Introduction
Postural control is defined as the ability to attain and to maintain the body segments in space.
Children with cerebral palsy (CP) have an impaired postural control system, which impacts postural mo- tor coordination, musculoskeletal system, and sensory organization (Dewar et al, 2015). Postural control dysfunction is caused by poor muscle recruitment and agonist-antagonist muscle coactivation (Schmit et al, 2015). This dysfunction results in falling, limi- tations in functional activities, and gross motor skills during voluntary movement (Ju et al, 2010). Postural control in children with CP plays an important role in recovery balance during perturbation, skillful per- formance, confidence, participation, and social inter-
action compared with typically developing children (Imms, 2008). Due to the importance of postural con- trol, many researchers have emphasized that postural balance training might be necessary for CP to recruit the postural muscles (i.e. abdominal and spinal mus- cles) (Geldhof et al, 2006; Shumway-Cook et al, 2003; Woollacott et al, 2005). Therapeutic inter- ventions for improving postural control in children with CP have investigated extensively such as gross motor exercises (Katz-Leurer et al, 2009), functional electrical stimulation (Karabay et al, 2012), and hip- potherapy (Zadnikar and Kastrin, 2011). Recently, re- searchers have been suggested reactive balance training using perturbation (El-Shamy and Abd El Kafy, 2014) and trunk-targeted training on vibrating board (Unger et al, 2013).
Corresponding author: Chung-hwi Yi [email protected]
Trunk Stabilization Exercise Using a Both Sides Utilized Ball in Children With Spastic Diplegia: Case Study
Yon-ju Sim1,2, MSc, PT, Jeong-soo Kim3, PhD, PT, Chung-hwi Yi4,5, PhD, PT, Heon-seock Cynn4,5, PhD, PT
1Dept. of Rehabilitation Medicine, Wonju Medical Center
2Dept. of Physical Therapy, The Graduate School, Yonsei University
3Dept. of Physical Therapy, Seoul Rehabilitation Hospital
4Dept. of Physical Therapy, College of Health Science, Yonsei University
5Dept. of Ergonomic Therapy, The Graduate School of Health and Environment, Yonsei University
Abstract
1)This study examined the effects of trunk stabilization exercise on balance and trunk control in children with spastic diplegia. Four children with ambulatory spastic diplegia participated in the trunk stabilization exercise program using a Both Sides Utilized (BOSU) ball, 30 minutes a day, two times a week for eight weeks. Outcome variables included the pediatric balance scale, trunk control movement scale and multifidus thickness using ultrasound image. After trunk stabilization exercise, there was statistically no significant improvement in pediatric balance scale, trunk control movement scale and multifidus thickness.
However, individual outcomes were observed with some positive changes. Balance, trunk control movement, and thickness of multifidus were found to be improved. Trunk stabilization exercise using a BOSU ball could improve trunk control and increase the thickness of multifidus in children with spastic diplegia. Further investigation is needed to evaluate subjects according to type of cerebral palsy and to understand the relationship between postural control and gait.
Key Words: Balance; Cerebral palsy; Multifidus; Postural control; Trunk stabilization.
The trunk organizes postural stability or balance at the center of our body (Dewar et al, 2015). The trunk provides a stable ground while moving the up- per and lower limbs, also leading to active partic- ipation during sitting, activities of daily living, reach- ing, and walking (Prosser et al, 2010; Saavedra et al, 2009). Trunk stability is an essential component of movement for performing all activities of daily living (De Kegel et al, 2012). Trunk stabilization is ach- ieved by co-contraction of global muscle, and local muscle improves the stability of the spine and trunk through trunk muscle strengthening. Multifidus, as a deep trunk stabilizer controls and stabilizes the trunk during segmental and rotational movements (Panjabi, 2003). Weakness of trunk musculature and poorer balance were associated with falls, as well as greater restriction of activities such as reaching and walking (Dewar et al, 2015). Thus there is a need for a trunk stabilization exercise and also a carry-over ef- fect on functional balance (Unger et al, 2013). In a previous study, exercises performed on unsupported surface increase core muscle activation and limb muscle activation. And the trunk muscle exercises performed on a physio ball are more effective than those performed on the plinth in improving both trunk control and functional balance in acute stroke patients (Karthikbabu et al, 2011). However, there has been limited study targeting trunk muscle di- rectly for postural control in CP.
