Geographic Difference in the Prevalence of Osteoporosis in Korea
Nam Han Cho, Chul Shin
1, Chan Park
2, Kyu Chan Kimm
2Department of Preventive Medicine, Ajou University School of Medicine, Suwon, Korea Department of Internal Medicine, Korea University College of Medicine, Ansan, Korea
1Korean National Genome Institute, Seoul, Korea
2목적: 지역사회 일반 인구 대상에서의 요골과 경골 골다공증 유병률 분석
방법: 본 연구는 전향성연구로 경기도 소재의 안성과 안산 지역에서 40~69세 남녀 총 10,038명 (남=4,762명, 여
=5,276명)을 대상으로 농촌-도시 지역의 골다공증 유병률을 분석하여 비교하였다. 골다공증 진단은 세계보건기구의 진단 기준에 따랐으며 경골과 요골에서의 골다공증 유병률을 분석 평가하였다. 골다공증 측정은 초음파방법을 사용 하였다.
결과: 농촌 지역인 안성 거주자들의 평균 연령은 55.5±8.8년, 도시 지역인 안산은 49.1±7.9년으로 농촌지역의 평균 연령이 높았다. 성별 분포는 도시의 경우 남녀가 50.3%, 49.7%으로 유사한 분포이며 안성은 여성이 55.4%였다. 체 질량지수는 농촌이 도시 지역에 비해 의미있게 높았다 (안성-24.7±3 kg/m
2, 안산-24.4±3.3 kg/m
2, P<0.01). 거주 기간은 41년 (안성)과 13년 (안산)으로 농촌에서의 거주 기간이 많았다. 혈압과 중성지방을 제외한 모든 검사 수치는 도시 지역에서 높게 분석되었다. 초음파를 사용한 평균 요골 SoS는 농촌 지역에서 높은 수치를 보인 반면 경골은 도시지역에서 높게 나타나는 현상을 보였다. 평균 초경 나이 역시 도시 지역에 비해 농촌 지역 여성에서 늦게 시작 되는 것으로 분석되었다 (16.1±0.9년, 15.6±2년, P<0.001). 하루 평균 칼슘 섭취량, 음주량, 커피, 탄산음료, 녹차 섭취량은 도시지역 여성들에서 높은 반면 농촌군에서는 흡연량이 높고 운동량은 적은 현상을 보였다. 남성에서는 지역적 차이가 없었다. 두지역간의 골다공증 유병률은 연령-성별-인구분포를 표준화된 방법으로 비교 분석하였다.
경골 골다공증의 경우 도시지역에서 11.4% (남=1.7%, 여=20.8%), 농촌 지역은 8.8% (남=2.2%, 여=15.1%)의 분포를 보여 도시 지역에서 유병률이 높게 나타났으나, 요골 골다공증은 도시지역 7.5% (남=3%, 여=11.9%), 농촌 지역 7.3% (남=3.3%, 여=11.1%)로 유사한 분포를 보였다. 다중로지스틱 회귀분석을 통해 성별, 나이, 체질량지수, 혈압을 보정할 경우 요골골다공증은 농촌지역이 도시지역에 비해 3.3배 (95% 신뢰구간 2.4~4.7, P<0.0001) 높은 것으로 분석되었다. 이러한 관계성은 경골에서도 농촌군에서 3.7배 (95% 신뢰구간 2.5~5.5, P<0.0001) 높은 것으로 분석 되었다.
결론: 요골, 경골 골다공증의 중요한 병인요소는 나이, 성별, 혈압, 체질량지수와 농촌 거주로 규명되었다. 특히 고위 험군으로 나타난 50대 이후 농촌 거주 여성들에서의 조속한 중재가 요구되고 있어 골다공증 조기 진단 및 관리가 체계적으로 이루어져야 할 것이다.
중심단어: 농촌-도시, 유병률, 골다공증, 대한민국, 전향성연구
책임저자 : 조남한, 아주대학교 의과대학 예방의학교실
Tel: 031)219-5900, Fax: 031)219-5901, E-mail: [email protected]
Rural and urban dwelling differ in the incidence of chronic disease such as coronary heart disease and some cancers
1~3. These differences might be direct and indirectly related to various environmental factors that one individual is exposed to long period of time.
