ISSN 0378-6471 (Print)⋅ISSN 2092-9374 (Online)
http://dx.doi.org/10.3341/jkos.2015.56.4.592
Case Report
안와관통상으로 인해 발생한 상안와열증후군 경과관찰 1예
A Case of Superior Orbital Fissure Syndrome Induced by Penetrating Orbital Injury
한 결1⋅안 민1,2
Kyeol Han, MD1, Min Ahn, MD, PhD1,2
전북대학교 의학전문대학원 안과학교실1, 전북대학교 임상의학연구소-전북대학교병원 의생명연구원2 Department of Ophthalmology, Chonbuk National University Medical School1, Jeonju, Korea
Research Institute of Clinical Medicine of Chonbuk National University-Biomedical Research Institute of Chonbuk National University Hospital2, Jeonju, Korea
Purpose: We report a case of superior orbital fissure syndrome induced by penetrating orbital injury caused by a steel wire and analyzed the clinical outcomes.
Case summary: A 49-year-old female visited our clinic after a penetrating orbital injury through the right inferolateral conjunctiva caused by a steel wire. The best corrected visual acuity of the right eye was 0.8 and a fixed dilated pupil was detected. Partial ptosis and ophthalmoplegia were observed in the right eye. The computed tomography image revealed no sign of orbital wall fracture, retrobulbar hemorrhage or foreign body. Slightly increased signal intensity was observed on the magnetic resonance image but other abnormal findings of the extraocular muscle and optic nerve were not detected. Under the impression of superior orbital fissure syndrome, systemic steroid was administered orally. After 1 month, ptosis and ophthalmoplegia were partially improved. After 3 months, the pupil size and response were normalized.
Conclusions: The oral steroid treatment was given to reduce the edema without orbital wall fracture after the penetrating orbital injury, which caused the superior orbital fissure syndrome. The symptom was relieved 3 months after the injury.
J Korean Ophthalmol Soc 2015;56(4):592-597
Key Words: Penetrating orbital injury, Superior orbital fissure syndrome
■Received: 2014. 7. 11. ■ Revised: 2014. 12. 28.
■Accepted: 2015. 3. 7.
■Address reprint requests to Min Ahn, MD, PhD
Department of Ophthalmology, Chonbuk National University Hospital, #20 Geonji-ro, Deokjin-gu, Jeonju 561-712, Korea Tel: 82-63-250-1965, Fax: 82-63-250-1960
E-mail: [email protected]
* This study was presented as a narration at the 110th Annual Meeting of the Korean Ophthalmological Society 2013.
* This paper was supported by Fund of Biomedical Research Institute, Chonbuk National University Hospital.
ⓒ2015 The Korean Ophthalmological Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
상안와열은 외측으로 접형골의 큰날개, 내측으로 접형골 의 작은날개, 상측으로는 전두골로 이루어져 있고, 외직근 의 기시부인 진씨총건륜(annuls of Zinn)에 의해 두 부위로
나뉘는데 활차신경, 삼차신경의 첫 번째 분지와 상안와정 맥을 포함하는 상측과 동안신경, 외향신경, 코섬모체신경, 하안와정맥을 포함하는 하측으로 나뉜다.1
상안와열 증후군은 두개 및 안면부 외상 후 발생하는 드 문 합병증 중 하나이며, 외안근의 마비, 삼차신경 첫 번째 분지의 지배 영역의 감각이상, 구후 통증 등의 임상증상을 특징으로 한다.
상안와열증후군의 발생 원인으로는 상안와열을 통과하 는 구조물을 침범한 구후종양이나 구후염증과 중추신경계 감염, 해면정맥과 안와첨부위의 구후출혈 등이 있으며, 두 개 및 안면부 외상에서 두개골 골절, 안와골절, 협골상악골 복합골절, Le FortⅡ와 Le FortⅢ 골절 등으로 인해 직접 또 는 간접적으로 상안와열을 통과하는 구조물들이 손상되어
Figure 1. Ophthalmoplegia of the
right eye and partial ptosis of the right upper eyelid are noted at 1 hour after the injury.Figure 2. Injury site on the inferolateral side of right bulbar
conjunctiva (arrow).Figure 3. Axial (A) and coronal (B) CT scan at 1 hour after
injury. There is no sign of orbital wall fracture, retrobulbar hemorrhage or foreign body.발생한다.
