Vol. 11, No. 2, 131-135, 2008
책임저자:윤병민, 서울시 종로구 연건동 28
110-744, 서울대학교병원 성형외과 Tel: 02-2072-0258, Fax: 02-3675-7792 E-mail: [email protected]
이 논문의 요지는 2008년도 제65차 대한성형외과학회 추계학술 대회에서 발표되었음.
관절부위 화상후반흔구축에 있어서 피하경 마름모모양피판의 유용성
윤 병 민
서울대학교 의과대학 성형외과학교실
The Use of Subcutaneous Pedicle Rhomboid Flaps in the Treatment of Postburn Scar Contractures in Joint Regions
Byung Min Yun, M.D.
Department of Plastic and Reconstructive Surgery, College of Medicine, Seoul National University, Seoul, Korea
Purpose: Various surgical techniques have been employed in the treatment of contracture bands, each with its own ad- vantages and disadvantages. The author uses the subcuta- neous pedicle rhomboid flaps which are relatively new in the treatment of scar contractures. This study investigates the use of this flap in joint regions particularly.
Methods: Three cases of linear and wide scar contracture(s) in joint regions were treated with subcutaneous pedicle rhomboid flaps. Rhomboid flaps were designed along the ax- is of the contracture line with 120- and 60-degree angles for the release of the contracture bands, and relaxation incision lines were marked. Rhomboid flaps were incised down to the muscle and freed from the surrounding skin. The emerged skin defects were then sutured with the flaps in V-Y advance- ment along the long axis and in Y-V advancement along the relaxation incisions.
Results: This flaps have three major advantages for the treatment of scar contractures in joint regions. Firstly, the technique is relatively free of distal necrosis when compared with triangular flaps in Z-plasty as no undermining is carried out. The broad subcutaneous pedicles of the flaps are very reliable. Secondly, the lengthening provided by this flaps is longer that a Z-plasty with 60-degree, which is the best angle to generate adequate central limb lengthening under equal tension. Lastly, the minimal distortion of the surrounding skin in this technique is more favorable to joint movements.
Conclusion: The subcutaneous pedicle rhomboid flaps can be chosen primarily for various types of postburn scar con-
tractures in joint regions. (Journal of Korean Burn Society 2008;11:131-135)
Key Words: Subcutaneous pedicle, Rhomboid flaps, Post- burn scar contracture, Joint reconstruction
서 론
화상후반흔구축(Postburn scar contracture)은 초기의 적 절한 치료에도 불구하고 비교적 흔하게 발생할 수 있는 합 병증이다1). 이에 대하여 제각의 장단점들을 가진 여러 가지 수술적 치료법들이 시행되고 있다. 우선 피부이식술은 폭 넓은 적응증을 가지고 고전적으로 사용되고 있는 수술법이 지만 화상 반흔 위에 시행하게 되므로 이식피부의 생착이 쉽지 않고 피부 공여부에 흉을 남길 뿐만 아니라 소아의 경우 성장에 따른 수차례의 수술적 치료를 요할 수 있다.
그리고 조직확장술은 환부를 덮을 확장된 조직이 반흔 주 변부에서 오므로 미용상 탁월한 결과를 얻을 수 있으나 반 흔 부위가 넓은 경우 역시 수차례 확장술을 시행 하여야 한다2). 한편 국소피판술은 수술방법이 비교적 쉽고 간단하 다. 반흔구축 치료에는 일반적으로 Z-성형술이 사용되고 있는데 박리된 피판 끝이 괴사되는 수가 적지 않은 것과 2개 이상 다수의 반흔구축들이 서로 평행하게 인접하고 있 거나 넓은 형태를 띠고 있는 경우는 사용할 수 없는 단점이 있다. 이에 대해서 비교적 최근에 소개된 또 다른 국소피판 술인 피하경 마름모모양피판(subcutaneous pedicle rhom- boid flap)은 Z-성형술에 비하여 피판 생착이 우수하고 길이 신장 정도가 더 우수하며 직선형 단일 반흔구축 이외에 어 떤 형태의 경우라도 사용될 수 있다3). 여기에서 저자는 이 피하경 마름모모양피판이 관절부위의 화상후반흔구축에 대 한 선택치료로서 사용될 수 있는지를 알아보고자 하였다.
