1Flight Surgeon, Dental Clinic, Hospital of The 5th Tactical Airlift Wing, Pusan, South Korea
2Associate Professor, Division of Prosthodontics, Department of Dental Specialties, Mayo Medical School, Rochester, Minnesota, USA
3Associate Professor, Divison of Prosthodontics, Ajou Medical School, Suwon, South Korea
4Private Practice, Seoul, South Korea
초 초록록
임프란트-골 접촉면에 과도한 열이 전달되면 임프란트의 골유착을 방해할 수 있으므로 본 연구에서는 지르코니아/알루미 나 복합체 어버트먼트를 프레퍼레이션 할 때 임프란트 표면에 발생하는 열의 정도를 조사하였다. 60개의 지르코니아/알루미 나 복합체 어버트먼트를 5개씩 무작위로 12개의 실험군에 할당하고 어버트먼트를 임프란트와 연결해서 아크릴-레진 블록에 매몰한 뒤에 인체의 체온과 비슷한 37℃ 의 수조에 담가 두었다. 고속 핸드피스로 1분 동안 어버트먼트를 수평으로 1mm를 삭제하고 30초 동안에 저속 핸드피스로 연마하였다. 이때 냉각수를 공급하거나 하지 않으면서 임프란트 표면의 경부, 중간 부, 첨단부(apex)의 온도를 측정하였다. Mann-Whitney rank-sum test를 사용하여 냉각수를 사용한 경우와 하지 않은 경 우의 온도차의 통계학적 유의성을 검증하였다. 고속 핸드피스로 냉각수 없이 1mm를 수평으로 삭제하였을 때 임프란트 경부 에서 최고 41.22℃가 측정되었다. 냉각수 없이 고속 핸드피스로 삭제할 때 75%의 경우에서 40℃ 이상의 온도가 임프란트 경 부에서 측정되었다. 저속 핸드피스나 고속 핸드피스 공히 냉각수를 사용한 경우와 냉각수를 사용하지 않은 경우의 온도차는 임프란트 경부에서 통계학적으로 유의한 차이가 있었다(P=0.009). 반대로, 저속 핸드피스나 고속 핸드피스 공히 냉각수를 사용한 경우와 냉각수를 사용하지 않은 경우의 온도차는 임프란트 중간부와 첨단부에서는 통계학적으로 유의한 차이가 관찰 되지 않았다(P>0.05). 지르코니아/알루미나 복합체 어버트먼트의 프레퍼레이션은 임프란트 표면의 온도를 상승시켰지만 골 유착에 치명적이라고 알려진 47℃ 까지 이르지는 않았다.
Key words: implant abutment preparation, heat generation, zirconia/alumina complex abutment
Heat Transfer to the Implant-Bone Interface
during preparation of Zirconia / Alumina Complex Abutment
Jung-Bo Huh1, Steven E. Eckert2, Seok-Min Ko3, Yong-Geun Choi4
Heat Transfer to the Implant-Bone Interface
during preparation of Zirconia/Alumina Complex
Abutment
R
estorations in the anterior esthetic zone present challenges in both the surgical and prosthetic phases of implant dentistry.1-3Zirconia/alumina abutments may provide improved translucency for the implant supported restoration than is obtainable with metal abutments. Zirconia/alumina abutments would also be preferable to metal abutments because gray color of metal abutments may show through the peri-implant tissues.4 These factors have caused an increased interest in the use of ceramic advantages.5Osseointegration is one of the fundamental factors for the long term success of implant restorations. The successful achievement of osseointegration depends on meticulous sur- gical technique and careful prosthetic management.6Bone tissue injury from heat above 47℃ is harmful to osseointe-
ed. In contrast, few studies on heat during titanium or titanium-alloy abutments preparation in prosthetic phase have been reported.17-18Further, no study on heat during preparation of zirconia/alumina complex abutment is found in searches of the scientific literature.
The purpose of this study was to investigate the quantity of heat during abutment preparation of zirconia/alumina com- plex.
