간문맥 혈전이 동반된 간세포암에서의 간절제술
Hepatic Resection in Patients with Hepatocellular Carcinoma Accompanied by Portal Vein Thrombus
Purpose: Although surgical resection is the most effective treatment for hepatocellular carcinoma (HCC) accompanied by portal vein tumor thrombus (PVTT), the recurrence rate is very high and prognosis is poor. This retrospective analysis aimed to establish a surgical strategy for patients with portal vein thrombus and to identify predictors of tumor thrombus in these patients.
Methods: From 2006 to 2007, 63 hepatocellular carcinoma patients with portal vein thrombus detected by preoperative imaging underwent hepatic resection, and their clinical data were retrospectively analyzed. Possible prognostic factors for survival were analyzed with postoperative survival curves, and significant factors were determined by univariate and multivariate analysis.
Results: 31 patients (49.2%) with portal vein tumor thrombus were detected by pathologic reports in 63 HCC patients with portal vein thrombus. Significant prognostic factors included Serum Albumin ≤3.5 g/dl, Alkaline phosphatase (ALP)≥100 IU/L, Tumor size≥10 cm, non-expanding type, PVTT and Alpha-feto protein (AFP)≥104 IU/L by univariate analysis. Independent prognostic factors included PVTT.
Conclusion: PVTT is not always detected in patients with HCC accompanied by portal vein thrombus. Although patients have a portal vein tumor thrombus, some patients have greater long-term survival. Hepatic resection should be considered for patients with portal vein thrombus.
정성민, 안철수, 이승규, 이영주1
,
박광민1, 황 신, 김기훈, 문덕복,
하태용울산대학교 의과대학 외과학교실 서울아산병원, 간이식 및 간담도외과,
1
간담췌외과
Sung Min Jung, M.D., Chul Soo Ahn, M.D., Sung Gyu Lee, M.D., Young Joo Lee, M.D.
1, Kwang Min Park, M.D.
1, Shin Hwang, M.D., Ki Hun Kim, M.D., Deok Bog Moon, M.D., Tae Yong Ha, M.D.
Departments of Liver Transplantation and Hepatobiliary Surgery,
1
Hepatobiliary Pancreatic Surgery, Asan Medical Center, Ulsan University College of Medicine
책임저자 안 철 수
서울시 송파구 풍납2동 388-1 울산대학교 의과대학 외과학교실 서울아산병원 간이식 및 간담도외과 우편번호 138-736
Tel: 02-3010-3942 Fax: 02-3010-6701 E-mail: [email protected]
Key Words : Hepatocellular carcinoma, Portal vein tumor thrombus, Hepatic resection 중심단어 : 간세포암, 간문맥종양혈전, 간절제술
Received: 2010. 9. 17 Accepted: 2010. 11. 15
서 론
간세포암은 간절제, 간이식의 수술적 치료 뿐 아니라 화학
동맥색전술, 고주파열치료 등의 치료에도 불구하고 여전히 사 망과 관련된 주요 암종이다.1 특히 간세포암이 간문맥에 침윤 하여 간문맥종양혈전을 유발할 경우에는 간내 파종성 전이나 문맥압 상승에 따른 정맥류의 파열, 복수 및 문맥혈류 저하에
따른 간성뇌증, 황달, 간부전을 야기하여 극히 나쁜 예후를 보이며 치료를 하지 않을 경우 중앙 생존률이 2.7∼4개월에 불과하다.2,3 더욱이 간문맥종양혈전을 가진 환자의 경우 수 술 전 간기능이 저하되어 있고 간절제 부위가 넓어지는 경우 가 많아 수술 후 합병증 발생률이 높고 근치적 간절제술을 시 행하였을 경우라도 수술 후 5년 생존률이 10∼30%에 불과하 다.4 하지만 일부 환자에서는 간절제술 단독이나 간절제술 후 보조요법을 병행함으로 장기 생존을 보고한 경우가 있다.5-7 그러므로 간문맥혈전이 있다 하더라도 장기 생존을 기대할 수 있는 환자를 선별하고 수술을 포함한 적절한 치료를 시도할 필요가 있다.
간문맥종양혈전이 있는 환자에서의 적절한 치료는 여전히 많은 이견이 있고 그 자체로 수술의 부적응으로 여겨지기도 했다.4 간세포암 진단시 종종 동반되는 간문맥혈전은 간문맥 종양혈전과 감별이 요구되나 수술 전 영상진단만으로는 이를 감별하기 어려워 치료 방향을 수립하기에 어려움이 많다. 본 후향적 연구는 수술 전 검사 상 간문맥내 혈전으로 진단된 환 자에서 간절제술 후 예후 및 합병증을 분석함으로써 적절한 치료 방향을 제시하고자 하였다.
방 법
1. 대상환자와 추적 관찰
2006년 1월부터 2007년 12월까지 서울아산병원에서 간세 포암으로 간절제술을 시행 받은 775명의 환자 중 수술 전 시 행한 컴퓨터 단층촬영에서 간문맥혈전이 관찰된 63명(8.1%) 의 환자를 대상으로 하였다. 근치적 절제술은 육안적으로 종 양이 완전히 제거되고 현미경적으로 절제연에 종양이 남아 있 지 않은 경우로 정의하였다. 63명의 환자 중 53명에서 근치적 절제술이 시행되었고 10명의 환자에서 현미경적으로 절제연 에 종양이 남아있었다.