대상 및 방법 1. 대상
2007년 3월부터 2008년 8월까지 서울대학교 어린이병원
Table 1. Summary of Clinical Cases
Number Age/Sex Location of contracture Cause of contracture Number of contracture Result
1 24 Mo/M Hand (Palm, 1st, 2nd, 3rd finger) Burn Multiple Released
2 5 YR/M Wrist Skin graft Single Released
3 5 YR/M Hand (1st web space) Skin graft Single Released
YR = year, Mo = month, M = male
Fig. 1. Schematic illustration of the operation technique of the subcutaneous pedicle rhomboid flap in the treatment of scar contractures in joint regions. (A) The preoperative design: the tension line is parallel to 60-degree inner angles and perpendicular to 120-degree inner angles. (B) Incision: the relaxation incisions should be made outwardly from the points of blunt angles. (C) After incision:
relaxation incisions elongate the tension line and free the rhomboid flap. (D) Suture: the rhomboid flap suture resurfaces skin defect in V-Y advancement along the tension line and Y-V advancement along the relaxation incisions (From Ertas NM, Bozdogan NB, Erbas O. Comparison of Elongations provided by subcutaenous pedicle rhomboid flap and z-plasty in rat inguinal skin. Plast Reconstr Surg 2006;117:486-490).
Fig. 2. (A) Linear contracture band located on the 1st finger web space. (B) Rhomboid flap was freed from the surrounding skin and the relaxation incisions lengthened the contracture. (C) 4 months postoperative view of the reconstructed 1st web space.
Fig. 3. (A) Linear contracture band located at the dorsum of wrist. (B) Relaxation incisions elongate the tension line and free the rhomboid flap. (C) 3 months postoperative view of the reconstructed wrist.
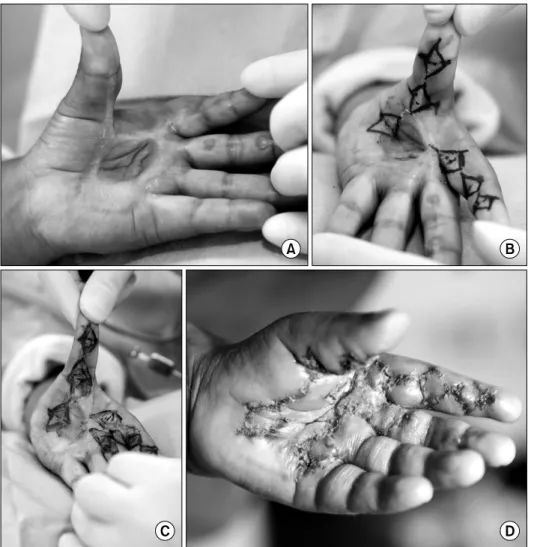
Fig. 4. (A) Multiple long linearr contracture bands located on thumb, index finger and long finger respectively with a wide scar contracture on palm. (B) Design of multiple rhomboid flaps.
(C) Consequent subcutaneous pe- dicle rhomboid flaps released the whole bands. (D) 2 weeks post- operative view of the reconstructed fingers and palm.
절반에서 최대 전체의 길이까지 가능하다. 절개깊이는 아 래로 건강한 피하 혹은 근막까지로 한다. 마름모 모양의 절 개를 마치게 되면 피판은 도서형(island)모양이 되어 주위 의 장력이 있는 피부로부터 자유롭게 되어 어느 정도 수축 이 일어난다. 그리고 둔각의 양꼭지점으로부터 마름모의 바깥으로 각각 이완절개(relaxation incision)를 시행하는데
절개의 길이는 수축된 피하경 마름모모양피판과 양측을 Y-V 봉합하는 데에 장력이 발생하지 않을 정도로서 수술자 가 결정 한다. 수축된 피판의 네 변들과 이완절개로 얻어진 여덟 개의 절개 면들 사이의 창상(raw surface)을 봉합할 때에는 장축을 따라서는 V-Y 전진피판술로 하고 이완절개 된 면을 따라서는 Y-V 전진피판술로 처리하며 피판 경계부
Table 2. Clinical Indications of Subcutaneous Pedicle Rhomboid Flap (SPRF) with Other Surgical Treatments in the Treatment of Scar Contractures in Joint Regions
Scar contracture in joint regions
First web space Wrist Palm Interphalangeal joint
Characteristics of scar contracture
Linear Linear Wide, often quadratic Longer linear
- Blood supply is limited.
- A sufficient contracture lengthening for full ROM is necessary.
- No displaced natural creases (anatomical landmark) in joint region is desirable.
