Vol. 19, No. 3, December, 2011
□ 원 저 □1)
접수 :2011년 7월4 ,일 수정:2011년8월 6일 승인 :2011년 10월 10일
책임저자 : 채종희 서울대학교 의과대학 소아과학교실, Tel : 02)20727-3622, Fax : 02)743-3455 E-mail : chaeped1@snu.ac.kr
서 론
혈구탐식성 림프조직구증식증(hemophagocytic
혈구탐식성 림프조직구증식증의 신경계 증상과 예후
서울대학교 의과대학 소아과학교실* 순천향대학교 의과대학 소아과학교실 ,
†류혜원* 두기현ㆍ * 김승수ㆍ †ㆍ임병찬* 황 희ㆍ * 김기중ㆍ * 황용승ㆍ * 채종희ㆍ *
= Abstract =
Neurologic Manifestations and Prognosis in Hemophagocytic Lymphohistiocytosis
Hye Won Ryu, M.D.*, Ki Hyun Doo, M.D.*, Seung Soo Kim, M.D.
†, Byung Chan Lim, M.D.*, Hee Hwang, M.D.*, Ki Joong Kim, M.D., Ph.D.*,
Yong Seung Hwang, M.D., Ph.D.* and Jong-Hee Chae, M.D, Ph.D.*
Department of Pediatrics, College of Medicine, Seoul National University*
Departments of Pediatrics, College of Medicine, Soonchunhyang University, Cheonan† Purpose : Hemophagocytic lymphohistiocytosis (HLH) presenting with neurologic mani- festationhas a poor prognosis due to delayed diagnosis and treatment. We investigated the time between onset of symptoms and diagnosis of HLH and clinical findings and outcome in patients with HLH presenting with neurologic manifestation.
Methods : We retrospectively assessed 24 patients with HLH in Seoul National University Children s Hospital from January 2002 to December 2010. Sex, age on diagnosis, symptoms,’ laboratory findings, time between onset of symptoms and diagnosis of HLH, cerebral spinal fluid (CSF) findings and brain magnetic resonance imaging (MRI) findings were reviewed.
Results : At diagnosis, 7 children (29.2%) had neurologic symptoms, including seizure (n=6) and right side weakness (n=1). Time to diagnosis from onset of symptoms ranged between 7 and 385 days in patients with neurologic symptoms and between 2 and 87 days in patients without neurologic symptoms. Five patients had brain MRI abnormalities; radio- logic findings were multiple high signal intensity lesions on T2-weighted image (n=3), focal high signal intensity lesion followed by severe cerebral edema (n=1), and diffuse cerebral atrophy (n=1).Of these 7 patients, 4 died, 1 underwent stem cell transplantation and was followed, 1 was followed after completion of therapy without neurologic sequelae, and 1 is still under treatment and has mild neurologic sequelae.
Conclusion : HLH presenting with neurologic manifestation is difficult to distinguish from other diseases because of nonspecific symptoms and imaging findings. However, HLH is treatable with chemotherapy and stem cell transplantation, so it is important to consider HLH in a patient with neurologic disease that is unresponsive to treatment and accompanies systemic symptoms.
Key Words : Hemophagocytic lymphohistiocytosis, Demyelinating disease, Central nervous system
이하 은 간 비장 림프 lymphohistiocytosis, HLH) , , 절 골수 및 중추 신경계 등 여러 장기에 조직구가, 침윤하여 발열 비비대 혈구 감소 고 중성지방혈증, , , 혹은 저 섬유소원혈증 혈중, ferritin의 상승 등을 주 로 나타내는 드문 질환으로 가족성 HLH와 후천
의 두 가지 형태로 나눌 수 있다
HLH 1, 2).가족성과
후천성 HLH모두 중추신경계를 침범할 수 있고 보 챔 경련 뇌신경 마비 뇌압 상승 및 의식 저하 등의, , , 다양한 비특이적 신경계 증상으로 나타날 수 있다3,
4).신경계 증상으로 발현한 경우 증상이 비특이적이 고 뇌, MRI 소견도 다양하며 다른 질환들과 감별이 어려운 경우가 드물지 않아 진단이 늦어지는 경우들 이 있으며5),중추신경계를 침범한 경우 불량한 예후 를 나타낸다고 알려져 있다6).