The Both Sides Utilized Balance Trainer (BOSU;
BOSU Balance Trainer, Fitness Quest, OH, USA) is the hemisphere-shaped and is an instrument for bal- ance training, core stability exercises, and proprio- ceptive training. The design of the BOSU provides a solid plastic base integrated with an inflatable rubber bladder that resembles a halved physio ball.
Therefore, the BOSU has a solid surface facing down that provides a stable surface compared with a physio ball (Yaggie and Campbell, 2006). Several studies have found that exercises using BOSU en- hance balance, trunk stability, and proprioceptive control (Romero-Franco et al, 2012; Yaggie and
Campbell, 2006). Most of these studies have re- searched subjects with uninjured population.
The purpose of this research was to investigate the effects of trunk stabilization exercise using a BOSU ball on balance and postural control among children with spastic diplegia (SD). We hypothesized that the trunk stabilization exercise on BOSU ball improves balance, postural control and the thickness of multifidus among children with SD.
Methods
Subjects
Four children with SD (4 males, mean age=12.3 years) participated in this study. Inclusion criteria were 1) able to sit without trunk support, and 2) Gross Motor Function Classification System (GMFCS) level Ⅰ or Ⅱ. Modified Ashworth Scale 0∼2. Exclusion criteria were 1) visual disorder, 2) cognitive disorder, 3) orthopedic intervention and 4) botulinum toxin in- jections performed in the last one year. Children and their legal guidances were provided a consent form prior to this study.
Child one was an 11 year-old male with GMFCS
Ⅰ, delivered by normal spontaneous vaginal delivery after a 32-week gestation. The cause of CP was cerebral hemorrhage. Child two was a 13 year-old male with GMFCS Ⅱ, delivered by cesarean section after a 28-week gestation. The cause of CP was al- coholic fetus during his mother’s pregnancy. Child three was a 12 year-old male with GMFCS Ⅰ, de- livered by cesarean section after a 32-week gestation. The cause of CP was viral meningitis.
Child four was a 13 year-old male with GMFCS Ⅱ, delivered by normal spontaneous vaginal delivery af- ter a 29-week gestation. The cause of CP was hy- poxemia for dystocia. The characteristics of subjects are presented in Table 1.
Pediatric balance scale
Pediatric Balance Scale (PBS) is a clinical meas-
urement tool for balance ability in the school-age children with motor impairments. The PBS examines 14 items, which can be administered quickly and easily without specialized facility. According to the extent of independence, scores are ranked from 0 to 4 points. The PBS score ranges from a minimum of 0 to a maximum of 56. The PBS has good test-re- test intra-class correlation coefficient [ICC(2,1)=.923]
and inter-rater reliability [ICC(2,1)=.972] (Franjoine et al, 2010).
Trunk control movement scale
Trunk Control Movement Scale (TCMS) is stem- med from the Trunk Impairment Scale. The TCMS examines 15 items, which evaluates trunk control with spastic CP, GMFCS levels Ⅰ∼Ⅴ, and aged 8 and 15 years. The TCMS measures static/dynamic sitting balance, selective movement control, and dy- namic reaching. The total TCMS score ranges from 0 to 58. A higher score indicates the ability of the child to perform better (Heyrman et al, 2013). ICCs ranged from .91 to .99 for inter-rater and test-retest reliability (Heyrman et al, 2011).
Ultrasound image measurement
The Philips iU22 Ultrasound (Philips Co. Ltd, WA, USA) application with a 50 ㎜, C 5-1 ㎒ curvilinear transducer is used to evaluate muscle thickness. The image view is an excellent and noninvasive method.
The child lay prone with folded towels under the pelvis to eliminate lumbar lordosis (Figure 1). The fourth lumbar spinous process (L4) was identified using the iliac crest as a landmark and confirmed using ultrasound imaging by viewing the spinous processes relative to the sacrum in sagittal section.