안와관통상으로 인한 상안와열증후군의 경우는 보고된 바가 적으며, 이 중에서도 안와골절을 동반하지 않은 경우 는 더 드문 경우로, 안와골절이 없는 안와관통상으로 인한 상안와열증후군 1예와 그 회복과정을 경험하였기에 이를 문헌고찰과 함께 보고하고자 한다.
증례보고
49세 여자 환자가 내원 1시간 전 화초를 돌보던 중 30 cm 정도 길이의 가느다란 화분지지대 철심에 우안을 찔린 것을 주소로 내원하였다. 환자가 찔린 철심은 부러지지 않
았고 매우 깊이 찌르고 나왔다고 하였다.
초진 시 최대 교정시력은 우안 0.8, 좌안 1.0이었고, 우안 의 동공은 7 mm로 산대되어 있었고 고정되어 있었다. 안구 돌출계 검사상 우안 15 mm, 좌안 14 mm로 우안에서 약간 의 안구돌출이 있었고, 안와 잡음은 없었다. 우안의 margin-
A
B
Figure 5. Fields of gazes at three
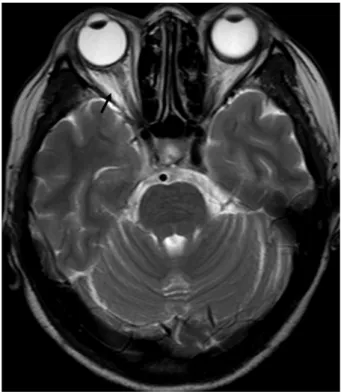
months after the injury show re- covery of the extraocular muscle movement in all directions. Ptosis of the right upper eyelid improved.Figure 4. Axial MRI (T2 weighted image) scan at 1 hour after
injury. Retrobulbar soft tissue of the right eye shows slightly increased signal intensity (arrow).al reflex distance 1 (MRD1)의 상안검하수와 우안의 전방향 에서 -3 이상의 안구운동 장애가 관찰되었고(Fig. 1), 전두 부와 우안의 상안검 주변 감각이상은 관찰되지 않았다. 세 극등현미경 검사에서 우안 하외측 결막부분으로 3 mm의 결막열상이 관찰되었다(Fig. 2). 안저검사 및 시야검사상 특
이소견은 없었다. 안와전산화단층촬영(computed tomog- raphy, CT) 검사상 안와골절, 구후출혈, 이물 등의 소견은 없 었으며(Fig. 3), 조영제를 사용한 안와자기공명영상(magnetic resonance image, MRI)에서 우안의 외직근 및 시신경의 이 상소견은 관찰되지 않았고, 눈 뒤쪽 안와 연부조직의 신호 강도가 약간 증가된 소견이 관찰되었다(Fig. 4). 병력과 이 학적 검진, 영상검사소견을 바탕으로 우안의 상안와열증후 군으로 진단하였다. 이후 환자는 예방적으로 항생제 경구 투약과 경구 스테로이드 치료를 시행하였다. 경구 스테로 이드 치료는 프레드니솔론(Prednisolone)을 7일간 1 mg/kg/day 을 투여하였고, 이후 7일 간격으로10 mg씩 감량하여 복용 하도록 하였다.
수상 후 1개월째 우안의 MRD1이 3으로 호전되었고, 안구 운동이 전방향에서 회복되었으나, 동공크기는 4 mm로 산대 된 채 대광반사의 경미한 지연을 보였다. 이후 수상 후 3개 월째 동공 크기와 동공 반응의 회복이 관찰되었다(Fig. 5).
고 찰
상안와열증후군은 안와외상의 드문 합병증으로 1858년 Hirschfeld2가 처음 보고하였다. 상안와열이 포함하는 구조 물들은 외직근의 기시부인 진씨총건륜(annuls of Zinn)에 의해 두 부위로 나뉘는데, 이중 총건륜 내에 위치하는 하측 구조물들은 두개 및 안면부외상시 뒤틀림 손상에 상대적으 로 더 취약하다고 알려졌다(Fig. 6).1,3 상안와열증후군의 임 상증상은 상안검의 하수, 안구운동마비, 약간의 안구돌출,
Figure 6. Diagrammatic representation of right superior orbi-
tal fissure with its contents (1. lacrimal nerve; 2. frontal nerve;3. trochlear nerve; 4. superior branch of ophthalmic vein; 5.
superior branch of oculomotor nerve; 6. nasociliary nerve; 7.
inferior branch of oculomotor nerve; 8. abducens nerve; 9. in- ferior branch of ophthalmic vein; 10. optic nerve; 11. oph- thalmic artery).