본 연구에서는 HLH로 진단받은 24명의 환자를 대상으로 임상 증상 발병부터 진단까지의 기간 뇌, , 신경 영상 치료결과 등을 조사하였고 이중 진단 당, , 시 또는 경과 중에 신경계 증상이 주 증상이었던 환 자 7명의 신경학적 임상양상을 분석하고 예후와의 상관관계를 알아보고자 하였다.
대상 및 방법
년 월부터 년 월까지 서울대학교 어 2002 1 2010 12
린이병원 소아청소년과에서HLH로 진단된 24명의 환자를 대상으로 하였고 이들의 성별 및 진단 시 연, 령 임상 증상 및 검사소견 치료 시작일 임상경과, , , 등을 후향적으로 조사 분석하였다, .
의 진단은 진단 지침에 따라
HLH HLH-2004 7)
분자유전학적 검사로 확진되거나 발열 비비대 혈, , , 구감소 고 중성지방혈증 혹은 저 섬유소원혈증 악, , 성의 증거 없이 골수 비장 혹은 림프절에 혈구포식, , 자연세포독성세포(NK-cell)활성도 저하 혹은 결핍, 혈중ferritin의 상승 가용성, CD25의 상승 중5가 지 이상 만족하는 경우로 하였다.
뇌척수액 검사는 백혈구 5/mm3 이상으로 상승되 어 있거나 단백이45 mg/dL 이상으로 상승되어 있 는 경우 비정상으로 분류하였고 영상검사로는 뇌,
혹은 뇌 를 시행하였다
MRI CT .
환자들의 임상양상은 진료기록을 후향적으로 고 찰하였고 치료결과는 항암화학요법 종료, 1년 후까 지 재발이 없는 경우를 치료 종결로 정의하였으며, 수술 말초혈액조혈모세포이식 골수이식 받은 경우, , 와 현재 치료 진행 중인 경우를 별도로 표시하였다.
결 과
환자의 전반적 임상 양상 1.
명의 환자 중 명이 남자 명이 여자였고
24 13 , 11 ,
진단 시 연령은 평균 세4 (2개월-12세 개월 이었5 ) 다 진단 당시에 신경학적 증상이 있던. 7명의 환자 중에는 남자가 명 여자가 명이었고 진단 시 연령4 , 3 , 은 평균 4세 8개월(1세 7개월-12세 5개월 이었) 다 이 중 첫 증상으로 신경계 증상을 나타낸 환자는. 명이었고 나머지 명은 병의 경과 중 신경계 증상
4 , 3
이 동반 되어24명의 환자 중에서 명이 진단 시 또7 는 경과 중에 신경계 증상이 있었고 신경계 증상이, 없었던 환자17명 중 혈소판 감소증 례를 제외하고1
명 모두 발열이 첫 증상이었다
16 (Table 1).
진단 시 신경계 증상이 있었던 환자군과 그렇지 않은 환자군에서 발병 일부터 진단 일까지의 기간은 각각 일에서7 385 (일 중앙값; 40 ), 2일 일에서 87일 중앙값 일 이었다 명의 환자 중 명의 환자 ( ; 14 ) . 24 7
가 사망하였고, 2명이 말초혈액조혈모세포 이식, 1 명이 골수이식을 받았고, 1명이 치료 진행 중이며, 1 명의 환자에서는 치료 없이 증상이 호전되었고 나머 지12명의 환자는 치료 후 년 이상 재발 없어 치료1 종료하였다.