수술 대상 환자들은 대부분 Child-Pugh A (95.2%)였으며 수술 전 간기능 확인을 위해 Indocyanine green 15분 정체율 검사를 시행하였고 간기능검사 소견 및 암종의 크기와 위치를 고려하여 절제 범위를 결정하였다.
모든 환자에서 수술 전 후 alpha-feto protein (AFP) 검사를 시행하였고 수술 전 종양의 크기가 크고 AFP이 상승되어 있 는 경우와 조직검사상 절제연에 종양이 남아 있거나 미세혈관 침윤이 있는 경우에 한달 이내에 간동맥 조영술 및 화학색전
술을 시행하였다. 63명의 수술 후 평균 추적 관찰기간은 24개 월(범위, 2∼47개월)이었다. 수술 후 6개월을 기준으로 초기 재발과 후기 재발로 구별하였다. AFP이 상승하거나 컴퓨터 단층 촬영에서 새로운 병변이 확인된 경우 재발을 의심하였으 며 간동맥 조영술을 통하여 확인하였다.
2. 종양혈전의 예측인자 및 생존율과 관련된 예후 인 자 분석
종양혈전의 예측인자 및 생존률과 관련된 예후 인자를 알기 위해 환자 관련 변수인 나이, 성별, 혈청알부민 수치, Alanin aminotransferase (ALT), Aspartate aminotransferase (AST), 혈소판 수치, 빌리루빈 수치, Alkaline phospatase (ALP), Prothrombin time (PT), Indocyanine green 15분 정체율를 분석하였다. 종양인자로 문맥혈전의 위치, 종양의 크기, 간세 포암의 재발여부를 분석하였다.
전체 생존율과 관련된 예후 인자는 임상 및 병리학적 변수 를 사용하였다. 수술과 관련된 변수는 간절제 범위, 근치적 절제 여부로 하였다. Couinaud 분류에 따라 3개 이상의 분절 을 절제하는 경우를 대량 간절제로, 2개 이하 분절을 절제하 는 경우를 소량 간절제로 정의하였다. 종양관련 변수는 육안 적 형태분류, 위성 결절 유무, 육안적 혈관 침윤여부, 현미경 적 혈관 침윤 여부, 종양의 분화도(Edmondson-Steiner 등급), 혈청 AFP 수치, 문맥내혈전의 위치 등을 포함하였다. 종양의 육안적 분류는 팽창성결절형, 다결절융합형, 결절주위파급형, 침습형 등으로 분류하였다. 이전 연구에 의하면 팽창성결절형 종양이 다른 형태의 종양과 비교하여 절제 후 예후가 좋은 것 으로 보고하였고8-10 이에 따라 팽창성결절형 종양과 비팽창성 결절형 종양의 이분형 변수로 분석하였다.
3. 통계 분석
모든 데이터는 환자의 백분율이나 평균 및 표준편차로 나타 내었다. 생존 곡선은 Kaplan-Meier method를 사용하였고 생 존율 차이를 비교하기 위해 Log-rank test를 이용하였다. 생존 과 연관이 있는 인자들을 단변량 분석을 시행하여 얻은 후 Cox-proportional hazards model에 포함하여 다변량 분석을 시행하였다. 범주형 변수들은 Chi-squre test 를 이용하여 비 교하였다. 통계 분석은 SPSS 12 windows (SPSS, inc, Chica- go, IL)를 이용하였고
p
-value가 0.05 미만의 경우를 통계적으 로 유의한 것으로 정의하였다.Table 1. Clinicopathological fetures of 63 HCC patients with Portal vein thrombus
Age (years) Gender Male/Female
Etiology of liver disease Hepatitis B virus Hepatitis C virus Alcoholic abuse Unknown
Child-Pugh classification A/B
Tumor size (cm) Serum AFP (IU/ml) Mean
Medial (range) Cirrhosis
Preoperative treatment Location of PV thrombus in PreOP CT
Main Trunk (Vp4) 1st order branch (Vp3) 2nd order branch (Vp2) 3rd order branch (Vp1) Gross classification of tumor Expanding nodular type Multinodular confluent type
Nodular with perinodular extension type
Infiltrative type Cirrhotomimetic type Total necrosis
Protal vein tumor thrombus Microvascular invasion Satellite nodule Curative resection
50.6 (range, 24∼73)
47 (74.6%)/16 (25.4%)
53 (84.1%) 2 (3.2%) 2 (3.2%) 6 (9.5%)
60 (95.2%)/3 (4.8%) 8.7 (range 1.6∼21.0)
55,800
1,215 (range, 4.5∼1,700,000) 33 (52.4%)
8 (12.7%)
3 (4.8%) 29 (46.0%) 20 (31.7%) 11 (17.5%)
13 (20.6%) 33 (52.4%)
8 (12.7%)
4 (6.3%) 2 (3.2%) 3 (4.8%) 31 (49.2%) 46 (73.0%) 16 (25.4%) 53 (84.2%)
