서 론
2007–2008
년 미국 국립건강영양조사(US National Health and Nutrition Examination Survey
) 연구에 따르면 미국인 남녀 고요산혈 증의 유병률이21
%를 넘었으며 이는1988–1994
년 조사 자료18
.2
% 에 비해 상승하여1) 공중 보건 문제로 대두되고 있다. 또한 중국에서 도 생활 습관의 급격한 변화로 고요산혈증 유병률이 급증하여 중국 북부와 동북부 지방에서는 유병률이13
.7
%에 이르렀다(남자21
%, 여자7
.9
%).2) 국내의 경우2016
년 국민건강영양조사(Korea National
Health and Nutrition Examination Survey
)를 토대로 고요산혈증 유병 률을 평가한Kim
등3)의 연구 결과에 따르면19
세 이상 한국 성인의 고요산혈증 유병률은11
.4
%였으며 남성에서17
.0
%, 여성에서5
.9
% 였다.요산은 퓨린 대사과정의 최종 산물로서 간에서 만들어져 주로 신 장으로 배출되며 일부 장으로 배출된다.4) 또한 세포 외 환경에서 항 산화 작용을 할 수 있으며5) 세포 내 환경에서는 반대 작용을 하고 산화 스트레스와 염증 반응을 촉진한다.6)
혈중 요산 농도는 여성 호르몬, 연령, 체질량지수(
body mass
Received October 1, 2019 Accepted November 4, 2019Corresponding author Yeon Ji Lee Tel: +82-32-890-3547, Fax: +82-32-890-2195 E-mail: [email protected]
ORCID: http://orcid.org/0000-0001-7712-996X
Copyright © 2019 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Original Article
https://doi.org/10.21215/kjfp.2019.9.6.532 eISSN 2233-9116
Korean J Fam Pract. 2019;9(6):532-538
Korean Journal of Family Practice
KJFP
한국 성인의 고요산혈증과 건강 관련 삶의 질과의 연관성: 제7기 국민건강영양조사 자료 이용(2016–2017년)
방지혜, 이연지*, 최지호, 김유현, 안성희, 이민경, 이상숙
인하대학교 의과대학 가정의학교실
Association between Hyperuricemia and Health-Related Quality of Life in Korean Adults: Based on the Seventh Korean National Health and Nutrition Examination Survey (2016–2017)
Zee Hae Bang, Yeon Ji Lee*, Ji-Ho Choi, Yoohyun Kim, Sung Hee An, Min Kyoung Lee, Sangsook Lee Department of Family Medicine, Inha University College of Medicine, Incheon, Korea
Background: The prevalence of hyperuricemia has increased over the past few decades. Hyperuricemia is responsible for the increased risk of hypertension, type 2 diabetes mellitus, chronic renal disease, and cardiovascular disease. Health-related quality of life (HQoL) has been increasingly used as an outcome in clinical trials, effectiveness research, and research on quality of care. Therefore, we aimed to analyze the association between hyperuricemia and HQoL in Korean adults aged >19 years.
Methods: We included 2,376 male and 2,593 female who participated in the Korea National Health and Nutrition Examination Survey from 2016 to 2017. Hyperuricemia was defined as a serum uric acid (SUA) level of 7 mg/dL. The Euro quality of life-5 dimension (EQ-5D) questionnaire was used to measure HQoL. A multiple logistic regression analysis was performed to examine the association between hyperuricemia and HQoL.
Results: The EQ-5D index score of the hyperuricemia group was significantly lower than of the healthy group. After adjusting for multiple covariates, the odds ratio (95% confidence interval, [CI]) for mobility issues was 1.46 (95% CI, 1.211–1.683) in male and 1.33 (95% CI, 0.716–2.464) in female;
however, the difference was not statistically significant for female.
Conclusion: Hyperuricemia was associated with reduced quality of life. It is important to control SUA levels to improve HQoL.
Keywords: Serum Uric Acid; Hyperuricemia; Health-Related Quality of Life; Adults
방지혜 외. 고요산혈증과 건강 관련 삶의 질 Korean Journal of Family Practice
KJFP
index
,BMI
), 혈압, 탈수, 음주 습관 등 다양한 인자들에 의하여 영 향을 받는데7,8) 정상적인 목표치는 고요산혈증 및 통풍 조절을 위한 개정된 가이드 라인에 따르면7 mg
/dL
이나9) 임상적으로 의미 있는 혈중 요산 농도는 명확하지 않으며 최근 역학 및 치료 자료에 근거 하여 새로운 고려가 필요하다.한편 인슐린은 신장에서의 요산 배설을 감소시키기 때문에 대사 증후군에서 관찰되는 요산 농도 상승이 고인슐린혈증에 기인하나 때때로 고요산혈증은 고인슐린혈증보다 선행하기도 한다.10) 고요산 혈증은 통풍의 위험 요인일 뿐만 아니라 심혈관계 질환 사망률의 위 험과 독립적으로 유의미하게 관련되어 있음을
Fang
과Alderman
8)이 보고하였고acute myocardial infarction
와 독립적인 위험 관계가 있다 는 것이Krishnan
등11)의 연구에서 밝혀졌다.또한 혈중 요산 농도는 고혈압,12) 관상동맥 질환,13) 혈관성 치매,13) 자간전증,14) 신장 질환 등을 포함하는 다양한 심혈관 질환과 관련되 어 있음15)이 보고되었고
2
세대에 걸쳐 전향적으로 조사된Fra
mingham Heart Study
에서는 다른 알려진 위험 요소와 독립적으로 혈중 요산 농도가 높을수록 제2
형 당뇨병 발생 위험이 증가함을 보 였다.16) 혈중 요산 농도가 대사 증후군의 정의에 속하지는 않지만 여 러 연구에서 혈중 요산 농도가 대사 증후군 또는 그것의 구성 요소 와 많은 연관성이 있음을 보여준다.이처럼 혈중 요산 농도는 심혈관 질환, 대사 증후군, 신장 질환, 통풍과 같은 만성 질환과 밀접한 관련이 있는 중요한 건강 지표로 증명되고 있다.