신경계 증상을 동반한 명의 임상 양상
2. 7 ,
검사 결과 및 치료 결과 임상 양상
1)
환자들의 신경계 증상으로는6명에서 경련이 있 었고, 1명의 환자는 우측 상하지 근 위약을 보였다. 환자 은 전신 긴장 간대 발작으로 내원하여 시행한1 뇌 MRI 상 급성 파종성 뇌척수염(acute dissemi- natedencephalomyeletis, 이하ADEM)으로 진단
되어 스테로이드 치료 후 호전되었다가 신경학적, 증상의 재발과 함께 발열 혈구감소 비장비대 등의, , 전신증상이 동반되어 첫 증상이 발현한지128일 만 에 진단되었고 환자 는 우측 상하지 근 위약을 보, 4 여 시행한 뇌 MRI 상 혈관염에 의한 경색 혹은 이 의심되어 스테로이드 치료 후 호전되었으 ADEM
나 개월 후 다시 발열 비비대 혈구 감소를 동반한9 , , 우측 상지의 근 위약과 복합부분발작을 나타내었다.
당시 골수 생검 시행하였고 판독상 림프종 의심된다 고 하였으나 함께 시행한 간 조직 검사 및 임상양상 이 림프종과 맞지 않고 혈구 감소는 호전되어 퇴원 하였다 퇴원. 3개월 후 의식저하와 함께 발열 비비, 대 혈구 감소 등의 전신 증상 동반되어 첫 증상 후, , 일 만에 로 진단받았다 환자 의 경우 첫
385 HLH . 5
증상으로 발열 없이 경련이 발생하여 경련 조절하며
경과관찰 중 잘 조절되지 않는 경련과 함께 시간이 경과하며 발열 비비대 혈구 감소 동반되었고 당시, , , 시행한 뇌 CT상 우측의 심한 뇌 부종과 뇌 이탈을 보여 응급 수술 두개 절제술 및 우측 측두엽 절제( 술 을 시행하였다 뇌 조직검사상) . HLH에 합당한 소 견 보여 진단되었다(Table 2).
뇌척수액 검사 2)
진단 시 신경계 증상이 있었던 7명의 환자 중, 4 명에서 뇌척수액 검사를 시행하였으며 명 모두에서4 단백 증가 소견이 있었고, 3명에서 백혈구 증가 소 견이 관찰되었다(Table 3).
영상 검사 3)
명 중 명의 환자에서 뇌 혹은 뇌 를 시
7 6 MRI CT
행하였다. 3명의 환자에서T2 강조영상에서 고신호 강도를 보이는 다발성 혹은 미만성의 병변이 관찰되 Table 1. Characteristics of 24 Patients with HLH
Patient Sex Age at Dx.
(mo) Initial manifestation
Time to Dx from onset
(days)
Outcome
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
F F M F M M M F F M M M F M M M F F F F F M M M
30 40 19 84 47 149
26 33 2 27 85 104 3
mo
53 21 8
mo
97 35 66 5 45 35 44 84
Seizure Seizure Fever, (Seizure) Right side weakness
Seizure Fever, (Seizure) Fever, (Seizure)
Fever
Prolonged thrombocytopenia Fever, pancytopenia
Fever, melena Fever Fever
Fever, abdominal distension Fever
Fever Fever Fever Fever, rash Fever, rash
Fever Fever, Fever Fever, rash
128 10 34 385 40 45 7 11 87 7 2 13 11 5 7 22 28 34 18 35 38 9 14 24
Died Died Died Post-PBSCT Op.done, Treatment ngoing
Off therapy Died Off therapy
Died Died Died Off therapy Post-PBSCT
Off therapy Off therapy Post-BMT Off therapy Off therapy Off therapy Off therapy Off therapy Off therapy Off therapy Spontaneous recovery
었고(Fig. 1, 2, 4), 발병 당시 시행한 뇌 MRI 상 강조영상에서 국소적인 고신호강도만을 보였으 T2
나37일 후 경련이 지속되어 시행한 뇌CT 상에서 는 심한 뇌부종과 뇌 이탈 소견을 보인 경우가 1명 진단 당시 시행한 뇌 상에는 이상소견 (Fig. 5), CT
이 없었으나 치료 시작 주 후 시행한 뇌3 MRI 에서 광범위한 뇌 위축을 보인 경우가1 (Fig 3),명 정상 소견을 보인 경우가 1명이었다.
