77
A case of protein losing nephropathy in a dog infected with canine Babesia gibsoni
Ha-Jung Kim, Chul Park, Dong-In Jung, Byeong-Teck Kang, Ju-Won Kim, Chae-Young Lim, Hee-Myung Park*
College of Veterinary Medicine, Konkuk University, Seoul 143-701, Korea
(Accepted: January 25, 2006)
Abstract :A 1-year and 6-month-old, intact male, Shih-tzu dog was referred to the Konkuk University Veterinary Teaching Hospital, due to ascite, melena, severe anemia, and polyuria/polydipsia. Complete blood count showed moderate leukocytosis, lymphocytosis, monocytosis, and microcytic hypochromic nonregenerative anemia. On serum biochemistry profiles, hypoalbuminemia and hypoproteinemia were observed, and proteinuria was detected on urinalysis. Pleural effusion and mild ascites were noted in radiological findings, and bilateral nephromegaly was noted on ultrasonography. Babesia gibsoni was detected by PCR. Babesiosis and glomerular disease was treated at a time with prednisolone and buparvaquone. This therapeutic regime was very efficacious and clinical sings were rapidly improved.
Proteinuria and severe anemia were disappeared following therapy.
Key words :babesiosis, glomerulonephritis, protein losing nephropathy, proteinuria Protein-losing nephropathy (PLN) is a complex group
of disorders arising from alterations in glomerular structure and function. There are two major PLN in dogs and cats, which are immune complex glomerulone- phritis (GN) and renal amyloidosis [2]. Veterinary clinicians and pathologists commonly categorize GN with further subdivision as membranouse, proliferative, membranoproliferative, or sclerosing types [6]. The lesions of GN may be regarded as idiopathic (i.e., primary) or secondary to other disorders, such as any chronic antigenic stimulus including infectious, inflammatory and neoplastic diseases [2, 4, 8]. Metabolic disorders (such as diabetes mellitus and hyperadrenocortism) and adminis- tration of various drugs and vaccines may also lead to glomerulonephritis [6]. Some of the more common infectious agents in protein-losing kidney diseases include: Brucellosis, Ehrlichiosis, Leptospirosis, heart worm disease and babesiosis [5].
In babesiosis of dogs, chronic antigenic stimulation may lead to sequelae such as the membranoproliferative glomerulonephritis with IgM deposits that has been
demonstrated in experimental infection with the Califor- nian isolates [14]. Renal damage is common in both complicated and uncomplicated babesiosis [7, 12, 13].
Glomerular proteinuria may lead to clinical signs related to protein loss, such as weight loss, lethargy and eventually, the nephrotic syndrome [2]. Subsequently, plasma colloid osmotic pressure is lowered sufficiently to lead to edema formation including ascite, pleural effusion and pitting edema. Anorexia, weight loss, and vomiting are the most common clinical signs. Urine protein loss are usually detected, using qualitave urine screening tests, a urine dipstick method or via a semi- quantitative test such as a urine protein creatinine ratio [3]. In some PLN cases, treatment of an infection, removal of a neoplastic mass or discontinuation of drug therapy may lead to complete resolution of proteinuria [2].
This case report is to discuss the presentation, diagnosis, treatment and progression of the canine PLN induced by babesiosis.
An 18-months-old, male, Shih-tzu dog was referred to the Konkuk University Veterinary Teaching Hospital
*Corresponding author: Hee-Myung Park
College of veterinary medicine, Konkuk University, Seoul 143-701 Korea [Tel: +82-2-450-4140, Fax: +82-2-450-3037, E-mail: [email protected]]
with a 2-week history of abdominal pain, shivering, fever, melena, and systemic edema. Prior to referred, he was diagnosed as having respiratory disease and was treated accordingly, ascites and polyuria/polydipsia were improved only partially. A complete blood count (CBC), a biochemistry profile, radiographs and an ultra- sonography, and a urinalysis were used initially to detect the causes of the various clinical sings. On physical examination, moderate depression, shivering, and pale mucous membrane were noted. Results of CBC examination revealed moderate leukocytosis, severe lymphocytosis, and moderate monocytosis. Hypochromic non-regenerartive (reticulocytes index: 1.26, Hb: 7.3, PCV:
20.7) anemia was also observed. Results from serum chemistry analysis revealed hypoalbuminemia (1.1 g/dl, reference range: 2.6-3.9 g/dl) and hypoproteinemia (3.3 g/
dl, reference range: 5.0-7.1 g/dl).
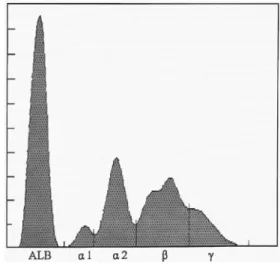
Babesia gibsoni infection was identified on blood films and confirmed by PCR (Fig. 1). In dipstick test, proteinuria (less or more than 100 mg/dl) and isosthenuric (SG: 1.005) was diagnosed. And urine protein creatinine ratio (UPC) was 13.5. Serum electrophoresis (SPE) showed low values of albumin (1.0 g/dl, reference range:
3.6-4.9 g/dl) and gammaglobulin (0.4 g/dl, reference range: 0.6-1.7 g/dl) (Fig. 2). Albumin/globulin ratio was 0.52, which indicated hyperglobulinemia.