건강 관련 삶의 질(
health-related quality of life
,HQoL
)은 지난20
년 간 만성 질환을 앓고 있는 환자의 치료 결과를 측정하는 중요한 지 표로 사용되었으며17) 보건 서비스 이용 및 사망률을 예측하는 것으 로 밝혀졌다.18)EuroQoL 5 dimension
(EQ-5D
)19)는 건강 관련 삶의 질 을 측정하는 도구 중의 하나이며 일반 인구 및 환자 그룹에서 광범 위하게 유효성이 확인되었고 감수성이 예민하며 일관성 있고 신뢰 할 수 있는QoL
도구이다.20)건강 관련 삶의 질이 만성 질환 환자에서 중요한 치료 성과 지표 로 여겨지므로 만성 질환과 혈중 요산 농도 간의 연관성을 고려하면 혈중 요산 농도가 건강 관련 삶의 질과 연관이 있을 것으로 예상된 다. 본 연구에서는 우리나라 성인 인구를 대상으로 고요산혈증과 건강 관련 삶의 질의 관계를 파악하고자 한다.
방 법
1. 연구대상
본 연구는 제
7
기1
,2
차년도 국민건강영양조사(2016–2017
년)에 참여한 대한민국 남녀
8
,127
명 중에서EQ-5D
설문 항목 무응답자, 혈 중 요산농도 결측값이 있는 경우를 제외한 만19
세 이상의 대한민국 성인 남녀를 대상으로 하였다. 남성2
,376
명, 여성2
,593
명, 총4
,969
명을 분석 대상으로 하였다.2. 국민건강영양조사 자료 활용 방법 1) 고요산혈증의 정의
현재 고요산혈증을 정의하는 여러 기준이 제시되고 있으나 일반 적으로 임상 실험실에서 사용되고 있는 혈중 요산 농도
7 mg
/dL
이 상으로 정의하였다.21)2) 건강 관련 삶의 질 자료 이용
건강 관련 삶의 질(
HQoL
)은 당뇨병, 심혈관 질환, 신장 질환 및 악성 종양을 비롯한 다양한 질병 환자에게 국제적으로 사용되는 환 자 중심의 임상 결과이다.22,23) 건강 관련 삶의 질을 평가하는 도구로EuroQoL group
에서 개발한 선호도 기반의HQoL
측정 도구인EQ- 5D
,19)EQ-5D index
를 사용하였다.EQ-5D
는 ‘운동능력’, ‘자기관리’, ‘일상활동,’ ‘통증/불편’, ‘불안/우울’로 각
5
개 차원으로 이루어져 있으며 이에 대하여 현재의 상태 를 ‘문제없음’, ‘다소 문제 있음’, ‘심각한 문제 있음’의3
가지 단계로 평가한다.24)EQ-5D index
는 완전한 건강 상태인1
부터 가장 낮은 점수인-0
.171
까지의 가중 지표값으로 계산한다.25)본 연구에서는
EQ-5D 5
개 영역의3
가지 응답 항목을 문제 없음과 문제 있음(다소 문제 있음, 심각한 문제 있음)으로 구분하였고EQ- 5D index
의 평균과 표준편차를 구하였다.3) 만성질환의 정의
만성질환은 고혈압, 당뇨, 이상지질혈증, 암, 우울증, 간경화, 만성 신부전, 뇌졸중, 심혈관계 질환, 관절염, 만성폐쇄성폐질환, 천식, 아 토피 피부염으로 국한하였고 심혈관계 질환은 심근경색과 협심증 으로 정의하였으며 관절염은 골관절염 또는 류마티스 관절염으로 정의하였다. 질환의 유무는 의사 진단 여부를 기준으로 하였다.