Experimental Design
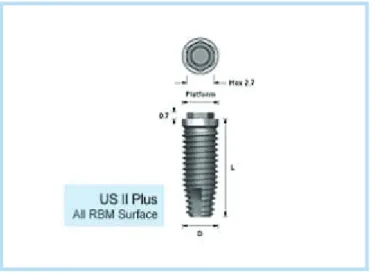
A US II plus implant 4mm in diameter and 13mm in length (Osstem, Seoul, South Korea) was embedded in an
Ⅱ
Fig. 1. US II Plus implant (Diameter:4.0mm, Length:13mm)
Jung-Bo Huh et al: Heat Transfer to the Implant-Bone Interface during preparation of Zirconia/Alumina Complex Abutment. Implantology 2008
Fig. 2. ZirAce Abutment(Platform: regular, Height: 5.5mm, collar:5.0mm)
Jung-Bo Huh et al: Heat Transfer to the Implant-Bone Interface during preparation of Zirconia/Alumina Complex Abutment. Implantology 2008
original article
Fig. 3. Schematic of locations of three temperature sensors
Jung-Bo Huh et al: Heat Transfer to the Implant-Bone Interface during preparation of Zirconia/Alumina Complex Abutment. Implantology 2008
ZirAce Abutment
US II Fixture Acrylic Resin Block
Thermocouple: Cervical Area
Thermocouple: Middle Area
Table 1. Temperatures at each location of implant during preparation of five abutments using each handpiece type accompanied with coolant and without coolant
E
Exxppeerriimmeenntt HHaannddppiieeccee CCoooollaanntt LLooccaattiioonn AAbbuuttmmeenntt AAbbuuttmmeenntt AAbbuuttmmeenntt AAbbuuttmmeenntt AAbbuuttmmeenntt G
Grroouupp ttyyppee 11 ((℃℃)) 22 ((℃℃)) 33 ((℃℃)) 44 ((℃℃)) 55 ((℃℃))
1 High Yes Cervical 38.58 37.50 38.90 37.80 38.58
2 High Yes Middle 37.80 37.50 37.02 36.69 37.21
3 High Yes Apical 37.50 37.39 37.02 36.33 37.21
4 High No Cervical 41.22 40.22 38.99 40.10 39.58
5 High No Middle 37.15 38.00 36.98 37.55 37.12
6 High No Apical 37.15 37.69 36.98 37.50 37.01
7 Low Yes Cervical 37.55 37.56 37.89 37.11 37.00
8 Low Yes Middle 37.01 37.00 36.98 37.45 37.69
9 Low Yes Apical 37.01 36.99 36.98 37.45 37.69
10 Low No Cervical 39.33 38.52 39.12 38.20 40.01
11 Low No Middle 37.08 37.96 37.45 37.45 37.23
12 Low No Apical 37.08 37.93 37.40 37.10 37.00
Jung-Bo Huh et al: Heat Transfer to the Implant-Bone Interface during preparation of Zirconia/Alumina Complex Abutment. Implantology 2008
acrylic resin block (Fig 1). The acrylic resin block was immersed in a water bath (Perform Inkovac system, Hedent GmbH, Oberursel, Germany) with a thermostatic tempera- ture-control mechanism maintaining the starting water tem- perature at 37℃. Sixty zirconia/alumina complex abutments (ZirAceⓇ, Osstem, Seoul, South Korea) were randomized to 12 experiment groups. Thus, each experiment group consist- ed of 5 abutments (Table 1). The abutment was connected to the implant through the use of a connecting screw and isolat- ed from the water bath by a rubber dam to prevent the water bath temperature influencing the temperature of the assem- bled components (Fig 2). A suction tip was held 2 mm from the abutment to remove the coolant collected in the rubber dam. Thermocouple electrodes were attached to cervical, middle, and apical parts of the implant (Fig 3). K-type (0.5mm diameter) temperature sensors were connected to a monitoring system PXI6259 (National Instrument, Texas, US) and LabView (National Instrument, Texas, US) (Fig 4).
Data was recorded at a rate of one location (cervical, middle, and apical) per 0.5 second in order.
Abutment Preparation
A high-speed turbine handpiece (Exceed EFⓇ, Yoshida Dental MFG., Tokyo, Japan) with rotation speed of 350,000 rpm and air pressure of 31.24psi was used to reduce the abut- ment. The air-coolant temperature was 26℃. Straight coarse (125㎛) diamond bur #6878(KometⓇ, Brasseler GmbH &
Co, Germany) was used to remove 1 mm of height over a time period of 1 minute from the most superior aspect of the abutment. A low-speed micromotor handpiece (Exceed EF
Ⓡ, Yoshida Dental MFG., Tokyo, Japan) with rotation speed of 40,000 rpm was used to polish the reduced abutment. Air- water spray with a temperature of 20℃ from a triple syringe was provided as coolant for the low-speed handpiece.