However, it is very difficult for one to identify the specificrisk factors that are responsible for specific disease. Furthermore, most of chronic diseases are caused by the multiple risk factors. Therefore, in some disease, it is better to evaluated the risk factors as a whole e.g., environment, than try to identify the individual risk factors. Osteoporosis is the one of the key example disease in this matter because it is related to lifetime exposure to the risk factors. Osteo- porosis is a silence, systemic chronic disease that can affect different bones but usually not detected until the fracture of bone
4. Osteoporosis is the leading cause of serious morbidity and functional loss in the elderly population, and it results in 1.5 million fractures and over $10 billion in medical expenditures annually
5~8. Osteoporosis affects 28 million Ameri- cans and The National Osteoporosis Foundation estimates 1.5 times increases by year 2015. Medical communities are estimating that osteoporosis is likely to become the most common disorder of our aging population. Thus, understanding of factors that affect the incidence of osteoporosis is critical if we are to successfully minimize the impact of this disorder on morbidity, mortality, and the cost of health care.
Osteoporosis can result patho-genetically from inadequate peak bone mass, excessive bone resorption, or impaired bone formation. These can be affected by genetics, nutrition, lifestyle, systemic hormones, and local factors as well as residential factors. The relative importance of these mechanisms is not fully under- stood and may differ among subjects
9. However, osteoporosis is more common in women than men, especially postmenopausal women. In Kwang-ju city, Korea, the prevalence of osteoporosis and osteopenia according to decades showed a clear difference bet-
ween genders, the prevalence of osteoporosis over 50 years of age being about 3 times higher in women than men. In addition to gender, numerous epide- miologic studies reported that age is one of the most significant and independent risk factor for osteopo- rosis
10~12. However, there are still more risk factors are yet to be identified and understand its role for osteoporosis. For example, several studies reported geographic differences in the prevalence of osteo- porosis. The study from Japan indicated that serum vitamin K2 level difference are the reasons for the geographic differences within country
13, however, the European multinational study indicated that anthropo- metric variability are the reasons for geographic differences in the osteoporotic fracture
14.
Over 40% of adult peak bone mass is acquired during adolescence. During this period, in order to prevent bone loss the lifestyle choices including ensuring adequate dietary Ca, regular weight-bearing exercise and avoiding hormonal insufficiency, are especially important
15. Therefore, both adequate nutri- tion and exercise are essential for development of peak adult bone mass and maintenance of bone during aging. The optimal dietary level of a nutrient may vary from individual to individual and may change with age, intake of other nutrients, disease, drug therapy, or sex hormone status
16. Therefore, for better understanding of osteoporosis it is important to eva- luate whether these factors are present independent of geographic variations.
It is very clear that the prevalence of osteoporosis in Korea steadily increased with an economic develop- ment of the nation. Therefore, in order to implement an effective prevention or intervention strategy for osteoporosis, understand the lifetime bone health such as changing pattern and magnitude is very essential.
However, it is very difficult to assess the life time
bone health pattern because of difficulty of measure-
ment, cost, especially in normal community popu-
lation. Thus, in this study we under took the issue by
using a non-invasive bone quality measuring instru- ment at the multiple bone sites and we investigated au urbanization as the risk factor for osteoporosis and conducted comparative study between the urban and rural area in a large scale community based epide- miologic study in Korea.
Methods 1. Study population
Two communities in South Korea were selected;
the Ansungcohort represented a rural community, and the Ansan cohort an urban community. Both commu- nities were selected for the Korean Health and Genome Study (KHGS) in 2001. Ansung is a far- mland with 90% of participants is involved rice farming, pear or grape orchard, and dairy farming.
Ansan is a mid-size industrial city with 60% of them working as either blue or white collar type of works.
This is an ongoing prospective study involving a biennial examination. Details of the KHGS and the method used have been previously described
17. In brief, a total of 10,038 subjects aged from 40 to 69 years were recruited (5,018 from a farming commu- nity, Ansung and 5,020 from an industrial community, Ansan). Of these 10,038 subjects, 5,018 Ansung sub- jects were recruited from a 5 out 11 Myon (lowest governing district) by cluster sampling method. For Ansan, a total of 5,020 subjects were recruited via Systematic Random Sampling method using the telephone directory. A total recruitment rate was about 80%. The study protocol was approved by the Ethics Committee of the Korean Heath and Genomic Study of the Korean National Institute of Health.
2. Measurement of anthropometric and bio- chemical parameters
Height, body weight, waist and hip circumference
were measured standard method in light clothes. Body mass index (BMI) was calculated as weight divided by height squared (kg/m
2). Body fat and lean body mass were measured by tetrapolar bioelectrical impedance analysis (Inbody 3.0
Ⓡ, Biospace, Korea).