4) 기타 변수의 정의
제
7
기1
,2
차년도 국민건강영양조사(2016–2017
년) 원시 자료 중 건 강면접조사와 보건의식행태 조사자료에 포함된 나이, 체질량지수, 삶의 질, 교육수준, 알코올, 흡연, 규칙적 운동을 이용하였다. 나이 는19–39
세,40–59
세,60
세 이상으로 분류하였고 체질량지수는 체 중(kg
)을 신장의 제곱(m
2)으로 나눈 값으로 계산하였다. 교육수준Original Article
Korean Journal of Family Practice
Zee Hae Bang, et al. Hyperuricemia and Health-Related Quality of Life
Korean Journal of Family Practice
KJFP
은 교육수준 재분류 코드에 따라 초등학교 졸업 이하, 중학교 졸업, 고등학교 졸업, 대학교 졸업 이상으로 구분하였다. 음주는 한 달에
1
회 이상 술을 마시는 경우로, 비음주는 한 달에1
회 미만으로 마시 는 경우로 정의하였다. 흡연은 피운 적 없거나100
개비 미만으로 흡연한 경우를 비흡연군,
100
개비 이상 흡연한 경우를 흡연군으로 분 류하였다. 규칙적 운동은International Physical Activity Question
naire
26)를 참고하여, 고강도 신체 활동을1
회20
분 이상, 주3
회 이상 실천하거나, 중강도 신체활동을1
회30
분 이상, 주5
회 이상 실천한Table 1. Baseline characteristics of study population according to sex from KNHANES 2016–2017
Characteristic Male (n=2,376) Female (n=2,593) P-value
Mean age (y) 50.490±16.541 48.940±15.886 <0.001
Age categories (y) 0.004
19–39 685 (28.8) 792 (30.5)
40–59 925 (38.9) 1,076 (41.5)
≥60 766 (32.2) 725 (28.0)
Uric acid (mg/dL) 5.960±1.358 4.440±1.010 <0.001
Body mass index (kg/m2) 24.420±3.315 23.370±3.714 <0.001
EQ-5D
EQ-5D index 1.080±0.178 1.110±0.198 <0.001
Problem of
Mobility 222 (9.3) 316 (12.2) 0.001
Self care 60 (2.5) 65 (2.5) 0.519
Usual activity 120 (5.1) 157 (6.1) 0.069
Pain/discomfort 411 (17.3) 659 (25.4) <0.001
Anxiety/depression 145 (6.1) 233 (9.0) <0.001
Education status <0.001
Elementary school or low 311 (13.1) 527 (20.3)
Middle school 249 (10.5) 234 (9.0)
High school 797 (33.5) 794 (30.6)
University or more 1,019 (42.9) 1,038 (40.0)
Chronic illness
Hypertension 617 (26.0) 469 (18.1) <0.001
DM 239 (10.1) 171 (6.6) <0.001
Dyslipidemia 392 (16.5) 476 (18.4) 0.046
Cancer 98 (4.1) 147 (5.7) 0.007
Depression 62 (2.6) 121 (4.7) <0.001
Liver cirrhosis 12 (0.5) 7 (0.3) 0.133
Chronic renal failure 8 (0.3) 4 (0.2) 0.154
Stroke 68 (2.9) 36 (1.4) <0.001
Coronary artery disease 87 (3.7) 43 (1.7) <0.001
Arthritis 134 (5.6) 421 (16.2) <0.001
COPD 15 (0.9) 8 (0.3) 0.083
Asthma 71 (3.0) 69 (2.7) 0.271
Atopic dermatitis 64 (2.7) 73 (2.8) 0.431
Health-related lifestyle
Alcohol <0.001
Never and rare (<once a month) 587 (24.7) 1,287 (49.6)
≥Once a month 1,789 (75.3) 1,306 (50.4)
Smokinga <0.001
Never smoker 617 (26.0) 2,326 (89.7)
Smoker 1,759 (74.0) 267 (10.3)
Regular exercise <0.001
Regular 916 (38.6) 730 (28.2)
Irregular 1,460 (61.4) 1,863 (71.8)
Values are presented as mean±standard error or number (%).
KNHANES, Korea National Health and Nutrition Examination Survey; EQ-5D, Euro quality of life-5 dimension; DM, diabetes mellitus; COPD, chronic obstructive pulmo- nary disease.
aNever smoker, <100 cigarettes in life; smoker, ≥100 cigarettes in life.
방지혜 외. 고요산혈증과 건강 관련 삶의 질 Korean Journal of Family Practice
KJFP
경우에 규칙적 운동을 한 것으로 정의하였다. 고강도 신체활동은 격렬한 신체 활동으로 숨이 많이 차거나 심장이 매우 빠르게 뛰는 활동(
20 kg