Table 2. Operative procedure and postoperative complication Major resection
Right hepatectomy
Right extended hepatectomy Letft extended hepatectomy Central bisectionectomy Minor resection
Left lateral sectionectomy Right anterior sectionectomy Right posterior sectionectomy Bisegmentectomy
Monosegmentectomy Postoperative morbidity Postoperative bleeding Intra-abdominal abscess Pleural effusion Postoperative ileus Bile leakage/biloma Ascites
Pneumonia Wound infection Postoperative mortality
33 (52.4%) 1 (1.6%) 2 (3.2%) 2 (3.2%)
7 (11.1%) 4 (9.5%) 6 (6.3%) 1 (1.6%) 7 (11.1%) 25 (39.7%)
0 1 3 9 2 14 2 3 0 (0.0%)
결 과
수술 전 간문맥혈전이 진단된 63명 환자의 임상 및 병리학 적 특징은 Table 1에 요약하였다. 평균 연령은 50.6세였으며 남자가 47명(74.6%)이었다. 간 질환의 원인은 53예(84.1%)에 서 B형 간염으로 가장 흔했으며, 혈청 AFP의 중앙 수치는 1,215 IU/ml이었고 간경변은 33예(52.4%)에서 현미경적으로 진단되었다. 술전 간동맥화학색전술이나 고주파열치료를 시
행한 경우가 8예(12.7%) 있었다. 종양의 육안적 분류는 다결 절융합형이 32예(50.8%)로 가장 많았다. 간문맥혈전이 조직 검사 상 종양혈전으로 확인된 경우가 31예(49.2%)였다. 수술 전 CT 소견에서 간문맥혈전은 총간문맥에 위치하는 경우가 3예였고 제1분지에 위치하는 경우가 29예(46.0%)로 가장 많 았다. 현미경적 혈관 침윤은 46예(73%)에서 있었고 위성결절 이 있는 경우는 16예(25.4%)였다.
근치적 절제는 53예(84.2%)에서 시행되었다. 대량 간절제 는 38예(60.3%)에서 시행되었고 소량 간절제는 25예에서 시 행되었으며 간우엽 절제술이 33예(52.4%)로 가장 많이 시행 되었다. 수술과 관련된 사망은 없었으며 합병증은 이뇨제 복 용 등 치료가 필요한 복수 발생이 14예로 가장 많았고 배액관 삽입이 필요한 복강내 농양과 흉수의 발생이 각각 1명, 3명 있었다(Table 2).
종양혈전의 예측 인자 중 술전 측정한 Prothrombin (PT) 수치만이 유의였으며(
p
=0.018, OR:3.5, 95% CI: 1.238∼9.891) 간문맥혈전의 위치(
p
=0.528)나 종양의 크기(p
=0.229) 등은 통계적으로 유의하지 않았다(Table 3).관찰 기간 중 32명(50.8%)의 환자가 사망하였으며 재발의 소견 없이 간성혼수로 사망한 1예(1.6%) 외에 재발의 소견 없
Table 3. Comparison of clinical characteristics of HCC with Portal vein thrombus
PVT without tumor thrombus (n=32) PVTT (n=31) p-value
Age (yrs) Gender (% male) Positive HBs-Ag (%) Serum albumin (g/dl) ALT (IU/L)
AST (IU/L) Platelet (103/ul) AFP (ng/ml) T-Bil (mg/dl) ALP (IU/L) PT (≤90%) ICGR15
Location of PVT (Vp3-4) Tumor size (cm) Preoperative Treatment
49.5±11.6 81.3
75 3.66±0.44
64±37 47±34 182±70 25,208±52,239
1.02±0.56 125±87
37.50%
15.2±6 46.90%
9.3±4.5 9.40%
51.7±10.3 67.7 93.50 3.55±0.42
61±37 35±16 164±87 88,432±316,928
1.07±0.37 113±68
67.7 15.1±9.7
54.80%
8.0±4.3 16.10%
0.515 0.223 0.06 0.343 0.724 0.09 0.362 0.27 0.704 0.566 0.018 0.953 0.528 0.229 0.426
Fig. 1. Disease free and overall survivals of 63 HCC patients after hepatectomy.
이 사망한 예는 없었다. 수술 후 1년, 3년 전체 생존률은 각각 73.0%, 48.8%였다. 전체 생존율과 무병 생존율 곡선을 보았 을 때 수술 후 1년 후부터 재발 및 사망이 현저히 감소하였다 (Fig. 1). 수술 후 27개월의 중앙 추적 기간 동안 46예(73%)에 서 재발을 경험하였다. 간외 재발은 28예(44.4%)에서, 간내 소결절형 재발은 8예(12.7%)에서, 간내 다결절형 재발은 10예 (15.9%)에서 각각 발생하였다. 1년내 재발한 경우가 39예 (61.9%)이었고, 특히 6개월 이내에 재발한 경우가 37예 (58.7%)였다.