Bioelectrical impedance analysis measures two para- meters, fat and lean tissue, using empirically derived formulas that have been validated by earlier studies, and which were found to correlate well with under- water weighing, except for extremely obese sub- jects
18,19.
The morning blood pressure was recorded three times between 7 and 9 am, after subjects had been in a relaxed state for at least 10 minutes, 5 minutes resting period was given between the each measure- ment. After 8~14 hours overnight fasting, plasma concentrations of glucose, insulin, total cholesterol, triglyceride, and HDL-cholesterol were measured enzymatically using a Hitachi 747 chemistry analyzer (Hitachi, Tokyo, Japan). The level of LDL-cholesterol (mmol/l) was calculated by using the following formula: [total cholesterol (mmol/l) - HDL-cholesterol (mmol/l) - triglyceride (mmol/l)/2.2)]
20.
Smoking status was divided into never smoker, ex-smoker, and current smoker (ie., <1 pack/day and
≥ 1 pack/day). The term “never” means the person who never smoked in his or her life time and “ever”
was used to classify the person who had smoked for at least one month or currently smokes. Responses to frequency questionnaire were obtained alcohol con- sumption, coffee intake, carbonated beverages consump- tion, dairy products intake and physical exercise.
Alcohol consumption was calculated at total amount of alcohol consumption by 52 weeks. Alcohol amount according to kind of alcoholic beverages was calcu- lated alcohol amount per glass. At each alcoholic beverages record Total periods of alcohol consump- tion, alcohol consumption times per month and number of glasses of alcoholic beveragesper time.
And alcohol consumption was divided into none
drinker, <=100 g and 100 g< groups. At each age the response was scored on a 4-point scale in Coffee, Green tea, and carbonated beverages frequency:
0:none, 1:13 times per month, 2:1 time per day, 3:
1~4 times per week, 4: >5 times per week. Alcohol intake amount was calculated by ‘kcal' of each kind of liquor per a week (i.e., grain alcohol=90 kcal, beer=100 kcal, wine=50 kcal, whisky=140 kcal, rice wine=100 kcal).
3. SoS Measurement
To measure the bone health, we used the Omni- sense 7000S (Sunlight Ultrasound Technologies, Rehovet, Israel). Omnisense is designed to measure Speed of Sound (SoS) for by ultrasonic waves axially trans- mitted along bonesand recorded in meter per seconds.
The two sites were measured using the special probes according to DR (Distal Radius) and MT (Midshaft Tibia). Omnisense SoS measurement consists of per- forming three measurement cycles of SoS recording while scanning tangentially the no dominant limb using a probe coupled by an acoustic gel. The two evaluation sites were the distal radius and midshaft tibia. The DR was measured by marking the half- length of the arm from elbow to the outstretched index finger, and by positioning the probe distally next to the mark. The Tibia was measured using DR by marking the half-length of Tibia from knee to the heel, and by positioning the probe distally next to the mark. The BMD was graded according to the categories of kanis et al. Kanis et al. defined normal bone as having a BMD higher than -1 SD, osteopenia as a BMD between -1 and -2.5 SD, osteoporosis as less than -2.5 SD
21.
4. Statistics
Statistical analyses were performed using SPSS Windows version 12 (Chicago, U.S.A). To test SoS
and cofactors association t-test and Multiple Logistic Regression Models were used. The Standardized Mor- tality Rate (SMR) adjusted for general population was calculated to make a direct comparison between the two studies sites. All tests were two tailed and p values <0.05 was considered as statistical significant.
Data are presented as mean±standard deviation (SD).