이상을 들어 올리거나 나르는 일, 땅파기, 건설 현장에서 의 노동, 계단으로 물건 나르기 등)이며 중강도 활동은 중간 정도의 신체 활동으로 숨이 약간 차거나 심장이 약간 빠르게 뛰는 활동(일 하는 중에 빠르게 걷기, 가벼운 물건 나르기, 청소, 아이 목욕 시키 거나 안아 주는 등의 육아)을 말한다.3. 통계분석
통계분석은 제
7
기1
,2
차년도 국민건강영양조사(2016–2017
년) 자 료를 이용하여 만19
세 이상 성인을 대상으로 통계 분석을 시행하 였다. 연구 대상자들의 기본 특성은 성별에 따라 연속 변수는 평균 과 표준편차로 제시하였고 범주 변수는 빈도(%)로 제시하였으며 각 각 독립표본t-
검정과 카이제곱 검정을 이용하였다. 연령별로 그룹 을 나눈 후 고요산혈증의 유병률은 카이제곱 검정을 이용하여 분석 하였고 고요산혈증이 있는 그룹에서 연령별EQ-5D
와의 연관성을 알아보기 위해 로지스틱 회귀분석을 시행하였다. 통계적 유의 수준 은P-value<0
.05
로 하였고 통계 분석은IBM SPSS Statistics for Windows
,Version 21
.0
(IBM Co
.,Armonk
,NY
,USA
)을 이용하였다.결 과
1. 연구 대상자의 일반적인 특성
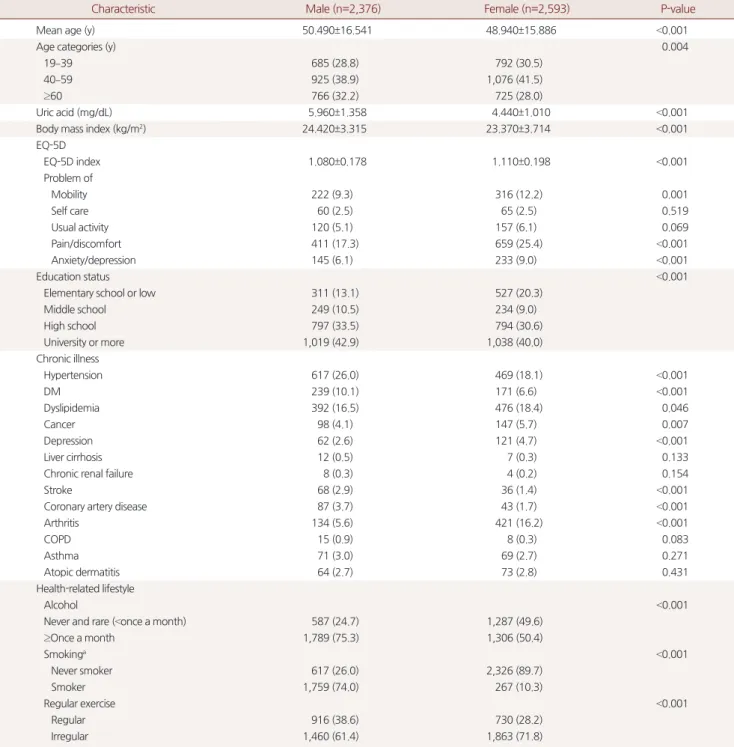
Table 1
에서 연구 대상자들의 일반적 특성을 성별로 나누어 표기 하였다. 남성2
,376
명, 여성2
,593
명으로,19–39
세는1
,477
명,40–59
세 는2
,001
명,60
세 이상은1
,491
명이었다. 남성의 경우 평균 연령은50
.490
±16
.541
세, 혈중 요산 농도는5
.960
±1
.358 mg
/dL
,EQ-5D
에서 통증/불편 문제 호소 비율이17
.3
%로 가장 높았고, 그 다음으로 운 동 능력의 문제 호소 비율이9
.3
%로 나타났다. 여성의 경우 평균 연 령은48
.940
±15
.886
세, 혈중 요산 농도는4
.440
±1
.010 mg
/dL
이며EQ-5D
중 통증/불편 문제 호소 비율이25
.4
%로 가장 높고, 그 다음 으로 운동 능력의 문제가12
.2
%로 나타났다.2. 연령 그룹별 평균 혈중 요산 농도와 고요산혈증 유병률
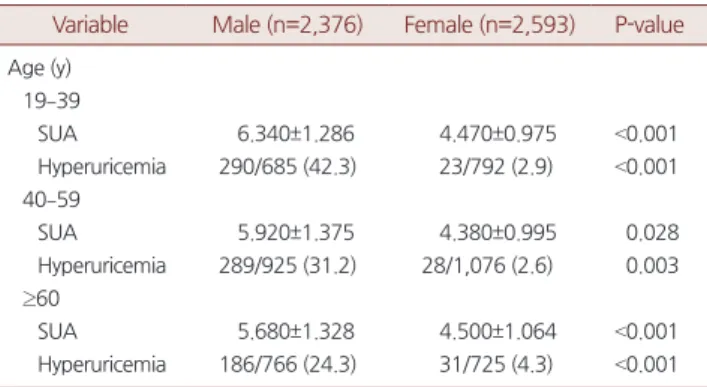
Table 2
는 남녀 각각에서 연령 그룹별serum uric acid
(SUA
)level
평균값과 표준편차, 고요산혈증 유병률을 나타낸 결과로 남성에서 는 연령이 증가함에 따라SUA
평균값이 유의하게 감소하였고 고요 산혈증 유병률도 유의하게 감소하였다. 여성에서는 연령 증가에 따 른SUA
평균값, 고요산혈증 유병률 간에 유의성이 없었다(P<0
.05
).3. 연령 증가에 따른 고요산혈증과 건강 관련 삶의 질 지표와의 연관성
Table 3
은 남녀 각각의 정상 그룹과 고요산혈증 그룹에서의 연령 별EQ-5D index
의t-test
결과로 평균과 표준편차를 나타냈다. 남녀 정상 그룹과 고요산혈증 그룹에서 연령이 높아질수록EQ-5D index
가 감소하였고 통계적으로도 유의하였다. 남성과 여성 모두 고요산Table 2. Mean SUA level and prevalence of hyperuricemia according to age and sex
Variable Male (n=2,376) Female (n=2,593) P-value Age (y)
19–39
SUA 6.340±1.286 4.470±0.975 <0.001
Hyperuricemia 290/685 (42.3) 23/792 (2.9) <0.001 40–59
SUA 5.920±1.375 4.380±0.995 0.028
Hyperuricemia 289/925 (31.2) 28/1,076 (2.6) 0.003 ≥60
SUA 5.680±1.328 4.500±1.064 <0.001
Hyperuricemia 186/766 (24.3) 31/725 (4.3) <0.001 Values are presented as mean±standard error or number (case/total, %).
SUA, serum uric acid.
Hyperuricemia, SUA ≥7 mg/dL.
P-values represent prevalence of hyperuricemia according to age group by analy- sis of variance for continuous variable and chi-square test (P<0.05).
Table 3. EQ-5D index according to hyperuricemic status and age group Age
Male EQ-5D index
Female EQ-5D index
Normal (y) Hyperuricemia (y) P-value Normal (y) Hyperuricemia (y) P-value
Total 1.070±0.227a 1.040±0.185a 0.010 1.110±0.242a 1.070±0.262a 0.003
19–39 1.130±0.224a 1.110±0.213a 0.019 1.220±0.269a 1.210±0.289a 0.006
40–59 1.060±0.169a 1.050±0.154a 0.015 1.070±0.150a 1.050±0.158a 0.005
≥60 1.030±0.105a 1.020±0.114a 0.015 1.050±0.122a 1.030±0.129a 0.008
Values are presented as mean±standard error.
EQ-5D, Euro quality of life-5 dimension.
aP-values represent differences between age group in each gender (P<0.05).
P-value were obtained by analysis of variance.
