120
Introduction
Case
Collision tumors represent the coexistence of two adjacent but histologically distinct tumors in the same organ. There are two types of collision tumor. One is the intermingled type in which two kinds of tumors coexist and there is a histological transition; the other is the contiguous type in which two kinds of tumors exist independently from each other and there is no histological mixture or transition. It is believed that in the intermingled type two different kinds of tumor cells differentiated from progenitor cells to form a mass; in the contiguous type, two different types of tumors close to each other develop simultaneously in the same organ and form a mass. Most collision tumors in the liver are of the intermingled type and they are known to account for
2.0-3.6% of primary liver cancers. A representative example is hepatocholangiocarcinoma. Contiguous-type collision tumors are collision tumors in the true sense, and their percentage among primary liver cancers is low, in the range of 0.1-1%. Representative examples are HCC and neuroendocrine tumors.
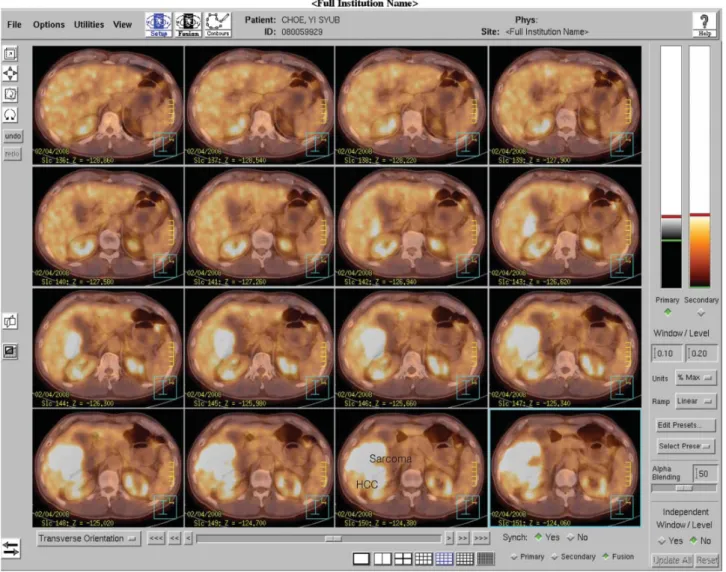
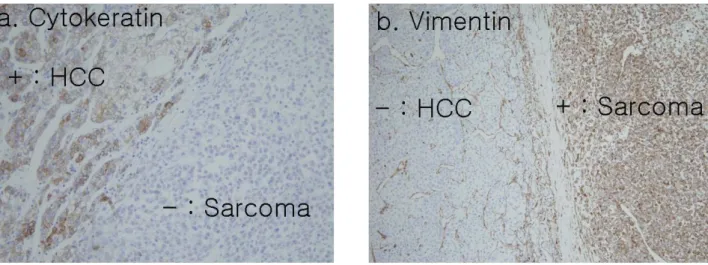
1,2The present authors experienced a case of a collision tumor that consisted of a HCC and an undifferentiated sarcoma. It was identified from the histopathologic findings of a patient who had a hepatectomy for a mass that had developed in the liver.
To the authors’ knowledge, this is the first case of such a collision tumor, and here we report the case with diagnostic tests, histological findings, and the result of treatment.
A 57-year-old patient who had had periodical
Korean Journal of HBP Surgery
Vol. 13, No 2, June
□ 증 례□
간에 발생한 충돌종양 (간세포암과 미분화성 육종)