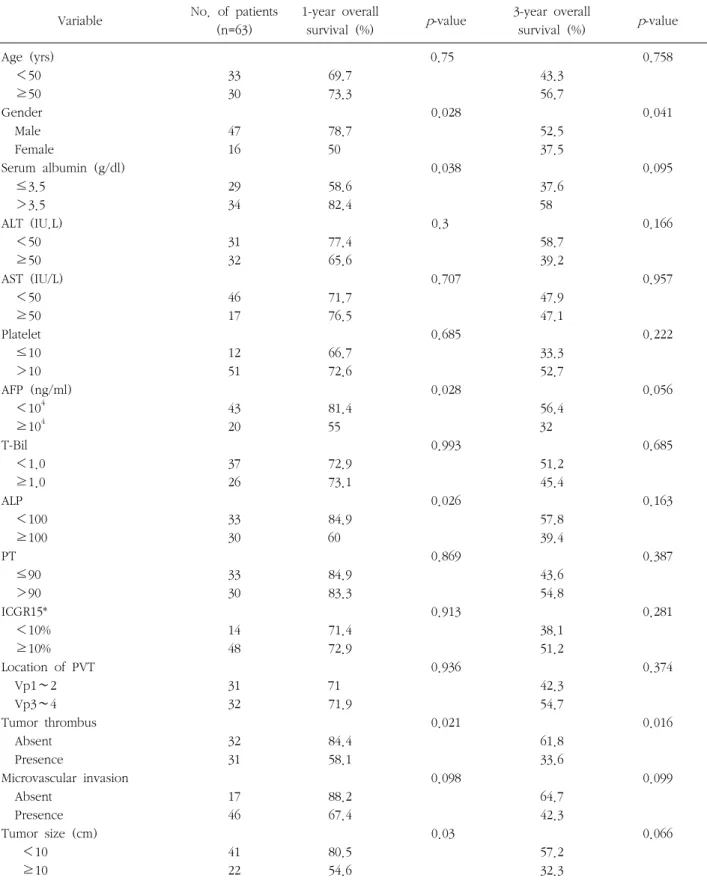
전체 생존률에 영향을 미치는 예후인자 분석에서 간기능 지 표 중 ALP ≥100 IU/L (
p
=0.025)와 ALB ≤3.5 g/dl (p
=0.038)이 단변량 분석에서 불량한 예후 인자로 나왔다. 종양 지표 중에서 종양크기 ≥10 cm (
p
=0.03)와 간문맥종양혈전이 존재하는 경우(p
=0.021), AFP ≥104 ng/ml (p
=0.028)에 단변 량 분석에서 의미가 있었다. 술 후 6개월 내에 재발한 경우(p
≤0.001) 매우 안 좋은 예후를 보였고 1년, 3년 생존률이 각각 51.4%, 26.8%이었다(Table 4). 단변량 분석에서 의미 있었던 변수들로 다변량 분석을 시행하였을 때 의미 있는 인자로는 종양인자인 간문맥종양혈전 존재 여부(
p
=0.016, Hazard ratio=2.585, 95% Confidence interval, 1.196-5.586)만이 술 후 생존 률과 관련 있는 독립적인 예후 인자였다(Table 5). 간문맥종 양혈전이 없는 환자의 1년, 3년 전체 생존률은 각각 84.4%,
Table 4. Univariate analysis of prognostic factors for overall survival
Variable No. of patients (n=63)
1-year overall
survival (%) p-value 3-year overall
survival (%) p-value Age (yrs)
<50 ≥50 Gender Male Female
Serum albumin (g/dl) ≤3.5
>3.5 ALT (IU.L) <50 ≥50 AST (IU/L) <50 ≥50 Platelet ≤10 >10 AFP (ng/ml) <104 ≥104 T-Bil <1.0 ≥1.0 ALP <100 ≥100 PT ≤90 >90 ICGR15*
<10%
≥10%
Location of PVT Vp1∼2 Vp3∼4 Tumor thrombus Absent Presence
Microvascular invasion Absent
Presence Tumor size (cm) <10 ≥10
33 30
47 16
29 34
31 32
46 17
12 51
43 20
37 26
33 30
33 30
14 48
31 32
32 31
17 46
41 22
69.7 73.3
78.7 50
58.6 82.4
77.4 65.6
71.7 76.5
66.7 72.6
81.4 55
72.9 73.1
84.9 60
84.9 83.3
71.4 72.9
71 71.9
84.4 58.1
88.2 67.4
80.5 54.6
0.75
0.028
0.038
0.3
0.707
0.685
0.028
0.993
0.026
0.869
0.913
0.936
0.021
0.098
0.03
43.3 56.7
52.5 37.5
37.6 58
58.7 39.2
47.9 47.1
33.3 52.7
56.4 32
51.2 45.4
57.8 39.4
43.6 54.8
38.1 51.2
42.3 54.7
61.8 33.6
64.7 42.3
57.2 32.3
0.758
0.041
0.095
0.166
0.957
0.222
0.056
0.685
0.163
0.387
0.281
0.374
0.016
0.099
0.066
Table 4. Continued
Variable No. of patients (n=63)
1-year overall
survival (%) p-value 3-year overall
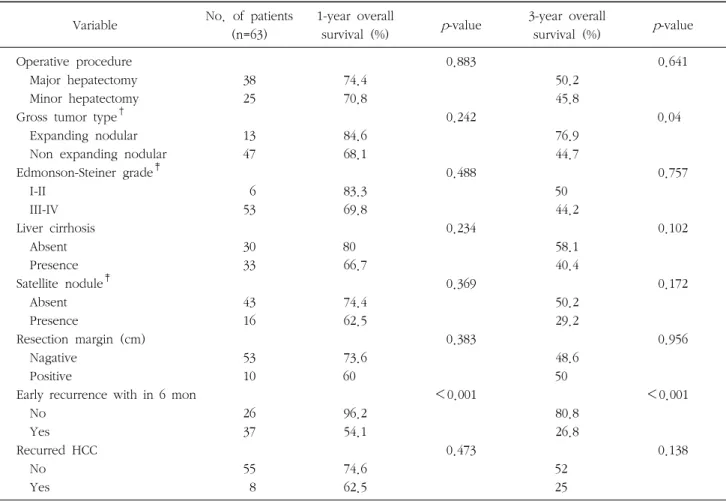
survival (%) p-value Operative procedure
Major hepatectomy Minor hepatectomy Gross tumor type† Expanding nodular Non expanding nodular Edmonson-Steiner grade‡ I-II
III-IV Liver cirrhosis Absent Presence Satellite nodule‡ Absent Presence