동공 산대와 조절마비, 전두부와 상안검부위의 지각마비 등 이다. 이 중 전두부와 상안검부위의 지각마비는 삼차신 경의 첫 번째 분지가 손상되거나 압박되어 나타나는 것으 로 삼차신경의 첫 번째 분지가 분포하는 부위의 지각마비 나 신경통증을 나타낼 수 있다.4
두개 및 안면부외상에 의한 상안와열증후군은 크게 골절 편의 전위로 인하여 직접적으로 상안와열을 통과하는 구조 물들에 압력을 가해 야기된 경우와 외상 후 발생한 조직의 부종, 혈종 등이 간접적으로 상안와열내의 압력을 증가시 켜 이를 통과하는 구조물들의 기능 장애를 초래하는 두 가 지 기전으로 나누어 볼 수 있다.5 본 증례는 안와골절 없이 심부 안와관통상에 의한 부종으로 인해 발생한 것으로 사 료되어 후자의 경우에 해당하는 것으로 보이며, 상안검과 전두부의 감각이상을 동반하지 않은 부분상안와열증후군 을 나타내었는데 이는 환자의 하외측 결막으로 관통된 철 심이 눈 뒤쪽으로 갈수록 총건륜의 위쪽으로 진행하지는 않아서 총건륜의 위쪽에 위치한 삼차신경의 첫 번째 분지 의 손상이 경미했다고 생각한다.
외상성 상안와열증후군의 치료에 대해서는 아직 명확히 정해진 바가 없으나, 안와전산화단층촬영 후 골절의 범위 와 모양에 따라 복합안면골절을 동반한 경우 골절정복수술 을 가능한 빨리 시행하여야 하며,6,7 골절편의 전위나 구후 혈종 등이 동반되어 상안와열과 안와첨이 현저히 좁아진 경우 감압술을 시행하여야 한다.4,8-10 골절편의 전위가 없는
선상골절인 경우에는 수술을 시행하지 않고 경과관찰과 보 존적 치료를 시행해볼 수 있으나,4,11 선상골절이거나 골절 이 없는 경우라도 진행하는 시신경 위축 소견이 동반될 때 는 안와첨에 대한 시험적 수술을 고려할 수 있다.12 상안와 열증후군에서 스테로이드 치료에 대해서는 용량과 방법이 정립되지 않았으나, 최근 연구에서는 스테로이드 치료의 일반적인 금기사항이 없는 한 조직의 부종을 감소시키기 위 해 단독 또는 수술 등의 다른 치료와 함께 사용하는 경향이 있다. Postma et al13은 외상성 상안와열증후군 환자에서 스테 로이드 단독 치료로 단기간의 덱사메타손(dexamethasone) 정맥투여를 시행하여 3개월만에 회복된 경과를 보고하였 고, 다른 연구에서는 골절정복수술 전, 후 덱사메타손 (dexamethasone)을 초기부하량 1 mg/kg 투여 후 0.5 mg/kg 으로 6시간마다 투여한 환자에서 그렇게 하지 않은 환자보 다 신경회복이 더 잘 이루어졌음을 보고한 바 있다.14 최근 Chen et al5은 33명의 외상성 상안와열증후군 환자에서 스 테로이드 치료를 병행한 경우와 병행하지 않은 경우에서 신경회복의 정도 차이가 없어 스테로이드의 역할이 불분명 하다고도 하였으나, 그럼에도 불구하고 스테로이드 치료가 외상성 상안와열증후군 환자에서 증상의 악화와 관계된 조 직의 부종을 감소시킨다는 부분에서 이점이 있으므로 스테 로이드 전신투여의 일반적인 금기사항이 없는 한 시행하는 것을 추천하였다. 최근 제안된 방법에는 메틸프레드니솔론 (methylprednisolone)을 초기 30 mg/kg의 용량으로 정맥주 사하고, 이후 15 mg/kg의 용량으로 6시간마다 3일간 정맥 주사 후 경구 스테로이드 치료로 전환하여 6개월까지 단계 적으로 감량하는 방법이 소개되기도 하였다.1,5 그러나 임상적 으로 외상성 상안와열증후군 및 눈 주변 신경손상 환자에서 고용량 스테로이드의 사용은 아직까지 논란의 여지가 있다. 