Results
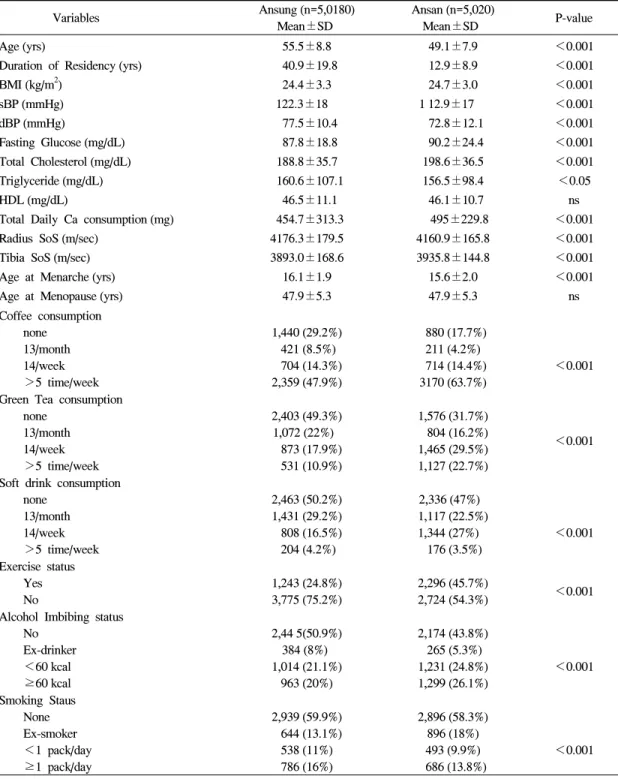
We recruited 10,038 subjects from the two com- munity population; 5,020 urban subjects and 5,018 rural. Demographic characteristics are shown in Table 1. The mean age of the rural subject was 55.5±8.8 that is significantly older in the urban (P<0.001);
mean age in the urban was 49.1±7.9. Gender distri- bution for urban was very similar (male 50.3% vs female 49.7%) but higher proportionof female subjects (55.4%) was seen in rural area. As shown in table 1, we found significant differences in the many demo- graphic characteristics between the two groups. BMI was significantly higher in the urban (24.7±3 kg/m
2) than rural region (24.4±3.3 kg/m
2)(P<0.01). Mean duration of residence was significantly longer in rural than urban indicating that urban population of more dynamic characteristics. However, other that blood pressures and triglyceride, all other metabolic vari- ables were significantly higher in urban population.
Mean SoS for radius was higher in rural but tibia value was greater in urban population. Mean age at menarche was significantly older in the rural region (16.1±1.9 years) and urban region (15.6±2 years) (P
<0.001). However, menopause age was not statis-
tically significant different in the two geographic
regions; rural region was 47.9±5.3 years and urban
47.9±5.3 years. Amount of daily calcium intake was
greater in urban population. We also evaluated life
style factors such as drinking habit, smoking and
exercise. There were more urban people drinking and
amount of alcohol intake was also significantly higher
Table 1. Demographic characteristics
Variables Ansung (n=5,0180) Mean±SD
Ansan (n=5,020)
Mean±SD P-value
Age (yrs)
Duration of Residency (yrs) BMI (kg/m2)
sBP (mmHg) dBP (mmHg)
Fasting Glucose (mg/dL) Total Cholesterol (mg/dL) Triglyceride (mg/dL) HDL (mg/dL)
Total Daily Ca consumption (mg) Radius SoS (m/sec)
Tibia SoS (m/sec) Age at Menarche (yrs) Age at Menopause (yrs)
55.5±8.8 40.9±19.8
24.4±3.3 122.3±18
77.5±10.4 87.8±18.8 188.8±35.7 160.6±107.1
46.5±11.1 454.7±313.3 4176.3±179.5 3893.0±168.6
16.1±1.9 47.9±5.3
49.1±7.9 12.9±8.9 24.7±3.0 1 12.9±17
72.8±12.1 90.2±24.4 198.6±36.5 156.5±98.4 46.1±10.7 495±229.8 4160.9±165.8 3935.8±144.8
15.6±2.0 47.9±5.3
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
<0.05 ns
<0.001
<0.001
<0.001
<0.001 ns Coffee consumption
none 13/month 14/week >5 time/week
1,440 (29.2%) 421 (8.5%) 704 (14.3%) 2,359 (47.9%)
880 (17.7%) 211 (4.2%) 714 (14.4%) 3170 (63.7%)
<0.001
Green Tea consumption none
13/month 14/week >5 time/week
2,403 (49.3%) 1,072 (22%)
873 (17.9%) 531 (10.9%)
1,576 (31.7%) 804 (16.2%) 1,465 (29.5%) 1,127 (22.7%)
<0.001
Soft drink consumption none
13/month 14/week >5 time/week
2,463 (50.2%) 1,431 (29.2%) 808 (16.5%) 204 (4.2%)
2,336 (47%) 1,117 (22.5%) 1,344 (27%)
176 (3.5%)
<0.001
Exercise status Yes No
1,243 (24.8%) 3,775 (75.2%)
2,296 (45.7%)
2,724 (54.3%) <0.001
Alcohol Imbibing status No
Ex-drinker <60 kcal ≥60 kcal
2,44 5(50.9%) 384 (8%)
1,014 (21.1%) 963 (20%)
2,174 (43.8%) 265 (5.3%) 1,231 (24.8%) 1,299 (26.1%)
<0.001
Smoking Staus None Ex-smoker <1 pack/day ≥1 pack/day
2,939 (59.9%) 644 (13.1%) 538 (11%) 786 (16%)
2,896 (58.3%) 896 (18%) 493 (9.9%) 686 (13.8%)
<0.001
in the rural area. Coffee intake, carbonated drink, and green tea consumption was also greater in rural area.