Resection margin (cm) Nagative
Positive
Early recurrence with in 6 mon No
Yes Recurred HCC No
Yes
38 25
13 47
6 53
30 33
43 16
53 10
26 37
55 8
74.4 70.8
84.6 68.1
83.3 69.8
80 66.7
74.4 62.5
73.6 60
96.2 54.1
74.6 62.5
0.883
0.242
0.488
0.234
0.369
0.383
<0.001
0.473
50.2 45.8
76.9 44.7
50 44.2
58.1 40.4
50.2 29.2
48.6 50
80.8 26.8
52 25
0.641
0.04
0.757
0.102
0.172
0.956
<0.001
0.138
*One patieunt doesn’t have exam; †Total necrosis (n=3); ‡non description on pathologic report (n=1), Total necrosis (n=3)
Table 5. Multivariate analysis of the prognostic factors of overall survival by Cox Proportional Hazard Model
Prognostic factors Hazard
ratio p-value 95% CI Gender male/female
ALB ≤3.5/>3.5 g/dl ALP <100/≥100 IU/L TT absent/presence Size <10/≥10 cm AFP <104/≥104 ng/ml
1.36 1.881 1.38 2.585 1.315 1.802
0.461 0.14 0.511 0.016 0.517 0.185
0.6∼3.082 0.813∼4.349 0.528∼3.603 1.196∼5.586 0.574∼3.013 0.755∼4.3
61.8%였고, 간문맥종양혈전이 있는 경우는 각각 58.6%, 33.6%였다(Fig. 2).
고 찰
현미경적 혈관 침윤은 간세포암 환자에서 암종의 크기와 관 계없이 수술 후 재발과 생존율을 예측할 수 있는 독립적인 인
자이다.11-14 특히 간문맥종양혈전은 간내 다발성 종양의 전이
에 가장 중요한 인자로 보고되어 있으며 간문맥압의 상승을 유도해 이에 따른 합병증 등으로 환자의 자연 경과는 매우 불 량하다고 보고되고 있다.2,3 따라서 간세포암 환자에서 술 전 간문맥종양혈전을 발견하는 것은 치료 전략을 세우는데 매우 중요한 지표가 된다. 간문맥혈전 유무는 수술 전 컴퓨터 단층 촬영이나 도플러 초음파를 시행하여 확인할 수 있지만 간문맥 혈전은 종양의 혈관 침윤 뿐 아니라 종괴에 의한 문맥 압박으 로 인해 발생할 수 있으며 영상 진단만으로 종양혈전 여부들 판단하는 것은 한계가 있다.11,12
Fig. 2. Comparison of overall survival between Portal vein thrombus and tumor thrombus after hepatectomy.
간문맥종양혈전이 있는 경우 이전 연구에 의하면 간절제절 후 일부 환자에서 장기 생존을 보이는 경우는 있으나 대부분 안 좋은 예후를 보였다.4 수술에 따른 위험성이 높다 하더라도 수술에 따른 예후가 양호한 경우 수술은 쉽게 받아들여지지만 예후가 나쁜 반면 수술에 따른 위험성이 높은 경우 수술적 치 료를 선택하기란 쉽지 않다. 더욱이 수술에 따른 합병증의 발 생은 수술 후 보조항암치료의 기회를 줄일 수 있다.15-17 이런 이유로 수술 전 간문맥혈전이 발견된 환자에서 수술의 결정은 환자나 의료진 모두에게 일반적으로 어려운 선택이 된다. 그 러나 본 연구에서와 같이 정확한 수술과 술전, 술후의 세심한 치료를 병행한다면 간문맥혈전 환자의 수술후 합병증은 다른 간암환자의 수술과 특별한 차이를 보이지 않으며(Table 2), 일 반적인 원칙에 의한 적극적인 수술을 고려해 볼 수 있으며 간 문맥혈전의 존재자체를 수술의 부적응증으로 생각해서는 안 될 것이다.