외상성 상안와열증후군의 경우는 아니지만, International Optic Nerve Trauma Study (IONTS)는 133명의 외상성 시 신경 병증환자에서 경과관찰군, 스테로이드 치료군, 수술적 치료군 사이에 치료효과의 차이가 없다고 보고하였으며,15 다른 연구들에서는 고용량 스테로이드 정맥투여의 후 감염 의 위험성이 증가하거나 위장관 출혈 등의 심각한 부작용 이 발생할 수 있음을 보고하였다.16,17 본 증례에서는 외상성 상안와열증후군에서 스테로이드 치료 중 최근 제안된 방법 보다 저용량의 경구 스테로이드 치료를 시행하였는데, 본 증례의 경우 CT나 MRI와 같은 영상 검사에서 안와 및 두 개골의 골절이 없었으며 조직의 부종이 비교적 적었고, 수 상 후 1시간 뒤인 비교적 초기에 진단이 가능했던 경우로, 초기치료로 수상 부위의 염증과 부종을 감소시키기 위해 스테로이드 전신투여를 고려하였으며, 고용량 스테로이드 정맥 투여의 부작용을 감안하여 저용량 치료를 시행하였다.
Chung et al18은 외상성 상안와열증후군 1예를 보고하였 는데, 우안 상안검 내측에 약 5 cm 깊이의 관통상이 있었고 CT상 내직근의 파열이 의심되는 소견이 보였으며, 경구 스 테로이드 치료 후 안구운동이 수상 10일후 호전되기 시작 하여 1개월 후에는 상방주시를 제외한 모든 방향의 안구운 동과 안검하수가 호전되었고, 수상 3개월후 대광반사의 경 미한 지연을 제외한 모든 증상의 회복되었다고 보고하였다.
본 증례의 경우는 안검이 아닌 결막을 통한 관통상으로 육 안상 보이는 관통부위가 없었던 점과 진단 당시 전두부와 상안검 주변의 감각이상이 저명하지 않은 부분 상안와열증 후군 양상을 보였다는 점이 차이라 할 수 있고, 안구운동 및 안검하수가 먼저 호전되고 동공 반응이 3개월 이후 회 복되어 회복과정에서는 비슷한 순서를 보였으나, 외안근마 비의 전 방향에서의 회복이 수상 후 1개월째로 더 빨랐다.
기존에 국내에서 보고된 외상성 상안와열증후군의 다른 증 례들은 얼굴뼈 골절이 동반된 경우로 골절이 없이 안와 관 통상에 의해 발생한 본 증례와는 차이를 보인다.19,20
현재까지 상안와열증후군에서 스테로이드 치료에 대한 명확한 적응증이나 용량, 방법 등이 정해지지 않았고, 상안 와열증후군에서 전신 스테로이드의 치료에 대한 일치된 이 해가 없다. 따라서 추후 이에 대한 무작위 임상연구 등 관 련 연구가 필요할 것으로 생각한다.
REFERENCES
1) Chen CT, Chen YR. Traumatic superior orbital fissure syndrome:
current management. Craniomaxillofac Trauma Reconstr 2010;
3:9-16.
2) Hirschfeld L. Epanchement de sang dans le sinus caverneux du cote gauche diagnostique pendant la vie. Compt Rend Soc Biol 1858;138.
3) Rai S, Rattan V. Traumatic superior orbital fissure syndrome:
Review of literature and report of three cases. Natl J Maxillofac Surg 2012;3:222-5.
4) Zachariades N. The superior orbital fissure syndrome. Review of the literature and report of a case. Oral Surg Oral Med Oral Pathol 1982;53:237-40.
5) Chen CT, Wang TY, Tsay PK, et al. Traumatic superior orbital fis- sure syndrome: assessment of cranial nerve recovery in 33 cases.
Plast Reconstr Surg 2010;126:205-12.
6) Zachariades N, Vairaktaris E, Papavassiliou D, et al. The superior orbital fissure syndrome. J Maxillofac Surg 1985;13:125-8.