Zee Hae Bang, et al. Hyperuricemia and Health-Related Quality of Life
Korean Journal of Family Practice
KJFP
혈증 그룹이 정상그룹에 비해 건강 관련 삶의 질 지표가 낮았고 연 령이 증가함에 따라 건강 관련 삶의 질 만족도가 낮게 나타났다 (
P<0
.05
).4. 고요산혈증과 EQ-5D와의 관계
Table 4
는 성별에 따른 고요산혈증과EQ-5D
의 연관성에 관한 로 지스틱 회귀분석 결과이다. 남성은model 1
의 경우 고요산혈증이 있 는 사람이 정상인과 비교했을 때 ‘통증/불편’의 문제 발생 위험이1
.71
배 증가하였고(95
%confidence interval [CI]
,1
.449–2
.041
)model 2
의 경우 ‘통증/불편’의 문제 발생 위험도가1
.66
배(95
%CI
,1
.264–
2
.165
),model 3
에서는 ‘운동 능력’의 문제 발생 위험이1
.46
배 증가하 였다(95
%CI
,1
.211–1
.683
). 여성에서는model 1
의 경우 고요산혈증 그룹에서 정상 그룹에 비해 ‘불안/우울’ 문제 발생 위험이2
.29
배 증 가하였다(95
%CI
,1
.167–4
.474
).5. 연령 그룹별 고요산혈증과 EQ-5D와의 연관성
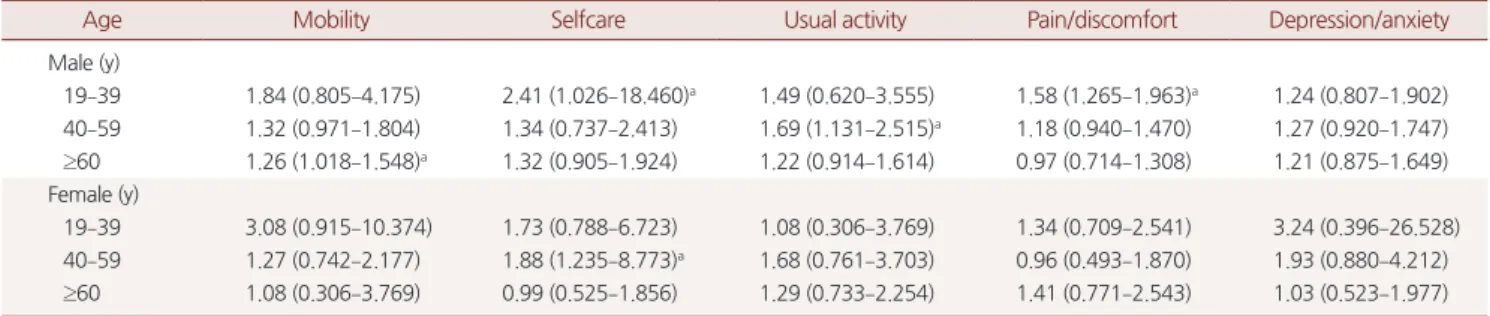
Table 5
는 연령 그룹별로 고요산혈증에 따른EQ-5D
와의 연관성 을 보기 위해 로지스틱 회귀분석을 시행한 결과이다. 남성에서는20–30
대 그룹에서 고요산혈증일 때 ‘자기관리’의 문제 발생 위험도가
odds ratio [OR]
,2
.41
(95
%CI
,1
.026–18
.460
)로 유의하게 높았고60
대 이상에서 고요산혈증일 때 ‘운동능력’의 문제 발생 위험도가OR
,1
.26
(95
%CI
,1
.018–1
.548
)으로 유의하게 높았다. 여성에서는40–50
대 그룹에서 ‘자기관리’ 문제 발생 위험도가OR
,1
.88
(95
%CI
,1
.235–8
.773
)로 유의하게 높았다.고 찰
기존 연구3)에 따르면 고요산혈증은 남녀 유병률이 다르고 연령에 따라
U-shape
연관성이 관찰되어 본 연구에서는 성별과 연령 그룹별 로 나누어 만19
세 이상 성인에서 혈중 요산 농도와 건강 관련 삶의 질과의 관계를 분석하였다.Table 5. Adjusted odds ratio for individual components of EQ-5D descriptive system in subjects with hyperuricemia according to age group
Age Mobility Selfcare Usual activity Pain/discomfort Depression/anxiety
Male (y)
19–39 1.84 (0.805–4.175) 2.41 (1.026–18.460)a 1.49 (0.620–3.555) 1.58 (1.265–1.963)a 1.24 (0.807–1.902) 40–59 1.32 (0.971–1.804) 1.34 (0.737–2.413) 1.69 (1.131–2.515)a 1.18 (0.940–1.470) 1.27 (0.920–1.747) ≥60 1.26 (1.018–1.548)a 1.32 (0.905–1.924) 1.22 (0.914–1.614) 0.97 (0.714–1.308) 1.21 (0.875–1.649) Female (y)
19–39 3.08 (0.915–10.374) 1.73 (0.788–6.723) 1.08 (0.306–3.769) 1.34 (0.709–2.541) 3.24 (0.396–26.528) 40–59 1.27 (0.742–2.177) 1.88 (1.235–8.773)a 1.68 (0.761–3.703) 0.96 (0.493–1.870) 1.93 (0.880–4.212) ≥60 1.08 (0.306–3.769) 0.99 (0.525–1.856) 1.29 (0.733–2.254) 1.41 (0.771–2.543) 1.03 (0.523–1.977) Values are presented as odds ratio (95% confidence interval).
EQ-5D, Euro quality of life-5 dimension.