분자유전학 검사 4)
신경계 증상이 동반된 환자 중 명에서4 perforin
Table 2. Characteristics of 7 HLH Patients with Neurologic Manifestation
Patient
No. Sex
Age at Diagnosis
(mo)
Time to Diagnosis from onset (days)
Initial
manifestation Fever Cytop- enia Spleno-
megaly Triglyceride↑
Fibrinogen
± ↓ Hemophago-
cytosis Ferritin↑ Treatment Outcome
1 2 3 4 5
6 7
F F M F M
M M
30 40 19 84 47
149 26
128 10 34 385
40
45 7
Seizure Seizure Fever, seizure
Right side weakness Seizure
Fever, seizure Fever, seizure
+
+
+
+ +
+
+
+
+
+
+
+
+
+
+
+
+
+
+
-
+
-
+
+
+
+
+
+
-
+
+
+
+
+ -
-
+
+
+
+
+
+
Chemotherapy Chemotherapy Chemotherapy Chemotherapy,
PBSCT Operation, chemotherapy
Chemotherapy Not done
Died Died Died Post-PBSCT
treatment ongoing, sequalae(+) ; left hemiplegia Off therapy Died before treatment
Table 3. CSF and Radiologic Findings and Genetic Analyis in 7 HLH Patients with Neurologic Manifestation
Patient No. CSF
MRI and CT findings Gene study WBC (/mm3) Protein (mg/dL)
1 2 3 4 5 6 7
15 36
130
101 MRI ; multiple T2 high SI lesion MRI ; multiple T2 high SI lesion
MRI ; diffuse brain atrophy MRI ; multiple T2 high SI lesion
CT ; severe cerebral edema MRI ; normal
Not done
UNC13D mutation(+) Not done Not done UNC13D mutation(+)
No mutation No mutation Not done Not done
Not done 20
4
203 68 Not done
Fig. 1. A and B. (A) Axial fluid attenuated inver- sion recovery (FLAIR) image of the first patient at initial presentation with seizure shows multi- focal patch high signal intensity lesions. (B) Three months later, axial FLAIR image shows pro- gressed cerebral atrophy and diffuse high signal intensity lesion.
Fig. 2 A and B. (A) T2-weighted axial image of the second patient at onset shows prominent leptomeningeal enhancement. (B) Axial FLAIR image 4 days after beginning of chemotherapy shows diffuse high signal intensity lesion in both globus pallidus and dorsal thalamus and deep white matter.
1 gene (PRF1), hMunc13-4 gene (UNC13D), 을 분석한 결과
syntaxin-11 gene (STX11) , UNC13D
의[c.754-1G>C]+[c.1055+1G>A] 복합이형접합 자 돌연변이 환자( 1)와UNC13D의[c.1693delG]+
복합이형접합자 돌연변이 환자 [c.2954+5G>A] ( 2) 가 확인되었고 나머지, 2명은 돌연변이가 보고되지 않았다.
치료 결과 5)
명의 환자 중에서 명이 사망하였고 명이 말
7 4 , 1
초조혈모세포이식을 받은 후 신경학적 후유증 없이 개월간 추적 관찰 중이며 명은 치료 종결 후 재
11 , 1
발이나 후유증 없이 6년간 추적 관찰 중이다 진단, 전 뇌 부종으로 두개 절제술 및 우측 측두엽 절제술 을 시행하였던 명은1 10개월간 재발 없이 항암치료 하며 추적 관찰 중으로 동반된 좌측 편마비는 재활 운동 후 하지는 정상으로 회복되었고 상지의 미세 운동 부전만 남겨진 상태이다.
