625
Print ISSN 1738-5520 / On-line ISSN 1738-5555 Copyright © 2011 The Korean Society of Cardiology CASE REPORT
http://dx.doi.org/10.4070/kcj.2011.41.10.625
Open Access
Delayed Ventricular Septal Rupture Following Blunt Chest Trauma
Na Young Kim, MD
1, Tae Jung Kwon, MD
1, Jeong Rang Park, MD
1, Ho Cheol Choi, MD
2, Yun Hong Cheon, MD
1, Min Kyu Kang, MD
1, Seok-Jae Hwang, MD
1, Yongwhi Park, MD
1, Young-Hoon Jeong, MD
1, Choong Hwan Kwak, MD
1, and Jin-Yong Hwang, MD
11
Departments of Internal Medicine and
2Radiology, Gyeongsang National University Hospital, Jinju, Korea
ABSTRACT
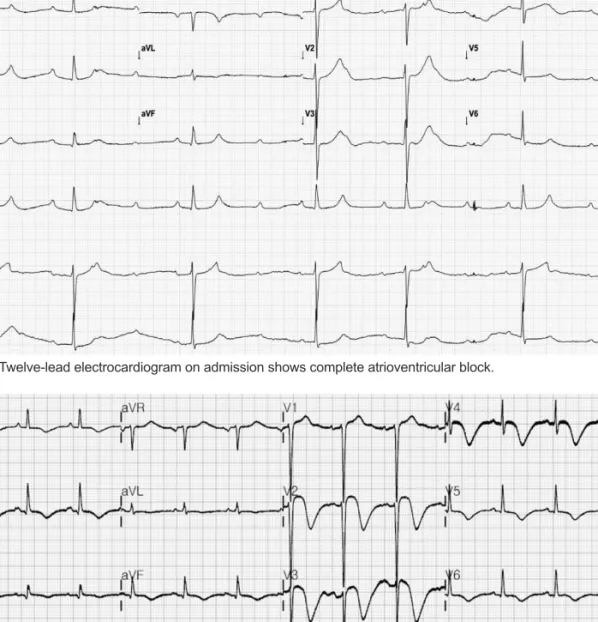
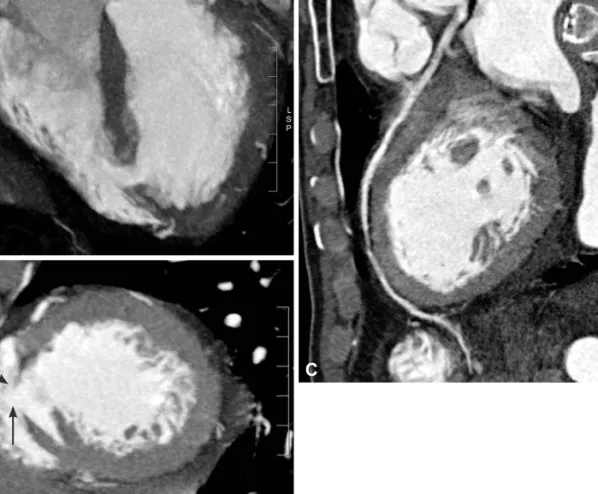
Cardiac injury is a common but occasionally serious complication of blunt chest trauma. A ventricular septal rupture (VSR) is a rare complication and is variable in its presentation, temporal course and severity. Here, we report a rare case of 75-year- old man who developed delayed VSR following blunt chest trauma. (Korean Circ J 2011;41:625-628)
KEY WORDS: Ventricular septal rupture; Thoracic injuries.
Received: December 8, 2010 Revision Received: January 4, 2011 Accepted: January 17, 2011
Correspondence: Jeong Rang Park, MD, Department of Internal Medi- cine, Gyeongsang National University Hospital, 90 Chiram-dong, Jinju 660- 702, Korea
Tel: 82-55-750-8068, Fax: 82-55-755-9078 E-mail: [email protected]
• The authors have no financial conflicts of interest.
cc