There were more smokers but lesser exercise in rural
area. It was very clear that demographic characteristic between the two regions were significantly different.
Since we found significant differences in the mean
Table 2. Crude rates at tibial
Age Group Sex Ansung Ansan
Osteoporosis n Age-Specific rate Osteoporosis n Age-Specific rate
40~49 M 7 689 0.01 23 1,590 0.014
F 67 856 0.078 54 1,331 0.041
50~59 M 14 658 0.021 8 527 0.015
F 193 788 0.245 91 521 0.175
60~69 M 25 875 0.029 14 272 0.051
F 458 1,101 0.416 130 382 0.34
Total
M 46 2,222 0.021 45 2,389 0.019
F 718 2,745 0.262 275 2,234 0.123
All 764 4,967 0.154 320 4,623 0.069
Table 3. Standardized mortality rate by direct adjustment for tibia
Age Group SexAnsung Ansan
Population Age-Specific rate
Estimated
Cases Population Age-Specific rate
Estimated Cases 40~49 M 3,487,210 0.01 34,872 3,487,210 0.014 48,821
F 3,411,518 0.078 266,098 3,411,518 0.041 139,872
50~59 M 2,127,806 0.021 44,683 2,127,806 0.015 31,917
F 2,167,404 0.245 531,013 2,167,404 0.175 379,296
60~69 M 1,422,761 0.029 41,260 1,422,761 0.051 72,561
F 1,729,127 0.416 719,317 1,729,127 0.340 587,903
Total
M 7,037,777 0.017 120,815 7,037,777 0.022 153,299
F 7,308,049 0.208 1,516,428 7,308,049 0.151 1,107,071
All 14,345,826 0.114 1,637,243 14,345,826 0.088 1,260,370
Radius and Tibia SoS lever, we compared prevalence of osteoporosis separately. The crude rate of Tibia osteoporosis for rural area was 15.4% (male=2.1%, female=26.2%), and for urban of 6.9% (male=1.9%, female=12.3%) (Table 2). We found similar rates in male but more than two fold higher female rates were seen in rural area. Moreover, when the rates were further stratified by the age groups (ie., 40, 50, and 60
th), we found clear pattern of a linear increments in female subjects. However, increment patterns are milder in male subjects. In females, the magnitude of rates changes was greater in tibia than radius in both regions. The changing patterns clear show a strong
age effects on the prevalence of both tibia and radius
osteoporosis (Tables 2 and 4). There was an evidence
of significant age and gender distribution between the
two regions; we found more female and older subjects
(≥60 years) been recruited in the rural area than
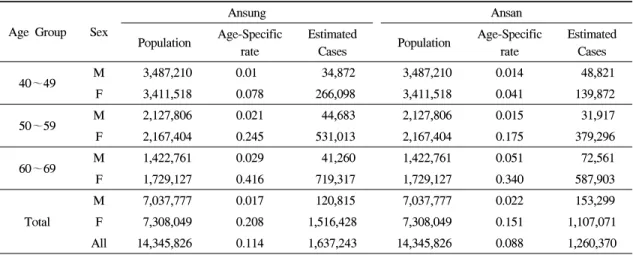
urban. Therefore, we calculated standardized mortality
rates (SMR) by using the direct adjustment to make
direct comparison between the two regions. A shown
in table 3, we found 1.3 times higher rates in urban
male, but 1.4 times higher in rural females. However,
the direct adjustment reduced the rate differences
significantly but still showing 1.3 time higher osteo-
porosis rates in rural population.
