뇌졸중 심근경색
위험인자
Hypercholesterolemia Hypertension Diabetes Mellitus Smoking Others
10 20 30 40 50 60 70 80
연령
(세)
증상
(+)
증상(-)
동맥경화의정도
심장질환의 고위험군이란 ?
• 심혈관 질환자 – 특히 급성관동맥증후군
• 당뇨 환자
• 동맥경화성 혈관 질환자
• 매우 심한 정도의 위험인자를 가진 경우
• 많은 위험인자를 가진 경우 ; 3개 이상의 위험인 자를 가진 경우
• 중등도의 위험을 가지고 있으면서 대사성증후군 또는 높은 CRP 수치등을 가진 경우 (optional)
Elderly People are the Major Target for Risk Reduction to Prevent Atherosclerotic Disease
한 기 훈
울산대학교 의과대학 심장내과학교실
• Cigarette smoking
• Hypertension
(blood pressure
≥
140/90 mmHg or on antihypertensive medication)• Low HDL cholesterol
(< 40 mg/dL)†
• Family history of premature CHD
(CHD in male first-degree relative < 55 years; CHD in female first-degree relative < 65 years)
• Age (men ≥ 45 years; women ≥ 55 years)
*Diabetes is regarded as a coronary heart disease (CHD) risk equivalent.
†HDL cholesterol≥ 60 mg/dL counts as a “negative” risk factor; its pres ence removes 1 risk factor from the total count.
Major Risk Factors That Modify LDL Goals * (Exclusive of LDL Cholesterol)
NCEP-III Guideline European Guideline
Distribution of Absolute Risk* of CHD Within 10 Years European Populations
Men Women
<10% 46% 82%
10-20% 38% 16%
20-40% 15% 2%
>40% <1% 0%
* Framingham - Anderson function
Absolute Risk
+
of >20% of CHD Within 10 Year s by Age and Sex European PopulationsYears Men Women
25-34 35-44 45-54 55-64 65-74 25-74
0%
1%
11%
34%
68%
20%
0%
<1%
<1%
3.5%
6.4%
1.6%
+
Framingham - Anderson function
Points 10-Yr-Risk %
한국성인의 총 콜레스테롤 분포
0 2 4 6 8 10 12 14
<130 140- 160- 180- 200- 220- 240- 260-
남자 여자
%
mg/dl
Men = 7.9%
Women=9.6%
자료: 보건복지부. 1998년 국민건강영양조사 자료
연령군별 고지혈증 유병률
0 5 10 15 20 25
30-39 40-49 50-59 60-69 70이상
남자 여자 전체
자료: 보건복지부. 2001년 국민건강영양조사자료
중간요약 (1)
• 고위험군은 주로 (남성) 고령자에게 많이 발견된다.
• 우리나라에서도 고지혈증은 주로 고령에 서 많이 발견된다.
얼마나 낮추어야 하는가 ? : LDL-C Goal
• Very High Risk ; 70 – 100 mg/dl
• High Risk ; 100 mg/dl
• Intermediate Risk ; 130 mg/dl
Distribution of LDL-C Levels in Patients With 2 or More CHD Risk Factors Distribution of LDL
Distribution of LDL- -C Levels in Patients C Levels in Patients With 2 or More CHD Risk Factors With 2 or More CHD Risk Factors
No. of US Adults (millions) No. of No. of US Adults US Adults (millions) (millions)
LDL-C Level, mg/dL (mmol/L) LDL-C Level, mg/dL (mmol/L)
<60
<60--129129 (1.6 (1.6--3.3)3.3)
130 130--159159 (3.4 (3.4--4.1)4.1)
160 160--300300 (4.1 (4.1--7.8)7.8)
NHANES III phase II (1988 NHANES III phase II (1988--1994) data.1994) data.
Adapted from Jacobson TA et al.
Adapted from Jacobson TA et al. Arch Intern MedArch Intern Med. 2000;160:1361. 2000;160:1361--1369.1369.