Odds ratios and 95% confidence intervals were obtained by logistic regression analysis. Adjusted by age, body mass index, hypertension, diabetes mellitus, dyslipidemia, cancer, depression, liver cirrhosis, chronic renal failure, stroke, coronary artery disease, arthritis, asthma, atopic dermatitis, smoking, alcohol, regular exercise, education.
aP-value<0.05.
Table 4. Adjusted odds ratio for individual components of EQ-5D descriptive system in subjects with hyperuricemia
Variable Mobility Selfcare Usual activity Pain/discomfort Depression/anxiety
Male
Model 1 1.54 (1.090–2.168)a 1.32 (0.686–2.530) 0.67 (0.529–1.025) 1.71 (1.449–2.041)a 1.18 (0.790–1.735) Model 2 1.48 (1.236–1.908)a 1.29 (0.715–2.313) 1.47 (1.527–3.976)a 1.66 (1.264–2.165)a 0.85 (0.591–1.203) Model 3 1.46 (1.211–1.683)a 0.83 (0.450–1.506) 0.79 (0.523–1.171) 0.97 (0.778–1.208) 1.11 (0.797–1.543) Female
Model 1 1.41 (0.704–2.797) 0.98 (0.379–2.494) 1.23 (0.567–2.670) 1.28 (0.798–2.053) 2.29 (1.167–4.474)a Model 2 1.39 (0.747–2.594) 1.11 (0.510–2.380) 1.11 (0.575–2.106) 1.16 (0.727–1.837) 1.06 (0.483–2.291) Model 3 1.33 (0.716–2.464) 1.24 (0.567–2.684) 1.37 (0.711–2.640) 0.84 (0.490–1.440) 0.59 (0.308–1.118) Values are presented as odds ratio (95% confidence interval) by using logistic regression analysis.
Model 1 was adjusted for age, body mass index. Model 2 was adjusted for hypertension, diabetes mellitus, dyslipidemia, cancer, depression, liver cirrhosis, chronic renal failure, stroke, coronary artery disease, arthritis, asthma, atopic dermatitis in addition to the factors of model 1. Model 3 was adjusted for smoking, alcohol, regular exer- cise, education in addition to the factors of model 2.
EQ-5D, Euro quality of life-5 dimension.
aP-value<0.05.
방지혜 외. 고요산혈증과 건강 관련 삶의 질 Korean Journal of Family Practice
KJFP
남녀를 연령별로 구분하여
SUA
를 비교하였을 때 남성에서는 연 령이 증가함에 따라SUA
평균값이 유의하게 감소하고 고요산혈증 유병률도 유의하게 감소하였으나 여성에서는 연령 증가에 따라SUA
평균값과 고요산혈증 유병률이 감소하는 경향을 보이다가 여성 호 르몬의 영향이 감소하는60
대 이후에는 다시SUA
평균값과 유병률 이 증가하였다.정상 그룹과 고요산혈증이 있는 그룹에서 연령별로 비교 시 고요 산혈증이 있을 경우 남녀 모두 정상 그룹에 비해 모든 연령 그룹에 서
EQ-5D index
가 유의하게 낮게 나타났으며 나이가 증가할수록EQ-5D index
가 감소하는 추세를 보여 고요산혈증이 만19
세 이상 성인에서 건강관련 삶의 질에 영향을 주는 것으로 나타났다.Table 4
에서 ‘통증/불편’ 영역이model 3
에서 유의하지 않은 것으 로 미루어 보아 남성에서의 ‘통증/불편’ 영역은 고요산혈증보다 다 른 생활 요인들(흡연, 음주, 규칙적 운동, 교육수준)이 더 큰 영향을 미치는 것으로 판단된다(P<0
.05
).본 연구에서 고요산혈증은 남녀 연령 그룹 모두에서 정신건강(불 안/우울) 부분에 영향을 미치지 않았고 신체적 기능 부분에 주로 영 향을 미쳤다.
60
세 이상의 여성에서는 고요산혈증과EQ-5D
연관성 이 유의하지 않았는데 고령 여성에서EQ-5D
에 크게 영향을 주는 것 은 고요산혈증과 같은 요인보다는 당뇨나 고혈압 등의 만성질환, 암 이나 생활 요인들이EQ-5D
에 더 중요한 요인으로 작용하기 때문에 이러한 결과가 나온 것으로 생각된다.고요산혈증과 건강 관련 삶의 질에 대한 기존 연구는 부족한 실 정으로
Dalbeth
등27)의 연구에서는 혈중 요산 농도가HQoL
저하와 관련 있다고 밝혔고Roddy
등28)의 연구에서는 통풍 환자를 혈중 요 산 농도를360
μmol
/L
를 기준으로 두 그룹으로 나누어 삶의 질을 평가했을 때 전체 또는 개별 영역(물리적, 심리적, 사회적, 환경적)에 서Q
OL
차이가 발견되지 않았다.반면 체내에 과잉 축적된 요산이 결정화되면서 관절과 관절 주위 조직에 반복적으로 염증을 일으키는 통풍의 경우에는 심한 관절통 과 관절 변형을 유발29)시키기 때문에 이로 인한 삶의 질 저하에 대 한 연구는 많이 시행되었다. 통풍과 삶의 질의 연관성에 대한 이전 연구들을 살펴보면
Roddy
등28)이2007
년 영국 노팅엄에서3
,082
명을 대상으로World Health Organization-QoL Bref instrument