본 연구에서 수술 전 간문맥혈전이 확인된 환자는 63명 (8.1%)였다. 이들 환자의 무병생존율 및 전체 생존율 곡선 (Fig. 1)에서 수술 후 1년이 지나면 재발 및 사망이 현저히 완화되는 것을 볼 수 있다. 46명의 재발 환자 중 37명이 수술 후 6개월 이내에 발생하였다. 이는 대상 환자들에서 재발이 잔존 간실질에서 다중심성으로 새롭게 발생하기 보다는 혈관 침윤에 따른 전이에 의해 발생했을 가능성이 매우 높다고 생 각한다. 간문맥혈전이 있는 환자의 절제 후 3년 전체생존율은 48.8%였고 3년 무병 생존률은 28.2%였다. 이는 수술 전 문맥 혈전이 있더라도 1/3의 환자에서는 수술적 절제로 장기생존
을 기대할 수 있다는 것을 시사한다.
간문맥혈전을 가진 환자(63명) 중 조직검사 상 종양혈전으 로 확인된 경우는 31명(49.2%)였다. 단변량 분석에서 간문맥 혈전을 예측할 수 인자로 Prothrombin time (PT)이 90% 이하 인 경우(
p
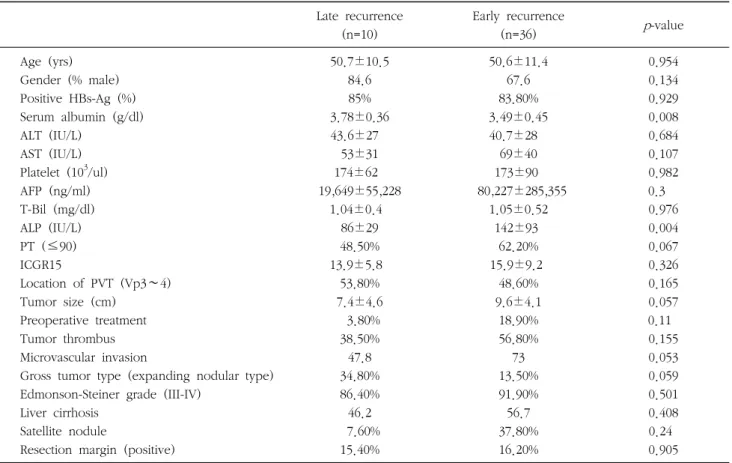
=0.018, OR:3.5, 95% CI: 1.238∼9.891)가 있었으나 종양혈전과 상관관계를 확인할 수가 없었으며 다변량 분석에 서 의미있는 결과를 얻지 못했다(Table 3). 혈전 위치와 종양 크기는 의미있는 예측인자는 아니었고 이는 수술 전 간문맥혈 전이 있어도 영상진단이나 임상적 특징만으로 종양혈전을 예 측하기는 어렵다고 생각한다. 6개월 내 재발하지 않은 26명 중 10명(38.5%)에서 간문맥종양혈전을 가지고 있었고 이들의 1년, 3년 전체 생존률과 무병생존률이 각각 92.3%, 80.8%와 88.5%, 63.7%였다. 이는 간문맥종양혈전의 경우에도 조기 전 이가 없는 경우에는 장기 생존이 가능할 수 있다는 점을 시사 하지만 조기전이를 구별할 수 있는 조건에 대하여는 확실히 알 수는 없다. 6개월 내 조기재발과 관련된 변수로는 혈청 알 부민 수치(p
=0.008)과 ALP (p
=0.004)가 있었으나 의미를 논 하기는 한계가 있다(Table 6).간기능 검사 중 전체생존률의 예후 인자로 혈청알부민 (
p
=0.038), ALP (p
=0.026) 등이 있으나 이들이 간문맥종양혈 전증과의 직접적인 관계를 설명하는 것은 무리가 있다고 생각 한다. 다만 ALP의 상승은 최근 연구에서 이들은 간기능의 지 표일 뿐 아니라 종양에 의한 압박이나 담도계 침윤에 따른 효 과로써 악성도의 지표로 쓰일 수 있다 보고되었다.16-18 총빌리 루빈이 높은 환자에서는 광범위 수술20이나 보조 항암치료6,7,16 는 술 후 간부전의 위험으로 피해져 왔다. 따라서 총빌리루빈 수치는 본 연구에서는 의미 있는 결과가 나오지는 않았지만 간문맥혈전이 있고 총빌리루빈 수치, ALP가 높은 환자의 수술 결정은 신중해야 한다. 종양 주변 간경변은 재발 및 생존율에 영향을 주지 못했다.종양과 관련된 예후 인자로는 간문맥종양혈전(
p
=0.021)과 크기가 10 cm 이상인 경우(p
=0.03), AFP 수치가 10,000 ng/ml이상인 경우(p
=0.028)에 단변량 분석에서 의미있었다.치료와 관련된 예후 인자 중 절제면 간세포암 잔존 여부도 (
p
=0.383) 의미 있는 인자는 아니었다. 기존 연구에서 전제면 잔존은 암종의 노출이 없었다면 술 후 생존에 영향을 미치지 않는다고 한다.21,22 이는 간절제 후 재발 양상이 절단면에서 발생하기 보다는 문맥을 통한 다발성 간내 전이로 재발하는 양상 때문이며 본 연구 환자들의 재발 양식 역시 문맥을 통한Table 6. Comparison of clinicopathologic features of HCC with early recurrence (6 mon) Late recurrence
(n=10)
Early recurrence
(n=36) p-value
Age (yrs) Gender (% male) Positive HBs-Ag (%) Serum albumin (g/dl) ALT (IU/L)
AST (IU/L) Platelet (103/ul) AFP (ng/ml) T-Bil (mg/dl) ALP (IU/L) PT (≤90) ICGR15
Location of PVT (Vp3∼4) Tumor size (cm)
