A CASE OF PATHOLOGIC FRACTURE OF THE PROXIMAL FEMUR RESULTING FROM METASTATIC BONE TUMOR OF OVARIAN IMMATURE TERATOMA
Tae Hyun Kim, MD 1 , Seung Yeon Choi, MD 1 , Ji Hee Sung, MD 1 , Chel Hun Choi, MD 1 , Sung Wook Seo, MD 2 , Duk Soo Bae, MD 1
Departments of
1Obstetrics and Gynecology,
2Orthopedics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
Composing of less than 1% of all ovarian cancers, immature teratoma is a malignancy that mainly affects the young. In this report, we present the first case of pathologic fracture of the proximal femur resulting from metastatic bone tumor of ovarian immature teratoma. A 33-year-old Korean female was diagnosed as immature teratoma of stage Ia and grade 3. Eleven months following initial surgery, she had developed right thigh pain and palpable mass, which was confirmed metastasis of immature teratoma. She had her right leg broken during concurrent chemoradiation. She took mass excision, closed reduction with internal fixation and allo-bone graft followed by 6 cycles of chemotherapy and 10 times of radiotherapy. Now she is on regular follow-up and remained disease-free for 14 months.
Keywords: Bone neoplasm; Teratoma; Fractures; Spontaneous; Ovary
Received: 2012.3.10. Revised: 2012.5.17. Accepted: 2012.7.3.
Corresponding author: Duk Soo Bae, MD
Department of Obstetrics and Gynecology, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon- ro, Gangnam-gu, Seoul 135-710, Korea
Tel: +82-2-3410-3519 Fax: +82-2-3410-0630 E-mail: [email protected]
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2012. Korean Society of Obstetrics and Gynecology
Ovarian immature teratoma affects mostly young women and constitutes approximately 1% of all ovarian malignancies [1]. The symptoms are often nonspecific, usually consisting of mass effect inflicting abdominal or pelvic discomfort and this tumor is rapidly progressive without treatment [1,2]. Although it was previously regarded as having a high mortality rate, the concurrent chemo- therapeutic agents, combination of bleomycin, etoposide, and cis- plantin (BEP), gives rise to better survival while minimizing toxicity profile [1,3].
Distant metastasis of immature teratoma of the ovary is uncom- mon [4]. In this report, we present the first case of bone metasta- sis from immature teratoma of the ovary followed by pathologic fracture.
Case Report
A 33-year-old female was diagnosed as ovarian immature tera- toma with stage Ia, grade 3 following left ovarian cystectomy. She underwent staging laparotomy involving hysterectomy, bilateral salpingo-oophorectomy, bilateral pelvic lymph node dissection
and appendectomy. She did not receive adjuvant chemotherapy.
Seven months following staging surgery, the patient revisited with complaints of right thigh pain and 4 × 3 cm sized palpable mass.
The mass was diagnosed as metastatic immature teratoma of the ovary by imaging study and incisional biopsy (Figs. 1, 2). At this point, she was referred to Samsung Medical Center.
She complaints of right thigh pain and initial workup was done at the Department of Orthopedics. It revealed about 20 cm sized http://dx.doi.org/10.5468/KJOG.2012.55.8.590
pISSN 2233-5188 · eISSN 2233-5196
Fig. 1. Initial imaging studies. (A) Plain radiography of the thigh. No pathologic fracture. (B) Magnetic resonance imaging finding.
20×5×4 cm sized solid mass in proximal to mid portion of right femur involving soft-tissue mass and vastus intermedius muscle.