Skin graft Possible Possible Possible Possible
Tissue expansion Possible Possible Difficult Difficult
Free flaps Possible Possible Possible Possible
Z-plasty Good Good Good Good
SPRF Better Better Better Better
고 찰
화상후반흔구축의 수술적 치료법은 피부이식술, 조직확 장술, 유리피판술, 국소피판술 등으로 다양하다. 이중 국소 피판술이 다른 방법에 비해 비교적 간단하며, 직선형 반흔 구축에 대해서는 Z-성형술이 대표적으로 시행되고 있지만 이를 응용한 복합(multiple) Z-성형술, 다섯피판(five-flap) 성형술 등도 있다. 문제는 반흔구축의 주변조직도 역시 반 흔조직이어서 국소피판 생착시 혈행 장애로 인하여 피판 끝이 괴사될 위험성이 크다는 점이다. 이에 대하여 1990년 Copper의 복합 Y-V 성형술4), 1991년 Grishkevich의 Trepe- zeplasty와 Olbrisch의 runing Y-V 성형술5), 그리고 변형된 다중 Y-V 성형술이 발표되었다. 한편 Barron과 Emmet가 피하경(subcutaneous pedicle)을 기반으로 하는 임의형 (randome)피판을 처음으로 피하경피판(subcutaneous pedi- cle flap)이라 명명한6) 이후 1987년 Suzuki가 회전피판 형식 의 피하경피판을 처음으로 화상반흔부위 치료에 사용하였 다7). 이는 피판의 혈행이 넓은 피하경을 기반으로 하기 때 문에 피판생착이 비교적 안전하게 되었다는 데에 의의가 있다8). 1994년에 Uzunismail은 Y-V 전진피판의 형식으로 피하경 마름모모양피판을 처음으로 화상반흔부위 치료에 사용하였는데 이는 피판 끝의 박리가 필요 없기 때문에 피
피판 길이의 연장 정도는 쥐를 가지고 한 동물실험에 따 르면 단일(single) 피하경 마름모모양피판이 104%의 신장 률(elongation rate)을 갖는다(p<0.001)고 보고하고 있으며, 이를 실제 임상에 적용한 경우는 75∼90%의 길이 연장 효 과가 있다(p<0.001)고 한다. 이는 실험동물에서는 건강한 조직이지만 임상에서는 화상반흔구축으로 조건에 차이가 있다고 설명하고 있다. 또한 최대로 늘어날 수 있는 60도 Z-성형술보다도 피하경 마름모모양피판의 늘어나는 정도 가 더 우수하다(p<0.001)고 보고하고 있다10).
피하경 마름모모양피판 술기에서 각별히 주의할 점은 첫 째, 마름모모양 피판의 절개면을 깊이에 상관없이 수직방 향으로 하거나 깊어질수록 바깥쪽으로 경사(bevel)지게 하 여야 한다. 만일 안쪽으로 경사지게 되면 피판 끝이 괴사가 될 수 있다. 둘째, 피판의 조직박리(undermining)는 절대로 시행하지 않는다. 셋째, 이 피판의 신장 기전이 Z-성형술에 서와는 다르게 마름모의 내각이나 피판의 두께에 있는 것 이 아니라 이완절개에 있으므로 반드시 이를 시행해야 한 다.
피하경 마름모모양피판(subcutaneous pedicle rhomboid flap)이 기존 수술적 치료법들과 다르게 갖고 있는 장점들 을 다음과 같이 열거해볼 수 있다. 먼저 피부이식술은 화상 반흔 위에 시행하게 되므로 이식피부의 생착이 쉽지 않고 피부 공여부에 흉을 남길 뿐만 아니라 소아의 경우 성장에
따라 여러 번 수술을 해야 할 수 있다. 반면 피하경 마름모 모양피판은 피판박리없는 전진피판이므로 혈행이 풍부하 며, 반흔구축 위에서 시행됨으로 추가의 흉을 만들지 않는 다. 조직확장술은 환부를 덮을 확장된 조직이 반흔 주변부 에서 왔으므로 미용상 탁월한 결과를 얻을 수 있는데 문제 는 늘어나는 정도에 한계가 있어서 반흔 부위가 넓은 경우 역시 수차례 확장술을 시행 하여야 한다. 반면 피하경 마름 모모양피판은 늘어나는 정도가 그 어떤 피판에 비해서 탁 월하며 수술전 특별한 준비없이 바로 시행할 수 있으며 얼 굴과 관절을 포함하여 온몸에 적용할 수 있다. 직선형 반흔 구축에 대해서 일반적으로 사용되고 있는 국소피판술인 Z- 성형술은 양측 삼각형(triangle)피판을 거상하기 위해 피판 의 기저부(base)에서 끝(tip)까지 근막하층(subfascial layer) 레벨로 박리(undermining)한 후 거상된 피판을 재배치 시 켜준다. 이 과정에서 주변조직이 끌어당기게 되어 반흔구 축의 힘이 재배치되며 또한 길이연장 효과를 얻게 되나, 피 판 거상 중 필연적으로 조직의 박리를 하여야 하므로 혈행 악화로 피판 일부가 괴사될 가능성이 있다. 또한 피판을 재 배치시키므로 해부학적 위치(예, 액와부의 털, 유두부위 등) 가 변한다. 피하경 마름모모양피판이 Z-성형술과 근본적으 로 다른 점은 피판의 거상이라는 동작이 필요 없고 따라서 피판의 재배치의 과정을 시행하지 않으므로 피판의 혈행이 악화되어 괴사될 가능성이 거의 없으며, 그 자리에서 봉합 을 다시 하기 때문에 해부학적인 위치가 변하가 되지 않는 다. 