을 이용하여 삶의 질을 평가했는데QoL
의 전체 등급과 건강 만족도는 대조군보 다 유의하게 낮았으며 각 영역의 비교에서 신체 건강과 관련된QoL
은 대조군보다 유의하게 낮았으나 심리적 건강, 사회적 또는 환경 영 역에서 유의한 차이는 발견되지 않았다.Chandratre
등30)의 연구에 서도 통풍은 다른 영역에 비해 신체적인HQoL
에 더 큰 영향을 미쳤 으며 통풍 특이 증상(발작 빈도와 강도, 관절염 통증 및 관절 수 포함) 및 합병증은
HQoL
저하와 관련이 있었다.본 연구에서 삶의 질을 평가하기 위해
EQ-5D
방법을 사용한 것 과는 달리 통풍과 건강 관련 삶의 질에 대한 다른 연구들에서는HAQ-DI
와Short Form 36
등을 주로 사용하였다.30)EQ-5D
에 추가하 여 삶의 질을 평가하는 다른 방법들도 사용하여 연구한다면 좀더 심층적인 분석을 할 수 있을 것이다. 이번 연구에서는 남성과 여성 을 별도로 분류하지 않고 고요산혈증의 정의를7 mg
/dL
로 정의하 였으나 다른 연구들에서처럼 성별에 따라 정의를 달리하는 것을 적 용한다면 남녀 각각에서의 고요산혈증 유병률이나HQoL
의 연관성 결과에 차이가 있을 것으로 생각한다. 본 연구는 단면 연구이며 고 요산혈증과 삶의 질 사이의 시간적 선후 관계가 명확하지 않고 자기 기입식 설문 조사에 의해EQ-5D
가 조사되어 개인의 주관적 판단과 기억 오류의 가능성이 있으며 요산저하제 복용으로 혈중 요산 농도 가 정상 레벨로 유지되고 있는 그룹에 대해서는 파악할 수 없었다.이번 연구는 한국인을 대표할 수 있는 대규모 집단을 대상으로 시행한 국민건강영양조사 자료를 토대로 고요산혈증이 노인 인구 뿐만 아니라
20–30
대의 젊은 인구에도 건강 관련 삶의 질에 영향을 미침을 밝힌 연구라는 것에 의의가 있으며 이들에게도 고요산혈증 의 적절한 관리가 필요함을 시사한다.요 약
연구배경: 본 연구는 우리나라 성인 인구를 대상으로 고요산혈증 과 건강 관련 삶의 질의 관계에 대한 연구를 시행하였다.
방법: 국민건강영양조사 제
7
기1
,2
차년도에 참여한 만19
세 이상의 대한민국 남녀4
,969
명을 대상으로 혈중 요산 농도7 mg
/dL
이상을 고요산혈증으로 정의하고 건강 관련 삶의 질은HQoL
측정 도구인EuroQoL 5 dimension
(EQ-5D
),EQ-5D index
를 이용하여 로지스틱 회귀분석을 시행하였다.결과:
EQ-5D index
는 연령 증가에 따라 고요산혈증이 있는 남녀 모 두에서 정상 그룹보다 유의하게 감소하였다(P<0
.05
). 고요산혈증과EQ-5D
의 로지스틱 회귀분석에서 남성은 고요산혈증 그룹에서 신체조건, 만성질환, 생활 요인들에 대해 보정하여 분석한 결과에서도
‘운동능력’
odds ratio
(OR
),1
.46
(95
%confidence interval [CI]
,1
.211–
1
.683
)은 고요산혈증에 의해 삶의 질이 저하되는 것으로 나타났다.여성에서는 ‘운동능력’
OR
,1
.33
(95
%CI
,0
.716–2
.464
)은 통계적 유 의성은 없었다.결론: 고요산혈증이 있는 경우 건강 관련 삶의 질이 유의하게 저하 되었으며 정신 건강 부분보다는 신체적 기능 부분에서 주로 저하되 었다.
Zee Hae Bang, et al. Hyperuricemia and Health-Related Quality of Life
Korean Journal of Family Practice
KJFP
중심단어: 혈중 요산 농도; 고요산혈증; 건강 관련 삶의 질; 성인 CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported
. ORCIDZee Hae Bang
,http
://orcid
.org
/0000-0002-8496-9518 Yeon Ji Lee
,http
://orcid
.org
/0000-0001-7712-996X Ji-Ho Choi
,http
://orcid
.org
/0000-0002-5194-930X Yoohyun Kim
,http
://orcid
.org
/0000-0002-4742-5722 Sung Hee An
,http
://orcid
.org
/0000-0001-9658-5530 Min Kyoung Lee
,http
://orcid
.org
/0000-0002-6587-3617 Sangsook Lee
,http
://orcid
.org
/0000-0002-6377-9598
REFERENCES1. Zhu Y, Pandya BJ, Choi HK. Prevalence of gout and hyperuricemia in the US general population: the National Health and Nutrition Examination Survey 2007-2008. Arthritis Rheum 2011; 63: 3136-41.
2. Qiu L, Cheng XQ, Wu J, Liu JT, Xu T, Ding HT, et al. Prevalence of hyperuricemia and its related risk factors in healthy adults from Northern and Northeastern Chinese provinces. BMC Public Health 2013; 13: 664.
3. Kim Y, Kang J, Kim GT. Prevalence of hyperuricemia and its associated factors in the general Korean population: an analysis of a population-based nationally representative sample. Clin Rheumatol 2018; 37: 2529-38.
4. Kannangara DR, Phipps-Green AJ, Dalbeth N, Stamp LK, Williams KM, Gra- ham GG, et al. Hyperuricaemia: contributions of urate transporter ABCG2 and the fractional renal clearance of urate. Ann Rheum Dis 2016; 75: 1363-6.