L4 was marked with a pen. The transducer was first placed longitudinally over the midline of the L4 spi- nous process and then moved laterally and angled medially to identify zygapophyseal joints. Multifidus thickness was defined as the distance from the zyg- apophyseal joints landmark to the inner edge of the fascia between the multifidus and superficial tissue at rest (Kiesel et al, 2007) (Figure 2). Image acquis- itions from each child were measured in three trials and averaged. This method had good intrarater reli- ability [ICC(3,3)=.83∼.99] and interrater reliability [ICC(2,3)=.93∼.99] in adolescents (Zapata et al, 2015).
Subjects Gender Age (year) Height (㎝) Weight (㎏) MASa GMFCSb level
Child 1 Male 11 141.0 45.0 G0 Ⅰ
Child 2 Male 13 136.0 28.0 G1 Ⅱ
Child 3 Male 12 142.0 35.0 G0 Ⅰ
Child 4 Male 13 140.0 37.6 G1+ Ⅱ
amodified Ashworth scale, bgross motor function classification system.
Table 1. Characteristics of the subjects (N=4)
Figure 1. Ultrasound imaging set up. Figure 2. Multifidus thickness at L4.
Experimental procedures
Each child received 30 minutes of trunk stabiliza- tion exercise a day, two days a week for eight weeks (i.e. a total of 16 sessions). The exercises were composed of 3 sets repeated 10 times for each session. The exercises were performed after taking off the orthosis. The children received trunk stabili- zation exercises in supine position and prone position.
The supine exercises involved “hollowing” the ab- dominals and pelvic bridge. The prone exercises in- cluded quadripedal, bird dog exercise, semi-plank po- sition, or plank position. The exercises were guided with moderate assistance and then carried out with- out assistance. The outcomes were measured before and after intervention.
Trunk stabilization exercise
The supine exercises consist of: 1) the child lying supine with knee flexion on the solid bottom side pull in abdominals toward the back, 2) the child flexing the knees and placing the feet on the dome and then lifting the pelvic off the floor. The prone exercises consist of: 1) the child performing 4-point weight on hands and knees on the dome; 2) the child kneeling with the hands on the floor and the knee on the dome to execute reaching forward with unilateral arm above shoulder level and then lifting
the leg alternatively; 3) the child being asked to pose in semi-plank position or plank position and keeping the hands extended to the solid bottom side of the BOSU ball; 4) the child’s trunk flexed to one side in semi-plank position (Figure 3).
Statistical analysis
Data were analyzed using the SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA). A Wilcoxon sign- ed-rank test was used to compare the differences pre- and post-test measurements within a group.
Statistical significance was set at p<.05. In addition, to assess the difference in each child, percent changes from pre-test to post-test were calculated [improvement (%)=(posttest-pretest)/pretest×100].
Results
There were no significant differences in the PBS, TCMS, and multifidus thickness (p>.05) (Table 2).
However, when regarding the percent changes for each child, some positive changes were observed. All children showed improvements in their total percent- age score on the PBS and TCMS. Results of the PBS and TCMS for each child are presented in Table 3. Three of four children showed improve-
A B C D
E F G H
Figure 3. Trunk stabilization exercise (A: hollowing exercise, B: bridge exercise, C: quadripedal, D:
bird-dog exercise 1, E: bird-dog exercise 2, F: plank exercise, G: semi-plank exercise, H: lateral flexion with semi-plank exercise).
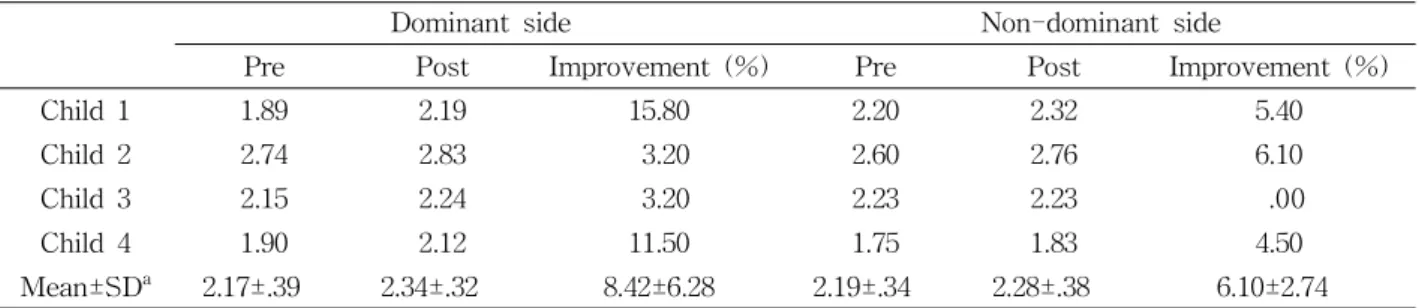
ments of multifidus thickness both on the dominant and non-dominant side. Child three showed improve- ment in multifidus thickness at dominant side.