Table 4. Crude rates at radius
Age Group Sex Ansung Ansan
Osteoporosis n Age-Specific rate Osteoporosis n Age-Specific rate
40~49 M 8 686 0.012 19 1,592 0.012
F 6 855 0.007 4 1,338 0.003
50~59 M 14 655 0.021 23 528 0.044
F 51 776 0.066 48 526 0.091
60~69 M 25 865 0.029 15 271 0.055
F 158 1,062 0.149 105 381 0.276
Total
M 47 2,693 0.017 57 2,391 0.024
F 215 2,206 0.097 157 2,245 0.07
All 262 4,899 0.053 214 4,636 0.046
Table 5. Standardized mortality rate by direct adjustment for radius
Age Group SexAnsung Ansan
Population Age-Specific rate
Estimated
Cases Population Age-Specific rate
Estimated Cases
40~49 M 3,487,210 0.012 41,847 3,487,210 0.012 41,847
F 3,411,518 0.007 23,881 3,411,518 0.003 10,235
50~59 M 2,127,806 0.021 44,684 2,127,806 0.044 93,623
F 2,167,404 0.066 531,013 2,167,404 0.091 379,296
60~69 M 1,422,761 0.029 143,049 1,422,761 0.055 78,252
F 1,729,127 0.149 257,640 1,729,127 0.276 477,239
Total
M 7,037,777 0.033 229,580 7,037,777 0.03 213,722
F 7,308,049 0.111 812,534 7,308,049 0.119 866,770
All 14,345,826 0.0726 1,042,114 14,345,826 0.075 1,080,492
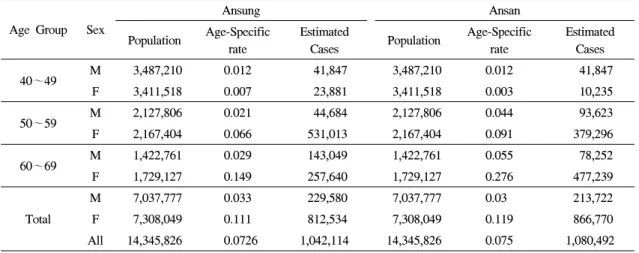
Table 4 shows an overall crude prevalence of radius osteoporosis in the urban was 4.6% and rural with 5.3%. We also observed gender differences, higher rates in urban male (2.4 vs 1.7%) but lower in female
(7% vs 9.7%). However, when SMR was calculated by direct method, differences in both genders were narrowed and found very similar rates, and geographic difference was observed only at tibia.
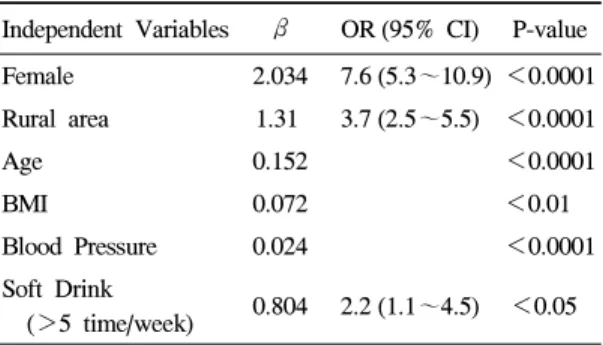
We further evaluated effect of residency on preva- lence of osteoporosis independent of other putative risk factors using multiple logistic regression models.
we found that population living in rural area was 3.3 times (95% CI 2.4~4.7, P<0.0001) higher risk for
osteoporosis at radius when compared to urban living (Table 6). This relationship existed independent of female gender, age, BMI and blood pressures. Female gender was the strongest independent risk factor for radius osteoporosis. When compared with male gender females are 9.6 time (95% CI 7~13, P<0.0001) at greater risk for radius osteoporosis. Furthermore, these relationship also persisted at tibia with 3.7 times (95%
CI 2.5~5.5, P<0.0001) higher risk been living in
Rural area. Similar independent variables were
included in the model along carbonated drink more
than 5 times per week. Female gender was one of the
strongest independent risk factor for tibia osteoporosis.
Table 6. Multiple logistic regression model for tibia
Independent Variables β OR (95% CI) P-value Female 2.034 7.6 (5.3~10.9) <0.0001 Rural area 1.31 3.7 (2.5~5.5) <0.0001Age 0.152 <0.0001
BMI 0.072 <0.01
Blood Pressure 0.024 <0.0001
Soft Drink
(>5 time/week) 0.804 2.2 (1.1~4.5) <0.05
Table 7. Multiple logistic regression model for radius
Independent Variables β OR (95% CI) P-valueFemale 2.264 9.6 (7~13) <0.0001
Rural area 1.21 3.3 (2.4~4.7) <0.0001
Age 0.156 <0.0001
BMI 0.064 <0.01
Blood Pressure 0.022 <0.0001