Silicone points (GreenieⓇ, Shofu Inc., Kyoto, Japan) were used to polish the abutment for 30 seconds. All preparations were performed by a single operator. Abutments, diamond burs and silicone points were replaced after each prepara- tion. Therefore, for high?speed handpiece, a total of 30 mea- surements of temperatures were conducted; 5 temperature measurements on the 5 abutments with coolant and 5 tem-
original article
perature measurements on the 5 abutment without coolant.
In addition, for low-speed handpiece, a total of 30 measure- ment of temperatures were conducted; 5 temperature mea- surements on the 5 abutments with coolant and 5 tempera- ture measurements on the 5 abutments without coolant. The measurements of maximum temperature during the prepara- tion of each abutment were made via thermosensors at the cervical, middle, and apical parts of the implants (Table 1).
Statistical Analysis
The Mann-Whitney rank-sum test was used to assess the statistical significance of difference of temperature at each location of implant between “with coolant”and “without coolant”when preparing the abutment with the two hand- piece types. P values less than .05 were considered signifi- cant. The statistical package used was JMP 5.0.1.2(SAS Institute, Cary, NC, USA).
Table 2. Mean temperature and statistical significance of temperature difference for Zirconia/Alumina Complex abutment with highspeed contouring
Location Coolant Mean temperature±SD Statistical significance (p-value)
Cervical Yes 38.27±0.59 0.009
No 40.02±0.83
Middle Yes 37.24±0.43 0.754
No 37.36±0.42
Apical Yes 37.09±0.46 0.834
No 37.27±0.31
Jung-Bo Huh et al: Heat Transfer to the Implant-Bone Interface during preparation of Zirconia/Alumina Complex Abutment. Implantology 2008
Table 3. Mean temperature and statistical significance of temperature difference for Zirconia/Alumina Complex abutment with lowspeed polishing
Location Coolant Mean temperature±SD Statistical significance (p-value)
Cervical Yes 37.42±0.36 0.009
No 39.04±0.71
Middle Yes 37.23±0.33 0.245
No 37.43±0.33
Apical Yes 37.22±0.33 0.465
No 37.30±0.38
Jung-Bo Huh et al: Heat Transfer to the Implant-Bone Interface during preparation of Zirconia/Alumina Complex Abutment. Implantology 2008
As shown on table 1, temperatures in excess of 40℃ were observed at the cervical part of implant for highspeed reduc- tion and lowspeed polishing without coolant. The maximum temperature of 41.22℃ was observed at the cervical part of implant of abutment 1 for highspeed reduction without coolant. Among the five cervical part of implant of abut- ments for highspeed reduction without coolant, temperatures more than 40℃ were observed at the three cervical part of implant of abutments. Table 2 shows that temperature differ- ence between “with coolant”and “without coolant”during highspeed reduction. These results were statistically signifi- cant at the cervical part of implant (P=0.009). In contrast, temperature difference between “with coolant”and “without coolant”during highspeed reduction was not statistically significant at the middle and apical parts of implant (P>0.05). Table 3 also shows that temperature difference between “with coolant”and “without coolant”during lowspeed polishing was statistically significant at the cervi- cal part of implant (P=0.009). In contrast, temperature differ- ence between “with coolant”and “without coolant”during lowspeed polishing was not statistically significant at the middle and apical parts ex of implant (P>0.05).
Gross et al.17reported that maximum temperature after reducing 1 mm of height from the most superior aspect of
um abutment for 10 seconds with lowspeed handpiece with coolant was 39℃.18In contrast, the preparation of titanium abutment for 30 seconds with lowspeed handpiece without coolant provoked maximum temperature of 155℃, a tem- perature that is much higher than 47℃ described as critical for irreversible bone damage.10Therefore, regardless of the handpiece type, preparation of titanium abutment and titani- um-alloy abutment without coolant could cause irreversible damage to bone and osseointegration.
In contrast, the current study demonstrated a maximum temperature 41.22℃ that is lower than critical level 47℃.
This temperature was observed during the preparation of zir- conia/alumina complex abutment with highspeed handpiece without coolant for 1 minute. Lower temperature increase of zirconia/alumina complex than that of titanium or titanium- alloy abutments may provide a higher comfort with this preparation.
The current study was performed in such a way as to reduce variability and bias. To decrease inter-operator vari- ability, all preparations were performed by a single operator.