Results of the multifidus thickness are presented in Table 4.
Discussion
In this study, the effects of trunk stabilization ex- ercise using a BOSU ball were examined in children with SD. The results of our study were statistically no significant difference in trunk control and the multifidus thickness in children with SD. The PBS
score did not show a significant difference, but the changes of the PBS score indicate clinically mean- ingful change. The children showed improvement in standing with one leg, placing interchanging foot on stool, and regaining an object from the floor. Balance control demands the displacement of the center of gravity in various bases of support and skillful coor- dinated movement.
Thus, trunk stabilization exercise using BOSU ball is effective for functional activities that require pos- tural control. The TCMS score did not show a sig- nificant difference, but the changes of the TCMS score showed a marked performance in lateral short- ening and lengthening of the trunk. In a previous
Pre Post p
PBSa (score) 41.25±6.65b 43.75±7.41 .68
TCMSc (score) 37.50±4.43 43.50±5.06 .66
Multifidus thickness at dominant side 2.17±.39 2.34±.32 .66
Multifidus thickness at non-dominant side 2.19±.34 2.28±.38 .14
apediatric balance score, bmean±standard deviation, ctrunk control measurement scale, p values are the results of Wilcoxon signed-rank test.
Table 2. Results of the PBS, TCMS, and multifidus thickness (N=4)
PBSa TCMSb
Pre Post Improvement (%) Pre Post Improvement (%)
Child 1 49 52 6.12 39 47 21.60
Child 2 40 44 10.00 39 45 15.38
Child 3 43 45 4.65 41 46 12.19
Child 4 33 35 6.00 31 36 16.12
Mean±SDc 41.25±6.65 44.00±6.97 6.69±2.30 37.50±4.43 43.50±5.06 16.32±3.90
apediatric balance score, btrunk control measurement scale, cmean±standard deviation.
Table 3. Pre- and post-test scores of PBS and TCMS
Dominant side Non-dominant side
Pre Post Improvement (%) Pre Post Improvement (%)
Child 1 1.89 2.19 15.80 2.20 2.32 5.40
Child 2 2.74 2.83 3.20 2.60 2.76 6.10
Child 3 2.15 2.24 3.20 2.23 2.23 .00
Child 4 1.90 2.12 11.50 1.75 1.83 4.50
Mean±SDa 2.17±.39 2.34±.32 8.42±6.28 2.19±.34 2.28±.38 6.10±2.74
amean±standard deviation.
Table 4. Pre- and post-test changes of the multifidus thickness (Unit=㎝)
study, trunk strengthening exercises proposed the ef- fect of perturbation that improves anticipatory pos- tural adjustments (Unger et al, 2013). Trunk stabili- zation exercise on BOSU ball stimulates sensory re- ceptors and arouses efficient trunk muscle activation (Lephart et al, 1997). There was no significant in- crease in multifidus thickness at dominant side, but all children showed a slight increase after intervention.
These results may presuppose that the deep muscle of the dominant side is more recruited during stabilization exercise, and the activation effect of deep muscle of dominant side is more exaggerated using the BOSU ball. Trunk stability requires a complex integration of the spinal segment, local and global spinal musculature, and neural mecha- nism (Hibbs et al, 2008).
