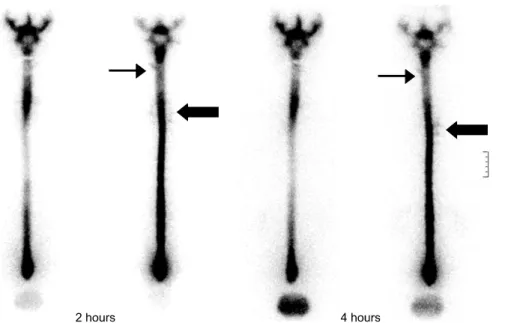
Epidural Blood Patches in a Patient With Multi-level Cerebrospinal Fluid Leakage That Was Induced by Spontaneous Intracranial Hypotension
5
0
0
전체 글
(2)
(3)
(4)
(5)
수치
관련 문서
Second, as a result of surveying the necessity of multi-cultural education, it was discovered that most of the subjects responded affirmatively, especially,
Relaxation effects of active tension by propofol on spontaneous activity(S.A) and oxytocin(OT) induced contractions of rat uterine myometrium..
Effects of Nitroglycerin(Ni) on Spontaneous Activity(S.A) and Oxytocin (OT) Induced Contractions in the Uterine Smooth Muscle. Data are expressed as mean
Second, analyzing students' level of interest in the unit of Clothes and Life Style revealed that there was significant difference between genders and students in the two
In this study, we found that Pin1 plays a pivotal role in insulin- induced AP-1 activation through its interaction with p70S6K and prolongs activity of
• In any flow of a barotropic inviscid fluid, the circulation about any closed path does not vary with time if the contour is imagined to move with the fluid, that is, always to
- Turbulence is generated primarily by friction effects at solid boundaries or by the interaction of fluid streams that are moving past each other with different velocities
n The magnitude of the buoyant force acting on a floating body in the fluid is equal to the weight of the fluid which is displaced by