고 찰
는 발열 비비대 혈구감소 고 중성지방혈증
HLH , , ,
혹은 저 섬유소원혈증 혈중, ferritin의 상승 등을 특 징으로 하는 드문 질환으로 여러 장기를 침범하며 드물지 않게 중추신경계를 침범하는 것으로 알려져 있다. 92명의HLH환자를 대상으로 시행한 한Yang 등8)의 연구에서는 43 (47%)명 의 환자가 진단 시에 신경계 증상 뇌척수액의 이상소견 혹은 뇌 영상검, , 사상의 이상으로 나타나는 중추신경계의 침범이 있 었다고 보고하였다. Horne등6)은193명의HLH환 자를 대상으로 신경계 증상 뇌척수액의 이상과 장, 기예후를 조사하였는데 진단 시 신경계 증상을 나타 내는 경우는37%, 신경계 증상 혹은 뇌척수액의 이 상소견이 있는 경우는 63%에 달하였고 신경계 증, 상과 뇌척수액의 이상소견이 있을 경우 신경계 증상 이 없고 뇌척수액 소견이 정상인 환자군에 비해 사 망률이 높았다고 보고하였다. 34명의 HLH 환자를 대상으로 한 Haddad 등3)의 연구에 따르면 신경계 증상 뇌척수액의 이상소견 혹은 뇌 영상검사상의, , 이상을 모두 포함시켜 중추신경계 질환으로 보았을 때 중추신경계 침범이73%에 이를 정도로 흔하다고 보고한 바 있다.
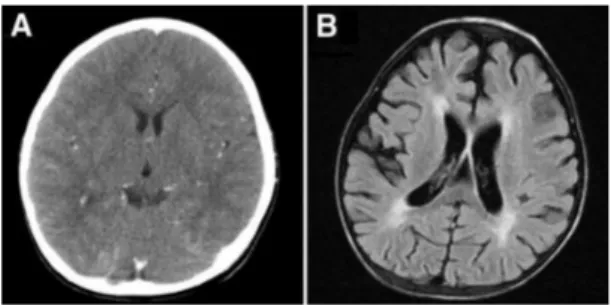
Fig. 3 A and B. (A) Computed tomography (CT) image of the third patient at diagnosis shows normal findings. (B) Three weeks later, axial FLAIR image shows diffuse brain atrophy with periventricular edema.
Fig. 5 A and B. (A) T2-weighted axial image of the fifth patient after initial presentation with seizure shows focal high signal intensity in an- terior limb of right internal capsule. (B) One month later, he visited hospital due to status epilepticus, and CT image shows severe bilateral cerebral edema.
Fig. 4 A and B. (A) Axial FLAIR image of the fourth patient after she presented with a second episode of right arm weakness shows multifocal high signal intensity lesions. (B) Three months later, axial FLAIR image shows diffuse high sig- nal intensity lesion in bilateral periventricular white matter
본 연구에서는 병의 발병 시 또는 경과 중에 신경 계 증상을 나타낸 환자들에서 뇌MRI 및 관련 뇌척 수액 소견 등을 고찰하였고 이중 진단 시 신경계 증, 상이 있는 경우는29.2% (7/24)를 차지하였다 이. 중 4 (4/7, 57.1%)명 이 사망하였고 신경계 증상을, 나타내지 않았던 17명의 환아 중에서는 3 (3/17명 이 사망하여 통계적 유의성을 얻기는 어렵지 17.6%)
만 신경계 증상이 있는 경우 사망률이 더 높은 경향, 을 보였다 진단 당시에 신경계 증상이 있는 경우 그. 렇지 않은 환자군에 비해 증상 발현부터 진단 및 치 료 시작까지의 기간이 길어지는 경향을 보였으나 평( 균 92.71일VS 21.47 )일 통계적은 유의성은 없었 다(
P
=0.075).따라서 신경계 증상이 있는 HLH환 자에서 진단의 지연이 높은 사망률과 예후에 영향을 미칠 가능성은 유추할 수 있으나 신경계 증상의 유 무만으로도 사망률에 영향이 있을 가능성 또한 높으 므로 이와 관련한 더 많은 수의 환자에서의 연구가 필요할 것으로 사료된다.이전 연구들에서 HLH의 뇌MRI 소견은 매우 다 양하여, T2강조영상에서 고신호 강도를 보이는 소 견과 함께 확산강조영상, (Diffusion weighted ima- 에서 제한을 보이는 병변이 백질 회색
ging, DWI) ,
질 회 백색질 결합 등 여러 부위에서 관찰되는 것, - 이 흔한 소견이지만 비 특이적인 뇌 위축 소견 또한 관찰되고 있음이 보고되어 있다9, 10). 본 연구에서도 뇌MRI 검사를 시행한 증례 중6 , 3증례에서 T2강 조영상에서 다발성 고신호강도를 보였고, 1증례에서 는 초기 뇌MRI상T2강조영상에서 국소적인 고신 호강도만을 보이다가 뇌부종으로 진행하였으며, 1명 에서 미만성의 뇌 위축, 1명에서는 정상 소견을 보 여 다양하고 비특이적인 뇌 MRI 소견을 보였다.