또한 피판의 이동이 없으므로 색깔과 피부 역시 수술 전과 일치하게 되는 장점이 있다. Z-성형술은 2개 이상 다 수의 반흔구축이 서로 평행하게 인접하고 있는 경우는 사 용할 수 없지만 여러 개의 직선형 반흔구축이 평행하게 있 더라도 한 개의 피판으로써 이완이 가능하다11). 무엇보다도 가장 우수한 점 중의 하나는 반흔구축이 재발한 경우에도 다시 처음 디자인대로 절개를 가해 재차 수술할 수 있다는 점이다. 하지만 Z-성형술로 치료한 경우에는 Z-성형술 이 외의 다른 국소피판이나 피부이식을 해야만 한다. 마지막 으로 유리피판술은 수술 자체가 기술적으로 어렵고 고비용 이지만 피하경 마름모모양피판은 디자인이 간편하고 수술 법이 비교적 용이하다.
관절부위 화상후 반흔구축의 특징은 피판생착을 위한 혈 행 조건이 좋지않고 일반적으로 관절운동의 제한을 가져오 는 긴 줄 모양 혹은 여러 줄이 넓게 펼쳐진 모양을 갖는다 는 점이다. 손가락관절, 손가락사이관절, 손바닥관절, 손목 관절 등에 있는 반흔구축을 수술적으로 치료하기 위한 피 하경 마름모모양피판(subcutaneous pedicle rhomboid flap)
과 기존 수술적 치료법들의 적응증을 요약하면 Table 2와 같다.
결 론
관절부위의 화상후 반흔구축 치료를 위한 피판은 기본적 으로 혈행이 우수한 피판이어야 할 뿐만 아니라 피부신전 정도가 관절운동 범위(full ROM)를 충분히 회복시킬 수 있 는 수준으로 탁월해야하며 관절부위 피부주름이 흐트러지 지 않도록 하는 것을 요구한다. 저자는 피하경 마름모모양 피판이 이런 조건들을 모두 만족시킬 수 있으므로 관절부 위의 화상후반흔구축에 대한 선택치료로서 사용될 수 있음 을 알 수 있었다.
REFERENCES
1) Lee YH, Lee SW, Lee ET. Use of bipedicled flap in treatment of burn scar contracture. J Korean Burn Soc. 2003;6:28-32.
2) Lee YH, Lee SJ, Lee ET. Varieous local flaps in the treatment of burn scar contracture. J Korean Burn Soc. 2000;3:22-28.
3) Ertas NM, Kucukcelebi A, Bozdogan NB. The use of subcutaneous pedicle multiple rhomboid flaps in the treatment of long postburn scar contractures. Burns. 2004;30:
594-599.
4) Cooper MACS. The multiple Y-V plasty in linear burn scar contracture release. Br J Plast Surg. 1990;43:145-149.
5) Olbrisch RR. Running Y-V plasty. Ann Plast Surg. 1991;26:
52-56.
6) Barron JN, Emmett AJ. Subcutaneous pedicle flaps. Br J Plast Surg. 1965;18:51.
7) Suzuki S, Isshik N, Kshileawa K, et al. The use of sub- cutaneous pedicle flaps in the treatment of postburn scar contractures. Plas Reconstr Surg. 1988;80:792-798.
8) Yang HW, Kang MG, Seo SW. Correction of axillary burn scar contracture with seven-flap plasty: a case report. J Korean Burn Soc. 2007;10:157-160.
9) Uzunismail A, Kahveei R, Ozdemir A, et al. The rhomboid release: a new approach to the management of digital burn contractures. Ann Mediterran Burns Club. 1994;8:94-97.
10) Ertas NM, Kucukcelebi A, Erbas O, et al. Comparison of elongation provided by subcutaneous pedicle rhomboid flap and Z-plasty in rat inguinal skin. Plast Reconstr Surg.
2006;117:486-490.
11) Ertas NM, Bozdogan NB, Erbas O. The use of subcutaneous pedicle rhomboid flap in the treatment of postburn scar contractures. Ann Plast Surg. 2004;53:235-239.