명(29%)의 환자에서 안구운동장애가 관찰되었으며, 이 중 48%는 뇌줄기 경색, 33%는 뇌수막염이 원인이었다. 본 증례에서도 첫 증상 때 과응고 상태로 인하여 좌측 중뇌에 다발성 뇌경색이 발생 하였고, 5개월 뒤에는 의식소실과 함께 이전 병변 부위 근 처에 뇌경색이 추가로 발생하였다. 첫 증상 때의 안구운동 은 임상양상이나 영상학적 검사에서 마비사시보다는 안와 근염에 의한 제한사시에 보다 합당하였지만, 두 번째 발현에 서는 좌측 중뇌 경색과 연관된 좌측 3번 뇌신경의 부분마비 (윗분지)에 합당하였다. 첫 안구운동장애가 고용량 스테로이
A B
드에 잘 반응하였으나, 두 번째 증상은 스테로이드에 반응하 지 않고 8개월이 지나도 의미있는 수직편위가 남아 수술적 교정이 필요하였던 점도 이를 뒷받침할 수 있겠다.
전신홍반루푸스는 눈 전체에 걸쳐 만성 염증성 질환이 나, 혈관폐쇄성 질환을 일으킬 수 있다.1-9 전안부 문제가 가 장 흔하지만, 시력을 직접적으로 위협하는 망막혈관이나 맥락막 이상에 대해 많이 알려져 있다.1,2,4,8 신경안과적으로 도 시력과 관련된 시신경염이나 허혈 시신경병증에 대한 보고들이 많다.2,5 하지만 안구운동장애도 드물지 않게 발생 하며, 전신홍반루푸스 환자의 5-42%에서는 뇌신경병증이 다양한 형태로 발생하는 것으로 알려져 있다.1-3 3, 4, 6번 뇌신경마비, 신경핵사이 눈근육마비, 1과 1/2 증후군, 눈떨 림과 같이 뇌병변과 관련된 경우도 있고, 외안근염을 포함 한 비특이성 안와염증과 같은 염증질환으로 나타나기도 하
였다.1-3,11-14 이러한 임상양상은 해당 뇌신경 부위의 미세혈
관이 혈전 등에 의해 폐쇄되거나, 과도한 자가면역 활성화 로 면역복합체의 침착 등 염증으로 인해 생기는 것으로 생 각되고 있다.2 따라서 허헐성 병변과 염증성 병변이 함께 존재할 수 있다.
항인지질항체는 혈전 형성을 촉진하므로, 안과적으로도 혈관폐쇄성 망막병증에서 항인지질항체가 양성인 경우의 빈도가 높았다.4,8,15 또한 항인지질항체 증후군에서 3, 4, 6 번 뇌신경의 다발성 마비가 발생한 국내보고도 있었다.10 본 증례도 루푸스 항응고인자가 양성으로, 혈전 형성으로 인해 젊은 나이에 뇌경색이 발생한 것으로 생각된다.
현재까지 브라운증후군으로 전신홍반루푸스가 처음 발 현한 경우는 전 세계적으로 5 증례뿐이며,14 이후에 3번 뇌 신경의 부분마비로 인해 한 눈 상전장애 형태로 나타난 경 우는 본 증례가 처음이다. 또한 이전에 보고된 전신홍반루 푸스에서 나타난 3번 뇌신경의 부분마비는 눈근무력증과 동반된 경우였다.13
본 증례를 통해 안구운동장애가 전신홍반루프스의 첫 발 현 증상일 수 있음을 다시 한 번 확인할 수 있었다. 따라서 젊은 여자 환자에서, 염증성 병변과 허헐성 병변이 함께 있 는 경우 감별진단으로 전신홍반루프스도 고려해야 하겠다.
REFERENCES
1) Arevalo JF, Lowder CY, Muci-Mendoza R. Ocular manifestations of systemic lupus erythematosus. Curr Opin Ophthalmol 2002;
13:404-10.
2) Teoh SC, Yap EY, Au Eong KG. Neuro-ophthalmological manifes- tations of systemic lupus erythematosus in Asian patients. Clin Experiment Ophthalmol 2001;29:213-6.