To decrease intra-operator variability, the operator was trained to prepare the abutments in accordance with the oper- ations manual to help the performance to be uniform over the 60 abutments.19To reduce inter-abutment variability, five abutments were used for each experiment group and the mean of the five measurements was analyzed to assess the statistical significance. By automating the measuring instru- ments with PXI6259 (National Instrument, Texas, US) and
Ⅳ
original article
LabView (National Instrument, Texas, US), variations in the way human observers make measurements could be elimi- nated. Selection bias in allocating abutments to experiment groups was reduced by the randomization of abutments.
Therefore, random allocation of abutments made experimen- tal groups similar at the start of the experiment.20
The amount and duration of abutment preparation in this study was determined to be in keeping with previously described methods.17,18Although preparation of the axial walls of the abutment may provide a better simulation of the clinical situation, this approach may not lend itself to stan- dardization as well as the employed method thereby result- ing in increased variability of results. Given the results of the current study it appears that the risks to the bone to implant interface through thermal insult are minimal when zirconi- um/alumina complex abutments are prepared intraorally.
Preparation of zirconia/alumina complex abutment result- ed in an increase in temperature within the implant body but this rise in temperature did not exceed the critical level of 47
℃ described in implant literature regardless of locations, coolant usage and handpiece types.
Acknowledgments
The authors acknowledge support provided by Osstem.
1. Sadoun M, Perelmuter S. Alumina-zirconia machinable abutments for implant-supported single-tooth anterior crowns. Pract Periodontics Aesthet Dent. 1997;9(9):1047-53.
2. Yildirim M, Edelhoff D, Hanisch O, Spiekermann H. Ceramic abut- ments--a new era in achieving optimal esthetics in implant dentistry. Int J Periodontics Restorative Dent. 2000;20(1):81-91.
3. Brodbeck U. The ZiReal Post: A new ceramic implant abutment. J Esthet Restor Dent. 2003;15(1):10-23.
4. Yildirim M, Fischer H, Marx R, Edelhoff D. In vivo fracture resistance of implant-supported all-ceramic restorations. J Prosthet Dent.
2003;90(4):325-31.
5. Stanford CM, Oates T, Beirne R. Zirconia as an Implant and Restorative Biomaterial. Int J Oral Maxillofac Implants. 2006;21(6):841-4.
6. Worthington P, Lang BR, Rubenstein JE. Osseointegration in Dentistry:
An Overview, ed 2. Chicago: Quintessence Publishing Co. Inc., 2003:1-5.
7. Glyn OP. Bone Biology and Healing, ed 1. Singapore: World Scientific Publishing Co. Pte. Ltd., 2003:31-45.
8. Currey JD. Bones: Structure and Mechanics, ed 1. New Jersey:
Princeton University Press, 2003:3-26.
9. Eriksson AR, Albrecktsson T, Grane B, McQueen D. Thermal injury to bone. A vital-microscopic description of heat effects. Int J Oral Surg.1982;11:115-21.
10. Eriksson AR, Albrektsson T. Temperature threshold levels for heat- induced bone tissue injury: A vital-microscopic study in the rabbit. J Prosthet Dent. 1983;50:101-107.
11. Misch CE. Contemporary Implant Dentistry, ed 2. Missouri: Mosby, 1999;242-5.
12. Eriksson AR, Albrecktsson T. Temperature threshold levels for heat- induced bone tissue injury: A vital-microscopic study in the rabbit. J
Ⅴ
14. Eriksson AR, Adell R. Temperatures during drilling for the placement of implants using the osseointegration technique. Journal of Oral &
Maxillofacial Surgery.1986;44: 4-7.
15. Watanabe F, Tawada Y, Komatsu SH, Hata Y. Heat distribution in bone during preparation of implant sites; Heat analysis by real-time thermog- raphy. Int J Oral Maxillofac Implants.1992;7:212-9.
16. Haider R, Watzek G, Plenk H. Effects of drill cooling and bone structure on IMZ implant fixation. Int J Oral Maxillofac Implants.1993;8:83-91.
titanium implants of the ITI Dental Implant System: an in vitro study.
Clin Oral Implants Res. 1995;6(4):254-9.
19. Hulley SB, Cummings SR, Browner WS, Grady D, Hearst H, Newman TB. Designing clinical research, ed 2. Philadelphia: Lippincott Williams
& Wilkins, 2001:37-50.
20. Rothman KJ. Epidemiology, ed 1. New York: Oxford University Express, 2002:94-112.
Corresponding author: 최용근
Private Practice: Jang-an dong 311-4 Seoul, South Korea
Tel: 3394-7555 Fax: 3394-6875
Email: [email protected] Received 4 August 2008 Accepted 5 November 2008