─ 5 ─ elSSN 2287-1683
plSSN 1738-8767
Journal of Trauma and Injury Vol. 27, No. 1, March, 2014
� Case Report � [ J Trauma Inj 2014;27:5-8 ]
� Address for Correspondence : Pil Won Seo, M.D.
Department of Thoracic & Cardiovascular Surgery, Dankook University College of Medicine, Dankook University Hospital, 16-5 Anseo-dong, Cheonan-si, Chungcheongnam-do, Korea
Tel : 82-41-550-6269, Fax : 82-41-550-0524, E-mail : [email protected]
Submitted : September 30, 2013 Revised : November 5, 2013 Accepted : April 9, 2014
I. Introduction
Blunt traumatic cardiac rupture is a relatively uncommon injury and usually associated with a high mortality rate. It could be arisen from motor vehicle accidents, falls from height, and crush injuries.
Diagnosis of blunt traumatic cardiac rupture is sometimes difficult, especially in stable patients.
Echocardiography is a safe and quick diagnostic tool for hemodynamically unstable patients. Once cardiac rupture is suspected, early surgical exploration and
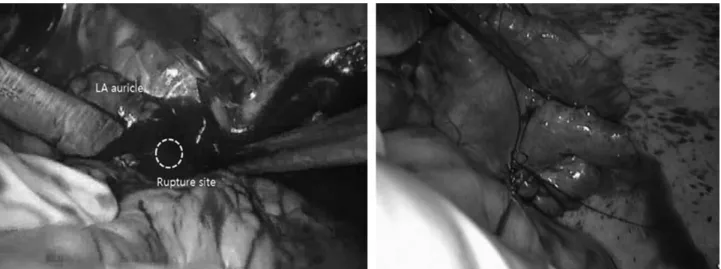
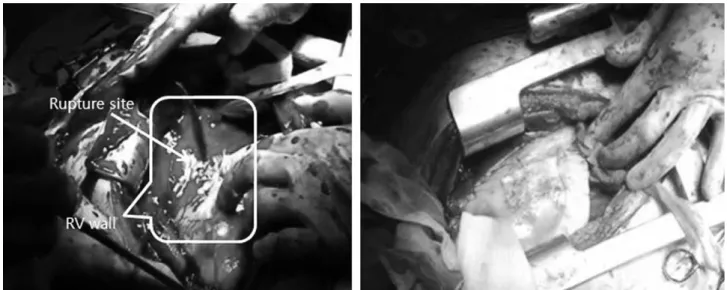
mechanical cardiopulmonary support should be con- sidered. Here in, we reported two cases of success- fully recovered from blunt traumatic cardiac rupture through early surgical exploration and application of ECMO.
II. Case Report
1. Case 1
A 36 years old male patient had fallen down from
둔상성 외상에 의한 심장파열에 대한 수술적 치험