관련 문서
consumer's behavior behavior behavior behavior of of of of using using using using nail nail nail nail shop shop shop for shop for for women for women
Purpose: Calcaneal fracture is a rare fracture, which accounts for about 2% of all fractures, but is one of the most common fractures in the ankle bone.. There is
The clinical outcome and complication for treating proximal femoral shaft fracture were compared and analyzed through the group treated with closed
82 year-old female patient with traffic accident, (A,B,C) Initial x-rays show open fracture of left distal femur(AO 33-C3, Gustilo-Anderson II) with patella
Nail clipper CD player Vending machine Nail clipper, CD player, Vending machine Mechanical engineering is a field of making a g g g. useful mechanism or machine by using
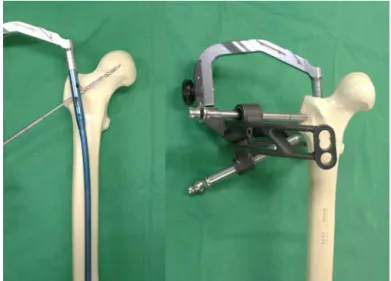
Key Words: Femur, Subtrochanteric fracture, limited open reduction, Proximal femoral nail anti-rotation (PFNA)... 수술 방법 및
No.. ramus insufficiency fracture, B) Thorax and abdomen CT showing multiple spine compression fracture.. ramus insufficiency fracture, B) After 4 months of
Although van der Waals equation is still less accurate at high