의 임상 양상은 중추신경계 임파종 랑게르
HLH ,
한스세포 조직구증 다발성 경화증, , ADEM 등과 같 은 광범위한 중추신경계 질환과 유사한 경우가 많다.
특히 말이집 탈락병(demyelinating disease)과 유 사한 경우가 많아 스테로이드 치료 후에 일시적으로 증상의 호전을 보이는 경우가 있으나 이후 잦은 증 상의 악화와 함께 비전형적 임상경과를 보이는 것이 특징이다. HLH의 임상경과 및 초기 증상이 비 특이
적인 신경계 증상을 보이고 뇌 MRI에서도 다양한 백질의 병변을 보이는 경우가 드물지 않아 실제 임 상에서는ADEM또는 감염 색전(septic emboli)등 과의 감별이 어려운 경우가 보고된 바 있고11, 12),저 자들 또한 증례 과 에서 질환 초기에는 임상증상1 4 과 영상소견 모두ADEM의 소견을 보여 스테로이드 등의 치료로 호전되었으나 일정 기간이 경과 한 후 신경학적 증상의 악화 및 재발과 함께 전신 증상이 동반되어HLH로 진단된 경우를 경험하였다.
의 질환의 초기에는 신경학적인 증상이 비특 HLH
이적이고 뇌, MRI 소견도 ADEM, 다발성 경화증 등의 말이집 탈락병 등과 (multiple sclerosis, MS)
감별이 어려운 경우가 드물지 않게 있으므로13)ADEM 등의 말이집 탈락병에서 병의 경과가 비 특이적이고 전신 증상의 동반과 함께 재발 할 경우 또는 신경계, 증상과 함께 전신 증상의 동반 및 발열의 기간이 길 어질 경우HLH의 가능성에 대한 고려가 필요할 것 으로 생각된다14-16).
증례 의 경우 갑자기 시작된 경련 및 의식저하를5 주소로 입원 치료 중 간질중첩증과 함께 심한 우측 뇌 부종 및 급성 뇌 이탈을 보여 두개 절제술 및 우 측 측두엽 절제술을 시행하였고 이후 뇌 조직검사, 상 HLH로 진단하였다. Weisfeld-Adams 등11)은 뇌MRI상ADEM과 같은 소견을 보이며HLH의 진 단기준에는 맞지 않지만 HLH가 의심되는 환자에서 뇌 조직검사 후HLH로 진단한 증례를 보고한 바 있 으며, Shinoda 등16)도 뇌MRI 상 악성교종이나 경 색을 의심하는 소견을 보였던 환자에서 전신 증상이 나 혈액 검사 등은 HLH의 진단기준에 맞지 않았으 나 뇌 조직검사 후 중추신경계에 국한된 HLH를 진 단한 증례를 보고하였다 본 연구에서 경험한 환자. 는 현재 항암 유지요법 중으로 재활치료를 받으면서 좌측 상지의 경미한 미세 운동장애만 남아 있을 정 도로 신경계 증상이 회복되어 외래 추적 관찰 중이 다. HLH의 경우 최근 들어 항암 치료성적이 매우 향상되었으므로7) 동반된 신경계 증상이 중증이고 의 진단기준에 완벽히 부합되지 않을 경우라도 HLH
어린이의 뇌 가소성 등을 고려할 때 임상적으로 의, 심이 될 경우엔 필요에 따라서 적극적이고 공격적인
진단 및 치료가 중요할 것으로 사료된다.