Thoracic and abdominal radiographs revealed mild Fig. 1. The PCR-based detection of Babesia gibsoni DNA in Shih-tzu dog. The amplified 1,213bp product, from the positive control (lane 3) or a positive test sample (lane 2), was subjected to electrophoresis in 1.5%-agarose gel and stained with ethidium bromide. A 100-bp ladder (M) and a negative control (saline) free of DNA template (lane 3) were run in parallel.
Fig. 2. An electrophoretogram from a dog with protein- losing nephropathy (PLN). Note the broad-based peak in the alpha2 and gamma region, indicating polyclonal gammopathy. (ALB; albumin, α1; α1-globulin, α2; α2- globulin, β; β-globulin, γ; γ-globulin).
Fig. 3. Right lateral (RL) and ventrodorsal (VD) view of thoracic radiogram. Pleural effusion was shown on ventral thorax in RL view (arrows).
pleural effusion, ascites (Fig. 3 and 4). However, there was no splenomegaly. On ultrasonographic findings, bilateral nephromegaly were detected. Right renal length
was 4.53 and left renal length was 5.38 cm (Fig. 5).
In addition, anechoic fluid is observed in sagittal sonogram (Fig. 4). Aspirated fluid was evaluated and was considered to be transudate. Melena was positive on fecal occult blood test. He was treated with prednisolone (Korea Pharma, Korea, initial dose: 2 mg/kg, PO, BID), and amoxicillin-clavulanic acid (Pfizer Animal Health, U.S.A, 25 mg/kg, PO, BID). For babesiosis, buparvaquone (Essex Animal Health, Germany, 10 mg/kg, IM, once a week) was used. In addition, sucralfate (Choong-wae Pharma, Korea, 0.2 g/kg, PO, BID), and misoprostol (Nelson Korea, Korea, 5µg/kg, PO, BID) were given for prevention of the GI ulceration induced by prednisolone, and ursodeoxycholic acid (Korea United Pharma, Korea, 10 mg/kg, PO, a day), silymarin (Sin- il Pharma, Korea, 50 mg/dog, PO, a day) for the elevated hepatic enzymes. For anemia, erythropoietin (Roche, Germany, 50 IU/kg, SC) and ferrous sulfate (Dae-woong Pharma, Korea, 300 mg/kg, PO, SID) were administrated.
Two weeks after therapy, prednisolone was tapered Fig. 4. Right lateral (RL) (A) and Ventrodorsal (VD) (B)
view on abdominal radiogram. Note the mild subtle changes owing to a small amout of fluid on radiogram.
Sagittal sonogram of the dog revealed that anechoic fluid is seen on sonogram owing to PLN (C).
Fig. 5. Sagittal sonogram of the kidney ([A] right kidney, [B] left kidney). It shows bilateral mild nephromegaly.
range: 37-55 g/dl). There were still elevated hepatic enzymes, but hypoalbuminemia and hypoproteinemia were improved (ALB: 2.0, TP: 4.9). Urinalysis results revealed absence of proteinuria, and normal specific gravity by dipstick. In addition, we performed urine- protein electrophoresis to detect the particular fraction of the urine protein. It showed some albumin and alpha-1 globulin. And UPC was 1.19, which indicated
“questionable” values in proteinuria, not abnormal. But
Babesia gibsoni was still detected by PCR. General condition of the patient was good at this time.
Dogs with UPC≥2.0 are certain to be abnormal, and between 0.5 and 1.0 (or 2.0) are “questionable” value.
In this case, moderate proteinuria was detected. In hypoalbuminenia and hypoproteinemia, it should be differentiated with other diseases (i.e., parasites infection, hypoadrenocorticism, liver disease, systemic inflamma- tory response syndrome, protein losing enteropathy, inflammatory bowel disease). In this case, UPC was 13.5, which indicated severe protein loss with glomerular damage [2]. Serum electrophoresis (SPE) was assessed to rule out the some other diseases with hypoalbuminemia and hyperglobulinemia with polyclonal or monoclonal gammopathy (i.e., canine lymphoma, multiple myeloma, ehrlichiosis).
Canine babesiosis causes multiple organ failure including pulmonary edema, acute respiratory distress syndrome, acute renal failure, hemolytic anemia, cerebral and cerebellar signs [9, 10]. Regenerative anemia and leukocytosis are also related to babesiosis, direct red blood cell damage, intravascular hemolysis, and extrava- scular hemolysis can occur [10, 11]. Severe non- regenerative anemia, leukocytosis, and melena in this case can be related to babesiosis. And lymphocytosis may be result from vaccination recently. Proteinuria can occur secondary to immune-mediated or structural glomerular damage or as a consequence of intraglomerular hypertension.
According to a previous report, 5 to 9 kg of dogs in general has mean renal length of 4.4 cm [2]. However, this patient has more than 4.4 cm in length. But pathogenesis of nephromegaly in this study is unclear at present time. For proteinuric animals that require treatment, the therapeutic goals are to reduce the magnitude of proteinuria and to slow the rate of renal
case.