Preoperative treatment Tumor thrombus Microvascular invasion
Gross tumor type (expanding nodular type) Edmonson-Steiner grade (III-IV)
Liver cirrhosis Satellite nodule
Resection margin (positive)
50.7±10.5 84.6 85%
3.78±0.36 43.6±27
53±31 174±62 19,649±55,228
1.04±0.4 86±29 48.50%
13.9±5.8 53.80%
7.4±4.6 3.80%
38.50%
47.8 34.80%
86.40%
46.2 7.60%
15.40%
50.6±11.4 67.6 83.80%
3.49±0.45 40.7±28
69±40 173±90 80,227±285,355
1.05±0.52 142±93
62.20%
15.9±9.2 48.60%
9.6±4.1 18.90%
56.80%
73 13.50%
91.90%
56.7 37.80%
16.20%
0.954 0.134 0.929 0.008 0.684 0.107 0.982 0.3 0.976 0.004 0.067 0.326 0.165 0.057 0.11 0.155 0.053 0.059 0.501 0.408 0.24 0.905
다발성 간내 전이에 의한 것으로 판단된다.
생존과 관련된 예후 인자들 중 다변량 분석에서 의미있는 인자는 종양혈전증이 확인된 경우(
p
=0.016, Harzard raito:2.585, 95% CI:1.196∼5.586)에서 이다(Table 5).
총간문맥(Vp4)에 종양혈전이 있는 경우는 제1분지 이하에 종양혈전이 있는 경우 보다 현저히 예후가 좋지 않은 것으로 보고되었다.23 본 연구에서도 3명의 Vp4환자 모두 한달 내외 로 시행한 간동맥 조영술에 다발성 간전이가 관찰되었고 7개 월 내 사망하였다. VP4환자는 식도 위 정맥류의 파열이나 급 성 간부전으로 급작스런 사망에 이를 수 있어 수술을 통한 제거가 요구되기도 한다.23 하지만 수술에 따른 합병증의 발생 및 수술 자체가 환자로부터 다른 보조 치료의 기회마저 앗아 갈 수 있다.5,24,25 본 연구에서 Vp4환자는 3명에 불과 하였으므 로 좀 더 많은 환자에서 술 후 합병증 발생 및 생존률에 대한 연구가 요구된다.
결 론
간문맥혈전이 있는 환자 중 수술 전 종양혈전을 영상검사를 통해 진단하는 것에는 한계가 있고 연구에서도 뚜렷한 예측 인자를 확인하지는 못하였다. 간문맥혈전이 있는 환자에서 수 술 후 조기재발을 잘하고 특히 종양혈전으로 진단된 경우에 더욱 나쁜 예후를 보였다. 그러나 간문맥혈전을 가진 환자에 서 49.8%만이 수술 후 간문맥종양혈전으로 확인되었으며 간 문맥 종양혈전이 있는 경우라도 좋은 예후를 보이는 경우가 있었다. 또한 비록 간문맥혈전증의 경우라도 세심한 간절제술 을 시행한다면 합병증은 다른 환자와 특별한 차이를 보이지 않으므로 간문맥혈전이 있는 경우라도 가능한 간절제술 시행 을 고려하는 것이 환자에게 도움이 될 수 있다. 그러나 간문맥 종양혈전의 수술적 치료에 대한 완전한 결론을 위해서는 향후 더 많은 연구와 노력이 필요하다고 생각한다.
참 고 문 헌
1. Llovet JM. Updated treatment approach to hepatocellular carcinoma. J Gastroenterol 2005;40:225-235.
2. Llovet JM, Bustamante J, Castells A, et al. Natural history of untreated nonsurgical hepatocellular carcinoma: rationale for the design and evaluation of therapeutic trials. Hepatology 1999;29:62-67.
3. Villa E, Moles A, Ferretti I, et al. Natural history of inoperable hepatocellular carcinoma: estrogen receptors' status in the tumor is the strongest prognostic factor for survival.
Hepatology 2000;32:233-238.