3) Keane JR. Eye movement abnormalities in systemic lupus erythematosus. Arch Neurol 1995;52:1145-9.
4) Yoon CK, Park JH, Yu HG. Retinopathy associated with systemic lupus erythematosus. J Korean Ophthalmol Soc 2009;50:1215-20.
5) Im CY, Kim SS, Kim HK. Bilateral optic neuritis as first manifes- tation of systemic lupus erythematosus. Korean J Ophthalmol 2002;16:52-8.
6) Hwang HS, Kim DH. Transient myopia with severe chemosis asso- ciated with systemic lupus erythematosus. J Korean Ophthalmol Soc 2007;48:1445-8.
7) Ahn SM, Kim SS. A case of coexisting neuromyelitis optica in sys- temic lupus erythematosus. J Korean Ophthalmol Soc 2013;54:
1469-74.
8) Kim IT, Na SC, Lee KJ. Vascular occlusions associated with anti- phospholipid antibodies in systemic lupus erythematosus. J Korean Ophthalmol Soc 2000;41:427-32.
9) Kim IT, Chang SD. Papilledema and cerebral venous thrombosis in a patient with systemic lupus ery thematosus. J Korean Ophthalmol Soc 1999;40:2015-9.
10) Shin SY, Lee JM. A case of multiple cranial nerve palsies as the ini- tial ophthalmic presentation of antiphospholipid syndrome.
Korean J Ophthamol 2006;20:76-8.
11) Saleh Z, Menassa J, Abbas O, et al. Cranial nerve VI palsy as a rare initial presentation of systemic lupus erythematosus: case report and review of the literature. Lupus 2010;19:201-5.
12) Koch M, Langmann A. Diplopia as the presenting sign of systemic lupus erythematosus: the chameleon diagnosis. J AAPOS 2006;
10:184-5.
13) Appenzeller S, Veilleux M, Clarke A. Third cranial nerve palsy or pseudo 3rd nerve palsy of myasthenia gravis? A challenging diag- nosis in systemic lupus erythematosus. Lupus 2009;18:836-40.
14) Fonseca P, Manno RL, Miller NR. Bilateral sequential trochleitis as the presenting feature of systemic lupus erythematosus. J Neuroophthalmol 2013;33:74-6.
15) Montehermoso A, Cervera R, Font J, et al. Association of anti- phospholipid antibodies with retinal vascular disease in systemic lupus erythematosus. Semin Arthritis Rheum 1999;28:326-32.
= 국문초록 =
한 눈 상전장애로 나타난 전신홍반루푸스 1예
목적: 한 눈 상전장애로 발현한 전신홍반루푸스 증례를 경험하여 보고하고자 한다.
증례요약: 평소 건강하였던 23세 여자 환자가 3일 전부터 발생한 수직복시와 두통을 주소로 내원하였다. 내전과 상전 시 악화되는 좌안 하사시가 있었고 현저한 좌안 하사근 기능저하(-3)가 있었다. 자기공명영상에서 좌안 상사근 주변에 염증소견과 좌측 중뇌에 다발성 경색이 관찰되었고, 반복적인 혈청학적 검사에서 빈혈, 림프구감소증과 항인지질항체가 양성이었다. 좌안 상사근염과 항인지 질항체로 인한 과응고 상태로 의심되어 고용량 스테로이드로 치료하고 2개월 뒤 수직복시가 소실되었다. 5개월 뒤 좌안 하사시가 모든 상전방향에서 악화된 형태로 재발하였고, 좌측 중뇌에 혈관염에 의한 경색이 추가 발생하여, 고용량 스테로이드로 치료하였다.
좌안 하사시가 치료에 반응하지 않아서, 8개월 뒤 좌안 하직근 후전술을 시행하였다. 수술 1개월 후 압통을 동반한 다발성 홍반이 발생하여 손가락 병변에서 피부조직검사를 시행하였고, 루푸스에 합당한 병리소견이 관찰되었다.
결론: 전신홍반루푸스가 안구운동장애로 첫 발현할 수 있으므로, 젊은 여자 환자에서는 감별질환의 하나로 고려하여야 하겠다.
<대한안과학회지 2016;57(1):161-166>