The management of PLN consists of four basic treatment objectives: (1) identification and elimination of causative antigens, (2) immunomodulation, (3) redu- ction of glomerular inflammation and fibrin deposition, (4) prevention of protein-energy malnutrition. The primary indication for glucocorticosteroids is if the underlying etiology is immune-mediated and responsive.
Angiotensin converting-enzyme inhibitor is used mainly on PLN, for reducing glomerulocapillary blood pressure.
But in this case, primary glomerular disease was suspected rather than secondary to nephron loss due to any cause (e.g., vascular, tubular, interstitial, as well as glomerular). Therefore the therapy was immune suppressive mainly with glucocorticosteroid and endopa- rasiticidal drug. It was very successful to reduce the magnitude of proteinuria.
And we performed the urine protein electrophoresis to detect particular fraction in urine protein after therapy, but it should also have performed before the therapy to get reliable results. After treatment, even if the clinical signs were improved, Babesia gibsoni was still detected by PCR. This study demonstrates that this case should be treated with long term therapy.
In conclusion, this study indicates that canine babe- siosis can cause the membranoproliferative glomerulone- phritis which results in hypoproteinemia and hypoal- buminemia. We report here the successful therapy of PLN in a dog infected with Babesia gibsoni with immune-suppressive drug.
Acknowledgements
The authors are special thanks to Ko-ryo Animal Hospital (Suwon, Korea) for referring this patient.
References
1. Abuelo JG. Proteinuria: diagnostic principles and procedures. Ann Intern Med 1983, 98, 186-191.
2. Bainbridge J, Elliott J. Proteinuria. In: Bainbridge J, Elliott J (eds.). BSAVA Manual of Canine and Feline Nephrology and Urology. 1st ed. pp. 68-84, British Small Animal Veterinary Association, Cheltenham.
1996.
3. Center SA, Wilkinson E, Smith CA, Erb H, Lewis RM. 24-Hour urine protein/creatinine ratio in dogs with protein-losing nephropathies. J Am Vet Med Assoc 1985, 187, 820-824.
4. DiBartola SP, Spaulding GL, Chew DJ, Lewis RM.
Urinary protein excretion and immunopathologic findings in dogs with glomerular disease. J Am Vet Med Assoc 1980, 177, 73-77.
5. Ettinger SJ, Feldman EC. Glomerular disease. In:
Ettinger SJ, Feldman EC (eds.). Textbook of Veterinary Internal Medicine: diseases of the dog and cat. 5th ed.
pp. 1666-1667, Saunders, Philadelphia, 2000.
6. Grauer GF, Thomas CB, Eicker SW. Estimation of quantitative proteinuria in the dog, using the urine protein-to creatinine ratio from a random, voided sample.
Am J Vet Res 1985, 46, 2116-2119.
7. Malherbe WD. Clinico-pathological studies of Babesia canis infection in dogs. V. The influence of the infection on kidney function. J S Afr Vet Med Assoc 1966, 37, 261-264.
8. Muller-Peddinghaus R, Trauwein G. Spontaneous glomrulonephritis in dogs. II. Correlation of glomerulo- nephritis with age, chronic interstitial nephritis and extrarenal lesions. Vet Pathol 1977, 14, 121-127.
9. McGuire W, Hill AV, Allsopp CE, Greenwood BM,
Kwiatkowski D. Variation of the TNF-á promoter region associated with susceptibility to cerebral malaria.
Nature 1994, 371, 508-510.
10.Morita T, Saeki H, Imai S, Ishii T. Erythrocytocyte oxidation in artificial Babesia gibsoni infection. Vet Parasitol 1996, 63, 1-7.
11. Murase T, Ueda T, Yamato O, Tajima M, Maede Y.
Oxidative damage and enhanced erythrophagocytosis in canine erythrocytes infected with Babesia gibsoni. J Vet Med Sci 1996, 58, 259-261.
12.Moore DJ, Williams MC. Disseminated intravascular coagulation: a complication of Babesia canis infection in the dog. J S Afr Vet Med Assoc 1979, 50, 265-275.
13.Reyers F, Leisewitz AL, Lobetti RG, Miller RJ, Jacobson LS, van ZylM. Canine babesiosis in South Africa: more than one disease. Does this serve as a model for falciparum malaria? Ann Trop Med Parasitol 1998, 92, 503-511.
14.Wozniak EJ, Barr BC, Thomford JW, Yamane I, McDonough SP, Moore PF, Naydan D, Robinson TW, Conrad PA. Clinical, anatomic, and immunopa- thologic characterization of Babesia gibsoni infection in the domestic dog (Canis familiaris). J Parasitol 1997, 83, 692-699.
![Fig. 5. Sagittal sonogram of the kidney ([A] right kidney, [B] left kidney). It shows bilateral mild nephromegaly.](https://thumb-ap.123doks.com/thumbv2/123dokinfo/5266981.368806/3.892.466.761.201.651/sagittal-sonogram-kidney-right-kidney-kidney-bilateral-nephromegaly.webp)