A B
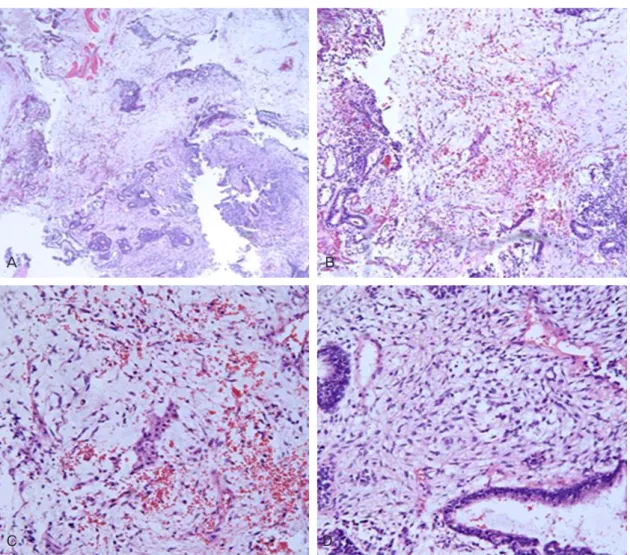
Fig. 2. The pathologic finding of immature teratoma, incisonal biopsy at right thigh palpable mass. (A) Gandular, stromal and muscular differentiations was noted (H&E, ×40). (B) Multifocal malignant transforming area (H&E, ×100). (C, D) Mesenchymal and epithelial cell shows polymorphic and hyperchromatic change with prominent nucleoli. Malignant transformation was detected (H&E, ×200).
A B
C D
mass in the right femur with involvement of adjacent muscle with- out evidence of recurrence at pelvic cavity and another distant metastasis. The serum calcium was 9.5 mg/dL and phosphorus was 3.9 mg/dL. And all tumor markers including were not in- creased. Combination chemotherapy was considered as the first choice of the treatment, therefore she was referred to department of gynecologic oncology. Six cycles of combination chemotherapy with bleomycin (15 mg, day 1 to 3), etoposide (100 mg/m
2, day 1 to 3) and cisplantin (50 mg/m
2, day 1 to 5) every 3 weeks with concurrent radiotherapy (30 Gy/10 fx) were planned. However, 5 days after starting concurrent chemoradiation therapy, she got her right leg broken when sitting up. Plain radiography revealed a pathologic fracture of right femur mid-shaft (Fig. 3A). Treatment was stopped (after 1 cycle of BEP and 5 times radiation therapy, 15 Gy) and she was given a long leg splint.
After 4 weeks, the patient was transferred to the department of Orthopedics for preoperative evaluation. Right femoral vein thrombus was founded during right thigh Doppler doppler ultra- sonography (USG) and inferior vena cava (IVC) filter was inserted before surgery. During surgery, tumor was present along the right femur mid-shaft fracture site with surrounding muscle infiltra- tion. After wide excision of the tumor, approximately 14 cm sized bone defect was made and grafted by femur allo-bone followed
by cementation. Then the patient was given closed reduction with internal fixation by femur intramuscular nail insertion (Fig. 3B).
Pathology revealed metastatic immature teratoma with malignant transformation. Following surgery, thigh computer tomography (CT) revealed no remained mass.
Two weeks later she was referred back to the department of gyne- cologic oncology and completed additional 5 cycles of chemother- apy (total 6 cycles of BEP) followed by 5 times of radiotherapy (50 Gy/5 Fx). Follow-up images involving plain radiography, CT and positron emission tomography show no recurrence and distant metastasis. The patient is on regular follow-up outpatient clinic without evidence of recurrent disease for 14 months.
Discussion
As far as we know, only 11 cases of hematogenous metastasis of immature teratoma of the ovary have been documented in the English language literature (Table 1). This 33-year-old women pre- sented with immature teratoma of the ovary which developed into systemic metastases to right femur within 1 year of initial diagno- sis. Therefore, this case is the first documentation of the bone me- tastasis of immature teratoma of the ovary followed by pathologic fracture.
Fertility sparing surgery and adjuvant combination chemotherapy could be considered for the immature teratoma patients who are young and planning to have a child birth. Most patients with im- mature teratoma of ovary are in their reproductive years and wish to preserve fertility. Because of the excellent response to chemo- therapy, unilateral salpingo-oophorectomy followed by combina- tion chemotherapy has become the standard treatment for early stage of immature teratoma [5]. Nowadays, newly developed combination chemotherapeutic agents such as BEP gives us better survival than before [6].