Mean LDL-C:
139.5 mg/dL (3.6 mmol/L) Mean LDL-C:
139.5 mg/dL (3.6 mmol/L) 0
0 1 1 2 2 3 3 44 5 5
P40
S20
R10
A20
S40
LDL - 30 %
LDL - 45 %
Mt.Goal
A10
스타틴의 용량조절
THREE-STEP TITRATION
10 20 30 40 50 60
% Reduction in LDL Cholesterol 0
-6% -6%
Simvastatin 10 mg
mg20 mg40 mg80-6%
Effect of Statin Therapy on LDL-C Levels: “The Rule of 6”
스타틴의 고용량에서의 주의점
• Myopathy 의 발생이 높은 집단을 이해 !
• 고령 (주로 80세 이상)
• 몸집이 작은 사람
• 당뇨성 신증등 다기관의 질병
• 약물병용
• 알코올 의존 경향
ONE-STEP COADMINISTRATION THREE-STEP TITRATION
10 20 30 40 50 60
% Reduction in
LDL-C0
Statin 10 mg 20 mg
40 mg
80 mg
Statin 10 mg + Ezetimibe 10 mg
새로운 LDL 강하방법 ; Ezetimibe
Rosuva Atorva Simva / EZ Simva Lova / Prava TC LDL-C
5 10 20 22 27
10 20 40 27 34
10 20 40 80 32 41
20 40 10 / 10 80 37 48
40 80 42 55
Dose (mg) of agent % Reduction
Roberts WC. Am J Cardiol. 1997;80:106-107.
Stein E et al. J Cardiovasc Pharmacol Therapeut. 1997;2:7-16.
Rule of 5s & 7s
용량에 따른 LDL 강하효과
S. Int. Rinse S. Int. Wall
L. Int. Rinse L. Int. Wall
Stomach Liver
Pancreas Adrenal
Kidney Lung
Heart Spleen
Teste Serum 0
60 50 40 30 20 10
% IV dose
0.3 mg/kg, 3-hr post-dosing, n=4/group
Tissue
Localization of IV-Dosed
125
I-Gluc-Ezetimibe(SCH 61209) in Normal Rats
중간요약 (2)
• EZ는 장에서의 콜레스테롤 흡수를 선택적 으로 저해한다.
• EZ는 주로 장관에만 분포하기 때문에, 기 타 조직에 미치는 효과가 거의 없다.
Daily Dose of Ezetimibe (mg)
0 5 10 20 40
From Baseline to Endpoint Mean (±S.E.M.) Percent Change in LDL-C -20%
-15%
-10%
-5%
0%
5%
Placebo
Ezetimibe
Results from three Phase II Clinical Therapy Trials
Relationship Between Dose of Ezetimibe and
% Change in Plasma LDL-C EZ + Simvastatin Study: Efficacy on LDL-C
Mean % Change
10 mg EZ 10 mg
+ Simva
10 mg 20 mg 40 mg 80 mg
Simvastatin
* p<0.01 combination therapy versus statin alone
Davidson M et al. ACC 2002: Abstract.
Davidson M et al. ACC 2002: Abstract.
-46 -45
-27*
-36* -38*
-60 -50 -40 -30 -20 -10 0
EZ + Statin Studies: Efficacy on TG
Pooled Results
* p<0.01 combination therapy versus statin alone
Atorvastatin Pravastatin
Simvastatin Lovastatin
Median % Change
*
*
*
*
Davidson M et al. ACC 2002: Abstract.
Ballantyne C et al. ACC 2002: Abstract.
Melani L et al. WCC 2002: Abstract.
Lipka L et al. WCC 2002: Abstract.
-24 -14
-20 -12
-33 -21
-29 -25
-40 -30 -20 -10 0
Statins only + EZ 10 mg/d
Atorvastatin Pravastatin
Simvastatin Lovastatin
4
7 7
4
9* 9**
8
7*
0 2 4 6 8 10
Mean % Change
* p<0.01 combination therapy versus statin alone
** p=0.03 combination therapy versus statin alone
Ezetrol + Statin Studies: Efficacy on HDL-C
Pooled Results
Davidson M et al. ACC 2002: Abstract.
Ballantyne C et al. ACC 2002: Abstract.
Melani L et al. WCC 2002: Abstract.
Lipka L et al. WCC 2002: Abstract.