7) Antonyshyn O, Gruss JS, Kassel EE. Blow-in fractures of the orbit.
Plast Reconstr Surg 1989;84:10-20.
8) Sieverink NP, van der Wal KG. Superior orbital fissure syndrome in a 7-year-old boy. Int J Oral Surg 1980;9:216-20.
9) Robinson DC, Jarrett WJ. Superior orbital fissure syndrome with Bell's palsy: report of case. J Oral Surg 1973;31:203-6.
10) Unger JM, Gentry LR, Grossman JE. Sphenoid fractures: preva- lence, sites, and significance. Radiology 1990;175:175-80.
11) Pogrel MA. The superior orbital fissure syndrome: report of case. J Oral Surg 1980;38:215-7.
12) Bun RJ, Vissink A, Bos RR. Traumatic superior orbital fissure syn- drome: report of two cases. J Oral Maxillofac Surg 1996;54:
758-61.
13) Postma MP, Seldomridge GW, Vines FS. Superior orbital fissure syndrome and bilateral internal carotid pseudoaneurysms. J Oral Maxillofac Surg 1990;48:503-8.
14) Rohrich RJ, Hackney FL, Parikh RS. Superior orbital fissure syn- drome: current management concepts. J Craniomaxillofac Trauma 1995;1:44-8.
15) Levin LA, Beck RW, Joseph MP, et al. The treatment of traumatic optic neuropathy: the International Optic Nerve Trauma Study.
Ophthalmology 1999;106:1268-77.
16) Yip CC, Chng NW, Au Eong KG, et al. Low-dose intravenous methylprednisolone or conservative treatment in the management of traumatic optic neuropathy. Eur J Ophthalmol 2002;12:309-14.
17) Bracken MB, Shepard MJ, Holford TR, et al. Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury. Results of the Third National Acute Spinal Cord Injury Randomized Controlled Trial. National Acute Spinal Cord Injury Study. JAMA 1997;277:
1597-604.
18) Chung JW, Kim SJ, Lee SY, Lee EH. A case of superior orbital fis- sure syndrome. J Korean Ophthalmol Soc 2001;42:654-7.
19) Kim SG. Traumatic Superior orbital fissure syndrome complicat- ing fractures of the facial skeleton: Report of a Case. J Korean Assoc Maxillofac Plast Reconstr Surg 2000;22:356-9.
20) Kim YI, Paik UB, Kim JH, et al. Case report of traumatic orbital apex syndrome and superior orbital fissure syndrome. J Korean Assoc Maxillofac Plast Reconstr Surg 1994;15:275-80.
= 국문초록 =
안와관통상으로 인해 발생한 상안와열증후군 경과관찰 1예
목적: 화분 철심에 의한 안와관통상 후 발생한 상안와열증후군과 그 임상적 회복 과정 1예를 경험하였기에 보고하고자 한다.
증례요약: 화분 지지대 철심에 우안 하외측 결막으로 안와 관통상을 입은 49세 여자로 수상 1시간 뒤 본원 내원 당시 우안은 최대교정 시력이 0.8이었고 동공은 산대된 채 고정되어 있었다. 우안 상안검의 경한 안검하수와 전방향에서 안구운동장애를 보였으나, 전두부 와 우안 상안검 주변의 감각이상은 관찰되지 않았다. 안저검사 및 시야검사상 특이소견은 보이지 않았다. 안와전산화단층촬영에서 안와골절, 구후출혈, 이물 등의 소견은 보이지 않았다. 안와자기공명 영상에서는 눈 뒤쪽 안와 연부조직의 신호강도가 약간 증가된 소견 이외에 외안근이나 시신경의 특이소견은 관찰되지 않았다. 상안와열증후군으로 진단하고 스테로이드 경구치료 후 수상 1개월째 안검하수 및 안구운동장애의 호전과 동공반응의 일부 회복 소견이 보였고, 이후 수상 3개월째 동공반응의 완전 회복이 관찰되었다.
결론: 안와관통상 후 안와골절 없이 부종으로 인해 발생한 것으로 사료되는 상안와열증후군 환자에서 조직 부종을 경감시키는 목적으 로 경구 스테로이드 치료를 시행하였고, 수상 3개월 후 증상은 호전되었다.
<대한안과학회지 2015;56(4):592-597>