5. Ames BN, Cathcart R, Schwiers E, Hochstein P. Uric acid provides an antioxi- dant defense in humans against oxidant- and radical-caused aging and cancer: a hypothesis. Proc Natl Acad Sci U S A 1981; 78: 6858-62.
6. Billiet L, Doaty S, Katz JD, Velasquez MT. Review of hyperuricemia as new marker for metabolic syndrome. ISRN Rheumatol 2014; 2014: 852954.
7. Nicholls A, Snaith ML, Scott JT. Effect of oestrogen therapy on plasma and uri- nary levels of uric acid. Br Med J 1973; 1: 449-51.
8. Fang J, Alderman MH. Serum uric acid and cardiovascular mortality the NHANES I epidemiologic follow-up study, 1971-1992. JAMA 2000; 283: 2404- 10.
9. Yamanaka H, Metabolism TG. Essence of the revised guideline for the manage- ment of hyperuricemia and gout. Japan Med Assoc J 2012; 55: 324-9.
10. Nakagawa T, Tuttle KR, Short RA, Johnson RJ. Hypothesis: fructose-induced hyperuricemia as a causal mechanism for the epidemic of the metabolic syn- drome. Nat Clin Pract Nephrol 2005; 1: 80-6.
11. Krishnan E, Baker JF, Furst DE, Schumacher HR. Gout and the risk of acute myocardial infarction. Arthritis Rheum 2006; 54: 2688-96.
12. Cannon PJ, Stason WB, Demartini FE, Sommers SC, Laragh JH. Hyperurice- mia in primary and renal hypertension. N Engl J Med 1966; 275: 457-64.
13. Schretlen DJ, Inscore AB, Vannorsdall TD, Kraut M, Pearlson GD, Gordon B, et al. Serum uric acid and brain ischemia in normal elderly adults. Neurology 2007; 69: 1418-23.
14. Roberts JM, Bodnar LM, Lain KY, Hubel CA, Markovic N, Ness RB, et al. Uric acid is as important as proteinuria in identifying fetal risk in women with gesta- tional hypertension. Hypertension 2005; 46: 1263-9.
15. Siu YP, Leung KT, Tong MK, Kwan TH. Use of allopurinol in slowing the pro- gression of renal disease through its ability to lower serum uric acid level. Am J Kidney Dis 2006; 47: 51-9.
16. Bhole V, Choi JW, Kim SW, de Vera M, Choi H. Serum uric acid levels and the risk of type 2 diabetes: a prospective study. Am J Med 2010; 123: 957-61.
17. Lam CL, Lauder IJ. The impact of chronic diseases on the health-related quality of life (HRQOL) of Chinese patients in primary care. Fam Pract 2000; 17: 159- 66.
18. Konstam V, Salem D, Pouleur H, Kostis J, Gorkin L, Shumaker S, et al. Baseline quality of life as a predictor of mortality and hospitalization in 5,025 patients with congestive heart failure. SOLVD Investigations. Studies of Left Ventricular Dysfunction Investigators. Am J Cardiol 1996; 78: 890-5.
19. Rabin R, de Charro F. EQ-5D: a measure of health status from the EuroQol Group. Ann Med 2001; 33: 337-43.
20. Dorman PJ, Waddell F, Slattery J, Dennis M, Sandercock P. Is the EuroQol a valid measure of health-related quality of life after stroke? Stroke 1997; 28: 1876-82.
21. Schlesinger N, Schumacher HR Jr. Update on gout. Arthritis Rheum 2002; 47:
563-5.
22. Rebollo P, Ortega F, Baltar JM, Díaz-Corte C, Navascués RA, Naves M, et al.
Health-related quality of life (HRQOL) in end stage renal disease (ESRD) pa- tients over 65 years. Geriatr Nephrol Urol 1998; 8: 85-94.
23. Bottomley A, Pe M, Sloan J, Basch E, Bonnetain F, Calvert M, et al.; Setting Inter- national Standards in Analyzing Patient-Reported Outcomes and Quality of Life Endpoints Data (SISAQOL) consortium. Analysing data from patient-re- ported outcome and quality of life endpoints for cancer clinical trials: a start in setting international standards. Lancet Oncol 2016; 17: e510-4.
24. Kim JS, Oh MK, Park BK, Lee MK, Kim GJ. Screening criteria of alcoholism by alcohol use disorders identification test(AUDIT) in Korea. J Korean Acad Fam Med 1999; 20: 1152-9.
25. Lee YK, Nam HS, Chuang LH, Kim KY, Yang HK, Kwon IS, et al. South Korean time trade-off values for EQ-5D health states: modeling with observed values for 101 health states. Value Health 2009; 12: 1187-93.
26. Craig CL, Marshall AL, Sjöström M, Bauman AE, Booth ML, Ainsworth BE, et al. International physical activity questionnaire: 12-country reliability and validi- ty. Med Sci Sports Exerc 2003; 35: 1381-95.
27. Dalbeth N, Petrie KJ, House M, Chong J, Leung W, Chegudi R, et al. Illness per- ceptions in patients with gout and the relationship with progression of muscu- loskeletal disability. Arthritis Care Res (Hoboken) 2011; 63: 1605-12.
28. Roddy E, Zhang W, Doherty M. Is gout associated with reduced quality of life? A case-control study. Rheumatology (Oxford) 2007; 46: 1441-4.
29. Choi HK, Mount DB, Reginato AM; American College of Physicians, American Physiological Society. Pathogenesis of gout. Ann Intern Med 2005; 143: 499-516.
30. Chandratre P, Roddy E, Clarson L, Richardson J, Hider SL, Mallen CD. Health- related quality of life in gout: a systematic review. Rheumatology (Oxford) 2013;
52: 2031-40.