In this study, the selected exercises were designed to activate and strengthen the core muscles and in- cluded both isometric and isotonic activities. The trunk muscle exercises using a physio ball are gen- erally used in clinics for adult patients (Karthikbabu et al, 2011). However, stabilization exercises on a physio ball among children with CP have several flaws, such as being too challenging and effecting undesirable movements (Cherng et al, 2004). The re- sults of our study show that stabilization exercises for the trunk muscle using the BOSU are more ef- fective than the physio ball and are suitable for SD.
The results of this study suggest that clinicians should consider the trunk stabilization exercises dur- ing the rehabilitation of children with CP. It should be included in combination with conventional treat- ment programs. The results also recommended using BOSU ball as an efficient balance training program for improving balance performance in these children.
There are some limitations in this study. First, the impact of the trunk stabilization exercise program using the BOSU on spasticity and functional motor skills such as gait was not investigated in this study. Second, for limitation of experimental design, we did not measure follow-up data. The continuous effect of the intervention was also not explored in
this study. Finally, other abdominal core muscles ex- cept multifidus muscle were not measured in this study. Future work needs to target different types of CP, different age intervals, and a large sample of children with CP to provide more generalization.
Trunk stabilization exercise using the BOSU is con- sidered to improve trunk control and increase muscle thickness in multifidus among children with SD.
Conclusion
This study investigated the effects of trunk stabi- lization exercise using BOSU ball in four children with SD. The four children showed small but poten- tially important changes in balance, trunk control, and thickness of multifidus after intervention. The findings suggest that trunk stabilization exercise us- ing BOSU ball may be promising for some children with CP. Although generalizations cannot be made to a large sample of children with CP, trunk stabiliza- tion exercise using BOSU ball may be considered by clinicians. Additional studies are necessary to further test the efficacy of trunk stabilization exercise on the gait performance of subjects with CP.
References
Cherng RJ, Liao HF, Leung HW, et al. The effec- tiveness of therapeutic horseback riding in chil- dren with spastic cerebral palsy. Adapt Phys Activ Q. 2004;21(2):103-121.
De Kegel A, Baetens T, Peersman W, et al. Ghent developmental balance test: A new tool to eval- uate balance performance in toddlers and pre- school children. Phys Ther. 2012;92(6):841-852.
http://dx.doi.org/10.2522/ptj.20110265
Dewar R, Love S, Johnston LM. Exercise inter- ventions improve postural control in children with cerebral palsy: A systematic review. Dev Med Child Neurol. 2015;57(6):504-520. http://dx.doi.org/
10.1111/dmcn.12660
El-Shamy SM, Abd El Kafy EM. Effect of balance training on postural balance control and risk of fall in children with diplegic cerebral palsy. Disabil Rehabil. 2014;36(14):1176-1183. http://dx.doi.org/
10.3109/09638288.2013.833312
Franjoine MR, Darr N, Held SL, et al. The performance of children developing typically on the pediatric balance scale. Pediatr Phys Ther. 2010;22(4):350-359.
http://dx.doi.org/10.1097/PEP.0b013e3181f9d5eb Geldhof E, Cardon G, De Bourdeaudhuij I, et al.
Static and dynamic standing balance: Test-re- test reliability and reference values in 9 to 10 year old children. Eur J Pediatr. 2006;165(11):
779-786.
Heyrman L, Desloovere K, Molenaers G, et al.
Clinical characteristics of impaired trunk control in children with spastic cerebral palsy. Res Dev Disabil. 2013;34(1):327-334. http://dx.doi.org/10.1016/
j.ridd.2012.08.015
Heyrman L, Molenaers G, Desloovere K, et al. A clin- ical tool to measure trunk control in children with cerebral palsy: The trunk control measurement scale. Res Dev Disabil. 2011;32(6):2624-2635.
http://dx.doi.org/10.1016/j.ridd.2011.06.012
Hibbs AE, Thompson KG, French D, et al.
Optimizing performance by improving core sta- bility and core strength. Sports Med. 2008;38(12):
995-1008. http://dx.doi.org/10.2165/00007256-200838120 -00004
Imms C. Children with cerebral palsy participate: A re- view of the literature. Disabil Rehabil. 2008;30(24):
1867-1884. http://dx.doi.org/10.1080/09638280701673542 Ju YH, You JY, Cherng RJ. Effect of task constraint
on reaching performance in children with spastic diplegic cerebral palsy. Res Dev Disabil. 2010;
31(5):1076-1082. http://dx.doi.org/10.1016/j.ridd.2010.