Prognosis for immature teratoma of the ovary is related to stage and grade of the tumor. The 2-year disease-free survival for grade 1, grade 2, and grade 3 is 83%, 50%, and 33%, respectively [7]. Recurrence can be minimized by postoperative adjuvant chemotherapy. The combination chemotherapy was considered as the standard regimen for patients with stage I, grade 2 and 3 immature teratoma of the ovary [8]. However, Gadducci et al.
[9] advised surgery alone as treatment for the tumor of stage I, grade 2 and 3. In addition, Cushing et al. [10] reported 31 cases of immature teratoma of grade 1-3 were found to have a 5-year survival of 97% after primary conservative therapy (surgical resec- Fig. 3. Plain radiography findings. (A) Fracture of right femur mid-shaft. (B)
Postoperation findings.
A B
tion only), leading the authors to conclude that surgery alone is curative for most children and adolescent with resected ovarian immature teratoma of any grade.
In this case, final diagnosis was immature teratoma, stage Ia, grade 3. Although the exact onset of bone metastasis is not known, the patient’s disease-free interval was only 9 months with- out chemotherapy after primary debulking surgery. This case report suggests, even though it remains controversial, that aggressive postoperative adjuvant chemotherapy for immature teratoma Ia, grade 3 is necessary.
The patients with metastatic bone disease complain of painful palpable mass and swelling. Tumor markers can be used but the correlation with bone metastasis is not clear. Radiologic stud- ies including plain X-ray, radionuclide bone scan and magnetic resonance imaging are helpful to diagnose the bone metastasis.
Radiologic differential diagnosis include various disorder such as osteoporosis, osteomalacia, infections and plasma cell myeloma.
Technetium bisphosphonate bone scans are extremely useful and can be positive up to 18 months before a lesion is detectable on a plain X-ray image [11]. However, a bone biopsy is needed to ob- tain a final diagnosis. Fine-needle aspiration biopsy is considered to have an accuraty rate, or sensitivity, of at least 90% of cases [12]. In the absence of definite tissue diagnosis, a surgical bone biopsy was required for further management. For the patients with low bone mineral density or rapid bone loss, systemic therapy with bisphosphonate administration are available to reduce skeletal- related events.
Surgical management of bone metastasis is contemplated in the case of fractures, or isolated and relatively localized disease, when the patient is in good general condition [13]. This is usually fol- lowed by palliative radiotherapy for control of pain and other local symptoms [14]. Combination chemotherapy may also be beneficial in cases with good performance status and synchronous involve- ment of other sites [15]. In this study, after debulking surgery, Table 1. Reported cases of immature teratoma of the ovary with hematogenous metastasis
Author Year Age-first
diagnosis Stage Grade
Chemotherapy before reoperation
Site of
metastasis Times of resection of metastasis Total
follow-up Dead/
alive
Masopust et al. [18] 1968 13 1 NR A, C Lung Not done 10 mo Dead
Masopust et al. [18] 1968 16 1 NR A, C Lung, thoracic
cavity, supraclav- icular LNs
Not done 6 mo Dead
Esterhay et al. [19] 1973 17 1 NR C, M, V Liver 1 yr 10 mo after the
first operation 3 yr
2 mo Alive
Nogales et al. [1] 1976 17 4 3 Not done Liver Not done 15 day Dead
Nogales et al. [1] 1976 10 4 3 V, M, P, A Liver, lung Not done 6 yr
6 mo Alive
Lentini et al. [20] 1986 19 4 2 Done Liver 4, 18 mo after the
first operation 3 yr
6 mo Alive
Kawai et al. [6] 1991 15 2 2 V, A, C Liver 14 mo after the first
operation 5 yr
10 mo Alive
Caldas et al. [21] 1992 27 3 3 V, A, C Liver 11 yr after
chemotherapy 11 yr
6 mo Alive
Geisler et al. [22] 1994 20 3 2 B, E, P, V, D, C Lung, neck LNs 19 mo after
diagnosis 25 mo Alive
Geisler et al. [22] 1994 22 3 3 B, E, P, V, D, C Liver Shortly after
chemotherapy 31 mo Alive
Li et al. [23] 2002 NR 1 2 B, E, (P) Lung 2 yr after the first
operation 15 yr Alive
Kurata et al. [4] 2010 15 1 2 B, E, (P) Brain, liver, lung
with peribronchial LN
19, 22, 25 mo after
the first operation 10 yr Alive
Present case 2010 33 1 3 Not done Femur 1 yr after the
first operation 14 mo Alive
NR, not reported; A, indicates actinomycin; C, cyclophosphamide; LN, lymph node; M, methotrexate; V, vincristine; P, cisplantin; B, bleomycin; D, dacti-
nomycin; E, etoposide; (P), carboplatin.