Statins only
+ EZ 10 mg/d
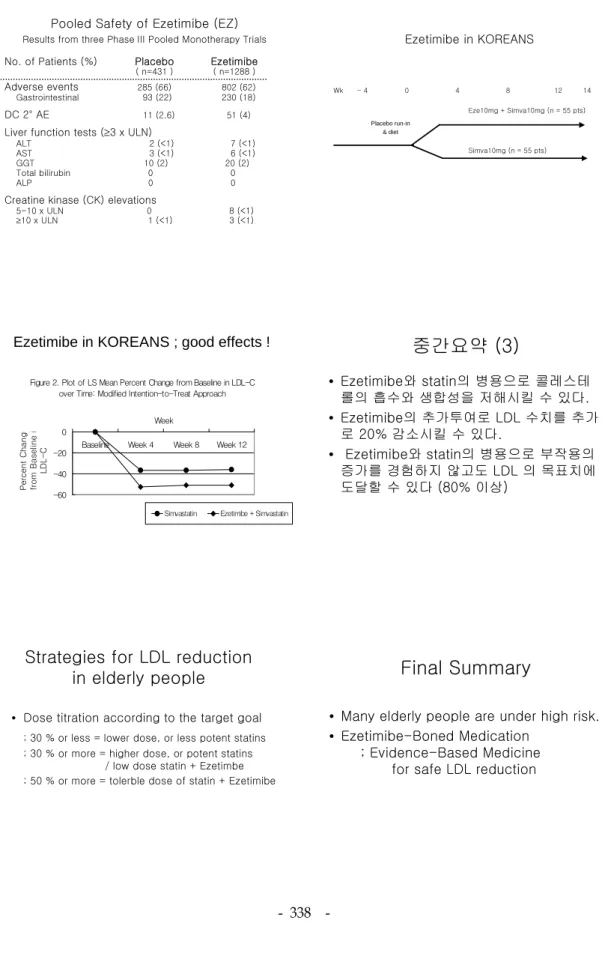
Pooled Safety of Ezetimibe (EZ)
Results from three Phase III Pooled Monotherapy Trials
No. of Patients (%) Placebo Ezetimibe( n=431 ) ( n=1288 )
Adverse events
285 (66) 802 (62)
Gastrointestinal 93 (22) 230 (18)
DC 2° AE
11 (2.6) 51 (4)
Liver function tests (≥3 x ULN)
ALT 2 (<1) 7 (<1)
AST 3 (<1) 6 (<1)
GGT 10 (2) 20 (2)
Total bilirubin 0 0
ALP 0 0
Creatine kinase (CK) elevations
5-10 x ULN 0 8 (<1)
≥10 x ULN 1 (<1) 3 (<1)
Ezetimibe in KOREANS
Wk - 4 0 4 8 12 14 Eze10mg + Simva10mg (n = 55 pts)
Simva10mg (n = 55 pts) Placebo run-in
& diet
Figure 2. Plot of LS Mean Percent Change from Baseline in LDL-C over Time: Modified Intention-to-Treat Approach
-60 -40 -20 0
Baseline Week 4 Week 8 Week 12 Week
Percent Change from Baseline i LDL-C
Simvastatin Ezetimibe + Simvastatin
Ezetimibe in KOREANS ; good effects !
• Ezetimibe와 statin의 병용으로 콜레스테 롤의 흡수와 생합성을 저해시킬 수 있다.
• Ezetimibe의 추가투여로 LDL 수치를 추가 로 20% 감소시킬 수 있다.
• Ezetimibe와 statin의 병용으로 부작용의 증가를 경험하지 않고도 LDL 의 목표치에 도달할 수 있다 (80% 이상)
중간요약 (3)
Strategies for LDL reduction in elderly people
• Dose titration according to the target goal
; 30 % or less = lower dose, or less potent statins
; 30 % or more = higher dose, or potent statins / low dose statin + Ezetimbe
; 50 % or more = tolerble dose of statin + Ezetimibe
Final Summary
• Many elderly people are under high risk.
• Ezetimibe-Boned Medication
; Evidence-Based Medicine for safe LDL reduction