4. Minagawa M, Makuuchi M. Treatment of hepatocellular carcinoma accompanied by portal vein tumor thrombus.
World J Gastroenterol 2006;12:7561-7567.
5. Lau WY, Lai EC. Hepatocellular carcinoma: current management and recent advances. Hepatobiliary Pancreat Dis Int 2008;7:237-257.
6. Minagawa M, Makuuchi M, Takayama T, Ohtomo K.
Selection criteria for hepatectomy in patients with hepatocellular carcinoma and portal vein tumor thrombus.
Ann Surg 2001;233:379-384.
7. Fukuda S, Okuda K, Imamura M, Imamura I, Eriguchi N, Aoyagi S. Surgical resection combined with chemotherapy for advanced hepatocellular carcinoma with tumor thrombus:
report of 19 cases. Surgery 2002;131:300-310.
8. Inayoshi J, Ichida T, Sugitani S, et al. Gross appearance of hepatocellular carcinoma reflects E-cadherin expression and risk of early recurrence after surgical treatment. J Gastroenterol Hepatol 2003;18:673-677.
9. Nakashima Y, Nakashima O, Tanaka M, Okuda K, Nakashima M, Kojiro M. Portal vein invasion and intrahepatic micrometastasis in small hepatocellular carcinoma by gross type. Hepatol Res 2003;26:142-147.
10. Kim CH, Choi GH, Han DH, et al. The outcome after Curative Resection for a Huge (>10 cm) Hepatocellular Carcinoma. Korean Journal of HBP Surgery 2008;12:238-244.
11. Dodd GD 3rd, Memel DS, Baron RL, Eichner L, Santiguida LA. Portal vein thrombosis in patients with cirrhosis: does sonographic detection of intrathrombus flow allow differen- tiation of benign and malignant thrombus? AJR Am J Roent- genol 1995;165:573-577.
12. Ricci P, Cantisani V, Biancari F, et al. Contrast-enhanced color Doppler US in malignant portal vein thrombosis. Acta Radiol 2000;41:470-473.
13. Pandey D, Lee KH, Wai CT, Wagholikar G, Tan KC. Long term outcome and prognostic factors for large hepatocellular
carcinoma (10 cm or more) after surgical resection. Ann Surg Oncol 2007;14:2817-2823.
14. Shah SA, Wei AC, Cleary SP, et al. Prognosis and results after resection of very large (>or=10 cm) hepatocellular carcino- ma. J Gastrointest Surg 2007;11:589-595.
15. Zhou YM, Yang JM, Li B, et al. Risk factors for early recurrence of small hepatocellular carcinoma after curative resection. Hepatobiliary Pancreat Dis Int 2010;9:33-37.
16. Liang LJ, Hu WJ, Yin XY, et al. Adjuvant intraportal venous chemotherapy for patients with hepatocellular carcinoma and portal vein tumor thrombi following hepatectomy plus portal thrombectomy. World J Surg 2008;32:627-631.
17. Zhou J, Tang ZY, Wu ZQ, et al. Factors influencing survival in hepatocellular carcinoma patients with macroscopic portal vein tumor thrombosis after surgery, with special reference to time dependency: a single-center experience of 381 cases.
Hepatogastroenterology 2006;53:275-280.
18. Ikai I, Hatano E, Hasegawa S, et al. Prognostic index for patients with hepatocellular carcinoma combined with tumor thrombosis in the major portal vein. J Am Coll Surg 2006;
202:431-438.
19. Ikenaga N, Chijiiwa K, Otani K, Ohuchida J, Uchiyama S, Kondo K. Clinicopathologic characteristics of hepatocellular carcinoma with bile duct invasion. J Gastrointest Surg 2009;13:492-497.
20. Kumada K, Ozawa K, Okamoto R, et al. Hepatic resection for advanced hepatocellular carcinoma with removal of portal vein tumor thrombi. Surgery 1990;108:821-827.
21. Ochiai T, Takayama T, Inoue K, et al. Hepatic resection with and without surgical margins for hepatocellular carcinoma in patients with impaired liver function. Hepatogastroenterology 1999;46:1885-1889.
22. Hashimoto T, Minagawa M, Aoki T, et al. Caval invasion by liver tumor is limited. J Am Coll Surg 2008;207:383-392.
23. Kondo K, Chijiiwa K, Kai M, et al. Surgical strategy for hepatocellular carcinoma patients with portal vein tumor thrombus based on prognostic factors. J Gastrointest Surg 2009;13:1078-1083.
24. Ishikawa T, Imai M, Kamimura H, et al. Improved survival for hepatocellular carcinoma with portal vein tumor throm- bosis treated by intra-arterial chemotherapy combining etopo- side, carboplatin, epirubicin and pharmacokinetic modulating chemotherapy by 5-FU and enteric-coated tegafur/uracil: a pilot study. World J Gastroenterol 2007;13:5465-5470.
25. Kamiyama T, Nakanishi K, Yokoo H, et al. Efficacy of preoperative radiotherapy to portal vein tumor thrombus in the main trunk or first branch in patients with hepatocellular carcinoma. Int J Clin Oncol 2007;12:363-368.