chemotherapy then radiotherapy was done. Even in the presence of multiple bone metastasis or an inoperable bone lesion, patients may benefit from radiotherapy, chemotherapy or a combination of both, rather than palliative care alone [15]. In this study, after debulking surgery, chemotherapy then radiotherapy was done.
Finally patients with chronic osseous pain and who demonstrated evidence of bone destruction, presenting a history of gynecology cancer, should be carefully evaluated because, although rare, me- tastasis can arise. This report also indicates that when impending fracture are suggestive, an aggressive approach to prophylactic fixation before a catastrophic fracture developed has distinct ad- vantages [16]. Guidelines for the prediction of pathologic fracture would facilitate the management of patients with metastatic bone defects. Unfortunately, existing clinical guidelines have not been validated and do not accurately predict the risk of fracture for many patients. The load-bearing capacity of a long bone can be predicted using CT with simulated defects [17]. By combining new methods to predict the load-bearing capacity with estimated loads for activities of daily living, it is possible to calculate a factor of risk for pathologic fractures.
At the time of this report, our patient can walk to do the daily living and no evidence of recurrence has been observed for 14 months.
References
1. Nogales FF Jr, Favara BE, Major FJ, Silverberg SG. Immature teratoma of the ovary with a neural component (“solid”
teratoma). A clinicopathologic study of 20 cases. Hum Pathol 1976;7:625-42.
2. Norris HJ, Zirkin HJ, Benson WL. Immature (malignant) tera- toma of the ovary: a clinical and pathologic study of 58 cases.
Cancer 1976;37:2359-72.
3. Williams S, Blessing JA, Liao SY, Ball H, Hanjani P. Adjuvant therapy of ovarian germ cell tumors with cisplatin, etoposide, and bleomycin: a trial of the Gynecologic Oncology Group. J Clin Oncol 1994;12:701-6.
4. Kurata A, Hirano K, Nagane M, Fujioka Y. Immature teratoma of the ovary with distant metastases: favorable prognosis and insights into chemotherapeutic retroconversion. Int J Gynecol Pathol 2010;29:438-44.
5. Long L, Jiang P, Liu FZ, Wang XP, Zhao TJ. Treatment of ovarian malignant germ cell tumors with preservation of fertility. Chin Med J (Engl) 1993;106:303-6.
6. Kawai M, Kano T, Furuhashi Y, Iwata M, Nakashima N, Imai N, et al. Immature teratoma of the ovary. Gynecol Oncol 1991;40:133-7.
7. Gallion H, van Nagell JR Jr, Donaldson ES, Hanson MB, Powell DF. Immature teratoma of the ovary. Am J Obstet Gynecol 1983;146:361-5.
8. Munkarah A, Gershenson DM, Levenback C, Silva EG, Messing MJ, Morris M, et al. Salvage surgery for chemorefractory ovar- ian germ cell tumors. Gynecol Oncol 1994;55:217-23.
9. Gadducci A, Cosio S, Muraca S, Genazzani AR. The manage- ment of malignant nondysgerminomatous ovarian germ cell tumors. Anticancer Res 2003;23:1827-36.
10. Cushing B, Giller R, Ablin A, Cohen L, Cullen J, Hawkins E, et al. Surgical resection alone is effective treatment for ovarian immature teratoma in children and adolescents: a report of the pediatric oncology group and the children’s cancer group.
Am J Obstet Gynecol 1999;181:353-8.
11. Petty RD, Gilbert F, Hutcheon AW, Sarkar TK, McNally O, Parkin D. Bone metastasis from epithelial ovarian carcinoma. Lancet Oncol 2002;3:513.