중추신경계를 침범한HLH의 경우 증상이 비특이 적이고 MRI 영상도 다른 질환과 감별이 어려운 경 우가 많아 발병부터 진단까지 기간이 길어지는 경향 이 있고 신경계 이상을 동반하지 않은 경우보다 사, 망률이 높다고 알려져 있다 그러나. HLH는 항암 화 학요법 조혈모세포 이식 등으로 치료할 경우 그 예, 후가 좋은 질환이므로 말이집 탈락병 또는 뇌염 등 과 유사한 비특이적 신경학적 증상 및 뇌MRI 보이 면서 경과 중 전신 증상과 함께 발열 등이 동반될 경 우, HLH의 진단 가능성을 고려하여 적극적인 진단 을 위한 검사를 하는 것이 필요할 것으로 사료된다.
요 약
목 적 : 신경계 증상으로 발현한HLH는 진단이 늦 어지고 적절한 시기에 치료를 시작하지 못하여 불량 한 예후를 나타낼 수 있다 본 연구에서는 신경계 증. 상으로 발병한HLH환자의 임상양상과 예후를 고찰 하였다.
방 법 :2002년 1월부터 2010년 12월까지 서울 대학교어린이병원 소아청소년과에서 HLH로 진단된 명의 환자 중 진단 당시 또는 병의 경과 중에 신 24
경계 증상이 있었던 명의 환자를 대상으로 임상 증7 상 및 진단 당시의 검사소견 첫 증상의 발병일 부터, 진단일 까지의 기간 뇌, MRI혹은 뇌CT소견 등의 임상양상을 고찰 분석하였다.
결 과 :24명의 환자 중 진단 시 신경계 증상이 있 었던 환자는 명으로 이 중 명은 첫 증상이 신경계7 4 증상이었다 신경계 증상으로는 경련이 명 우측 상. 6 , 하지 위약감을 나타낸 환자가 명이었다 신경계 증1 . 상이 동반되지 않았던 환자에서 발병일 부터 진단까 지의 기간은 최단 일에서 최장2 87일까지 이었으나, 신경계 증상이 동반된 경우 7일에서 385일로 매우 다양하였다 진단 시에 신경계 증상이 있었던 환자. 명중 명에서 뇌 를 시행하였고 명은 강
7 6 MRI , 3 T2
조영상에서 다발성 고신호강도를 보였고, 1명에서는 처음에는 T2 강조영상에서 국소적인 고신호강도를 보이다가 진단시에는 심한 뇌 부종을 보였고, 1명에
서 미만성의 뇌 위축, 1명에서는 정상 소견을 보였 다 신경계 증상을 보인. 7명의 환자 중 4명이 사망 하였고, 3명이 생존하였는데 이중 조혈모세포 이식 을 받은 환자가 1 ,명 치료종결 1년 후까지 재발 없 이 추적관찰 중인 환자가1 ,명 경미한 신경학적 후 유증을 가지고 치료 진행 중인 환자가 1명이다.
결 론 : 신경계 증상으로 발현한HLH는 비 특이적 인 신경계 증상과 영상소견으로 조기 진단 및 탈수 초성 질환 등 다른 질환과 감별이 어려운 경우가 드 물지 않다 그러나 항암 화학요법 조혈모세포 이식. , 등을 통한 치료로 좋은 예후를 보이므로 임상양상이 전형적이지 않거나 치료에 반응이 없는 신경계 질환 에서 전신 증상이 동반될 경우HLH가능성을 고려 하여 적극적인 진단을 위한 검사 및 치료가 필요할 것으로 사료된다.