04.001
Karabay İ, Dogan A, Arslan MD, et al. Effects of functional electrical stimulation on trunk control in children with diplegic cerebral palsy. Disabil Rehabil. 2012;34(11):965-970. http://dx.doi.org/10.3109/
09638288.2011.628741
Karthikbabu S, Nayak A, Vijayakumar K, et al.
Comparison of physio ball and plinth trunk ex- ercises regimens on trunk control and functional balance in patients with acute stroke: A pilot randomized controlled trial. Clin Rehabil. 2011;25(8):
709-719. http://dx.doi.org/10.1177/0269215510397393 Katz-Leurer M, Rotem H, Keren O, et al. The ef-
fects of a ‘home-based’ task-oriented exercise programme on motor and balance performance in children with spastic cerebral palsy and severe traumatic brain injury. Clin Rehabil. 2009;23(8):
714-724. http://dx.doi.org/10.1177/0269215509335293 Kiesel KB, Uhl TL, Underwood FB, et al.
Measurement of lumbar multifidus muscle con- traction with rehabilitative ultrasound imaging.
Man Ther. 2007;12(2):161-166.
Lephart SM, Pincivero DM, Giraido JL, et al. The role of proprioception in the management and rehabilitation of athletic injuries. Am J Sports Med. 1997;25(1):130-137.
Panjabi MM. Clinical spinal instability and low back pain. J Electromyogr Kinesiol. 2003;13(4):371-379.
Prosser LA, Lee SC, VanSant AF, et al. Trunk and hip muscle activation patterns are different dur- ing walking in young children with and without cerebral palsy. Phys Ther. 2010;90(7):986-997.
http://dx.doi.org/10.2522/ptj.20090161
Romero-Franco N, Martínez-López E, Lomas-Vega R, et al. Effects of proprioceptive training pro- gram on core stability and center of gravity control in sprinters. J Strength Cond Res.
2012;26(8):2071-2077. http://dx.doi.org/10.1519/JSC.
0b013e31823b06e6
Saavedra S, Joshi A, Woollacott M, et al. Eye hand coordination in children with cerebral palsy. Exp Brain Res. 2009;192(2):155-165.
Schmit J, Riley M, Cummins-Sebree S, et al.
Children with cerebral palsy effectively modulate postural control to perform a supra-postural task.
Gait Posture. 2015;42(1):49-53. http://dx.doi.org/
10.1016/j.gaitpost.2015.04.001
Shumway-Cook A, Hutchinson S, Kartin D, et al.
Effect of balance training on recovery of stabil- ity in children with cerebral palsy. Dev Med Child Neurol. 2003;45(9):591-602.
Unger M, Jelsma J, Stark C. Effect of a trunk-tar- geted intervention using vibration on posture and gait in children with spastic type cerebral palsy:
A randomized control trial. Dev Neurorehabil.
2013;16(2):79-88. http://dx.doi.org/10.3109/17518423.
2012.715313
Woollacott M, Shumway-Cook A, Hutchinson S, et al. Effect of balance training on muscle activity used in recovery of stability in children with cerebral palsy: A pilot study. Dev Med Child Neurol. 2005;47(7):455-461.
Yaggie JA, Campbell BM. Effects of balance training on selected skills. J Strength Cond Res. 2006;
20(2):422-428.
Zadnikar M, Kastrin A. Effects of hippotherapy and therapeutic horseback riding on postural control or balance in children with cerebral palsy: A meta-analysis. Dev Med Child Neurol. 2011;53(8):
684-691. http://dx.doi.org/10.1111/j.1469-8749.2011.
03951.x
Zapata KA, Wang-Price SS, Sucato DJ, et al.
Ultrasonographic measurements of paraspinal muscle thickness in adolescent idiopathic sco- liosis: A comparison and reliability study. Pediatr Phys Ther. 2015;27(2):119-125. http://dx.doi.org/
10.1097/PEP.0000000000000131
This article was received October 6, 2015, was reviewed October 6, 2015, and was accepted November 7, 2015.