12. Dubuc-Lissoir J, Berthiaume MJ, Boubez G, Van Nguyen T, Al- laire G. Bone metastasis from a granulosa cell tumor of the ovary. Gynecol Oncol 2001;83:400-4.
13. Pasricha R, Tiwari A, Aggarwal T, Lal P. Carcinoma of uterine cervix with isolated metastasis to fibula and its unusual be- havior: report of a case and review of literature. J Cancer Res Ther 2006;2:79-81.
14. Litton GJ, Ward JH, Abbott TM, Williams HJ Jr. Isolated calcane- al metastasis in a patient with endometrial adenocarcinoma.
Cancer 1991;67:1979-83.
15. Gottwald L, Dukowicz A, Piekarski J, Misiewicz B, Spych M, Misiewicz P, et al. Bone metastases from gynaecological epi- thelial cancers. J Obstet Gynaecol 2012;32:81-6.
16. Ogura K, Miyake R, Shiina S, Shinoda Y, Okuma T, Kobayashi H, et al. Bone radiofrequency ablation combined with prophy- lactic internal fixation for metastatic bone tumor of the femur from hepatocellular carcinoma. Int J Clin Oncol 2011 Sep 15 [Epub]. DOI: http://dx.doi.org/10.1007/s10147-011-0319-y.
17. Hipp JA, Springfield DS, Hayes WC. Predicting pathologic frac- ture risk in the management of metastatic bone defects. Clin Orthop Relat Res 1995:120-35.
18. Masopust J, Kithier K, Rádl J, Koutecký J, Kotál L. Occurrence of fetoprotein in patients with neoplasms and non-neoplastic diseases. Int J Cancer 1968;3:364-73.
19. Esterhay RJ Jr, Shapiro HM, Sutherland JC, McIntire KR, Wi-
ernik PH. Serum alpha fetoprotein concentration and tumor growth dissociation in a patient with ovarian teratocarcinoma.
Cancer 1973;31:835-9.
20. Lentini JF, Love MB, Ritchie WG, Sedlacek TV. Computed tomography in retroconversion of hepatic metastases from immature ovarian teratoma. J Comput Assist Tomogr 1986;10:1060-2.
21. Caldas C, Sitzmann J, Trimble CL, McGuire WP 3rd. Synchro- nous mature teratomas of the ovary and liver: a case present-
ing 11 years following chemotherapy for immature teratoma.
Gynecol Oncol 1992;47:385-90.
22. Geisler JP, Goulet R, Foster RS, Sutton GP. Growing teratoma syndrome after chemotherapy for germ cell tumors of the ovary. Obstet Gynecol 1994;84:719-21.
23. Li H, Hong W, Zhang R, Wu L, Liu L, Zhang W. Retrospective analysis of 67 consecutive cases of pure ovarian immature teratoma. Chin Med J (Engl) 2002;115:1496-500.
대퇴골에 전이된 난소의 미성숙 기형종에서 발생한 병적 골절의 1예
성균관대학교 의과대학 삼성서울병원
1산부인과학교실,
2정형외과학교실
김태현1, 최승연1, 성지희1, 최철훈1, 서성욱2, 배덕수1난소에서 발생하는 미성숙 기형종은 전체 난소암의 1% 미만을 차지하는 희귀종양으로, 평균 발생 연령은 10-20대로 젊은 여성에서 85%가 발생하고 있다. 예전에는 사망률이 매우 높은 질환으로 분류되었으나, 근래에는 항암제의 개발과 bleomycin, etoposide, cisplantin (BEP)의 복합투여요법으로 높은 생존율이 보고되고 있다. 또한 미성숙 기형종의 원격 전이는 매우 드물게 보고되고 있는데, 미성숙 기형 종이 대퇴골에 전이되어 병적 골절이 발생한 1예를 경험하였다. 폐쇄정복/내부교정술과 BEP 화학요법 및 방사선 치료를 시행한 후, 환자 는 혼자 보행이 가능한 상태로 14개월째 재발의 증거 없이 추적관찰 중에 있어 간단한 문헌과 함께 증례를 보고하는 바이다.
중심단어: 미성숙 기형종, 난소, 뼈전이, 병적 골절