References
1) Janka GE. Familial and acquired hemophagocytic lymphohistiocytosis. Eur J Pediatr 2007;166:95- 109.
2) Janka GE. Hemophagocytic syndromes. Blood Rev 2007;21:245-53.
3) Haddad E, Sulis ML, Jabado N, Blanche S, Fischer A, Tardieu M. Frequency and severity of central nervous system lesions in hemophagocytic lymp- hohistiocytosis. Blood 1997;89:794-800.
4) Henter Jl, Nennesmo I. Neuropathologic findings and neurologic symptoms in twenty-three children with hemophagocytic lymphohistiocytosis. J Pediatr 1997;130:358-65.
5) Chung TW. CNS Involvement in Hemophagocytic Lymphohistiocytosis: CT and MR Findings. Korean J Radiol 2007;8:78-81.
6) Horne A, Trottestam H, Aricò M, Egeler RM, Filipovich AH, Gadner H, et al. Frequency and spectrum of central nervous system involvement in 193 children with haemophagocytic lymphohi- stiocytosis. Br J Haematol 2008;140:327-35.
7) Henter JI, Horne AC, Aricó M, Egeler RM, Fili- povich AH, Imashuku S, et al. HLH 2004: diag- nostic and therapeutic guidelines for hemophago- cytic lymphohistiocytosis. Pediatr Blood Cancer 2007;48:124-31.
8) Yang S, Zhang L, Jia C, Ma H, Henter J-I, Shen K. Frequency and development of CNS involve- ment in Chinese children with hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer 2010;
54:408-15.
9) Goo HW, Weon YC. A spectrum of neuroradio- logical findings in children with haemophagocytic lymphohistiocytosis. Pediatr Radiol 2007;37:1110- 7.
10) Fitzgerald N, McClain K. Imaging characteristics of hemophagocytic lymphohistiocytosis. Pediatr Radiol 2003;33:392-401.
11) Turtzo LC, Lin DDM, Hartung H, Barker PB, Arceci R, Yohay K. A neurologic presentation of familial hemophagocytic lymphohistiocytosis which mimicked septic emboli to the brain. J Child Neurol 2007;22:863-8.
12) Weisfeld-Adams JD, Frank Y, Havalad V, Hoj- sak JM, Posada R, Kaicker SM, et al. Diagnostic challenges in a child with familial hemophagocytic lymphohistiocytosis type 3 (FHLH3) presenting with fulminant neurological disease. Childs Nerv Syst 2008;25:153-9.
13) Rostasy K, Kolb R, Pohl D, Mueller H, Fels C, Moers A, et al. CNS disease as the main mani- festation of hemophagocytic lymphohistiocytosis in two children. Neuropediatrics 2004;35:45-9.
14) Beaty A, Weller C, Levy B, Vogler C, Ferguson W, Bicknese A, et al. A teenage boy with late onset hemophagocytic lymphohistiocytosis with predominant neurologic disease and perforin deficiency." Pediatr Blood Cancer 2008;50:1070- 2.
15) Puliyel M, Rose W, Kumar S, Moses P, Gibikote S. Prolonged neurologic course of familial hemo- phagocytic lymphohistiocytosis. Pediatr Neuro- logy 2009;41:207-10.
16) Kieslich M, Vecchi M, Driever P, Laverda A, Schwabe D, Jacobi G. Acute encephalopathy as a primary manifestation of haemophagocytic lym- phohistiocytosis Developmental Medicine & Child Neurology 2001;43:555 8.–
17) Shinoda J, Murase S, Takenaka K, Sakai N. Iso- lated central nervous system hemophagocytic lymphohistiocytosis: case report. Neurosurgery 2005;56:E187-90.