서 론
대사증후군은 고혈압, 복부비만, 이상지질혈증 그리고 내당능장 애 등의 임상적인 특징들로 구성되어 있으며, 최근 서구화되고 있는 식생활 등 생활습관의 변화로 우리나라 대사증후군 유병률은 꾸준 히 증가하고 있다.1) 대사증후군 관련 요인으로 음주, 흡연 및 식생활 습관 등을 포함한 후천적인 환경인자가 밀접히 관련되어 있으나 아 직 당뇨 발생의 정확한 병태생리는 밝혀져 있지 않다.2,3)
대사증후군과 관련된 요인 중 소량의 음주나 건강한 음주행태는 심혈관질환 관련 사망률을 낮추고, 심근경색의 상대적 위험도를 낮
추며, 이상지질혈증에서 콜레스테롤 수치를 개선시킬 수 있다.3-5) 적 당한 알코올 섭취는 고밀도지단백 콜레스테롤(high density lipopro- tein [HDL] cholesterol)을 증가시켜 죽상동맥경화 위험도를 낮추고 혈 전용해를 증가시키는 등의 효과가 있기 때문이다.6,7) 그러나 일부 연 구에서는 알코올 섭취량이 증가할수록 혈압이 높아지고, 중성지방 (triglyceride, TG)이 증가하는 등의 보고도 있어 알코올 섭취와 이상 지질혈증과의 관계는 명확하지 않다.8-11)
한편 미국, 캐나다, 호주 등 세계 각국에서는 금주와 더불어 건전 한 음주를 위하여 가이드라인을 제시하고 있다.12-14) 우리나라에서도 국민건강증진종합계획 등을 통해 건전한 음주를 위하여 다양한 노
Original Article
건강음주행태와 대사증후군의 관계
김광진, 정 혁, 박경택, 김문택, 오택근, 이석환, 김현우*
대구의료원 가정의학과
Relation between Healthy Drinking Habits and Metabolic Syndrome
Kwang-Jin Kim, Hyuk Jung, Kyung-Taek Park, Mun-Taek Kim, Teak-Geon Oh, Seock-Hwan Lee, Hyun-Woo Kim*
Department of Family Medicine, Daegu Medical Center, Daegu, Korea
Background: Alcoholic drinking habits could affect the development of metabolic syndrome. However, the relationship between drinking habits and metabolic syndrome is not clear.
Methods: This study examined drinking habits and metabolic syndrome in 6,713 healthy adults who took a medical health examination in 2014. We divided participants into two groups, and patients were classified as ‘non-drinkers’ or ‘healthy drinkers’ according to Canada’s low-risk drinking guidelines. The relationship between drinking habits and metabolic syndrome was assessed by performing cross-sectional analysis.
Results: In men, high density lipoprotein (HDL) cholesterol was significantly higher and the odds ratio of metabolic syndrome was lower in the ‘healthy drinkers’ group (P< 0.05). In addition, low density lipoprotein (LDL) cholesterol and triglyceride levels tended to be lower, but this result was not statistically significant (P> 0.05). In women, healthy drinkers exhibited lower blood pressure, body mass index (BMI), fasting glucose, LDL cholesterol, triglyceride, and total cholesterol levels, as well as better liver function test values, a lower prevalence of metabolic syndrome, and a lower odds ratio of metabolic syndrome.
Conclusion: We verified that healthy drinking habits are related to lower levels of BMI, dyslipidemia, blood pressure, HDL cholesterol, and a lower odds ratio of metabolic syndrome. Additional studies are needed to confirm these results.
Keywords: Alcohol Drinking; HDL Cholesterol; Metabolic Syndrome; Blood Pressure; Healthy Drinking Habits
http://www.kafm.or.kr/kjfp.2015.5.3.361pISSN 2233-9019 · eISSN 2233-9116 Korean J Fam Pract. 2015;5(3):361-367
KJFP
Korean Journal of Family PracticeReceived February 24, 2015 Accepted August 28, 2015 Corresponding author Hyun-Woo Kim
Tel: +82-53-560-7390, Fax: +82-53-560-7499 E-mail: [email protected]
Copyright © 2015 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Kwang-Jin Kim, et al. Healthy Drinking Habits and Metabolic Syndrome
Korean Journal of Family Practice
KJFP
력을 하고 있다.15) 이러한 배경하에 본 연구에서는 일개병원 건강검 진센터를 방문한 성인을 대상으로 건강한 음주군을 중심으로 대사 증후군의 각 요소와의 관계를 알아보고자 하였다.
방 법
1. 연구대상
본 연구에서는 2014년 1월 1일에서 12월 31일까지 대구의료원 건강 증진센터에 방문하여 건강검진을 시행한 20세부터 70세 사이의 남 녀 수검자 10,534명을 대상으로 하였다. 이 중에서 자가보고를 통해 체크한 설문지를 통해 알코올 섭취량과 주당 횟수를 조사하였으며, 캐나다 건강음주지침14)을 기준으로 과음 음주군, 관련 설문에 응하 지 않은 사람 및 검사 값이 누락된 사람 3,821명을 제외한 성인 남자 2,867명, 여자 3,846명, 총 6,713명을 대상으로 실시하였다. 과음 음주 군은 대사증후군의 유병률이 증가하고, 뇌심혈관질환 관련 발병률 및 사망률이 높아지는 등의 위험성이 알려져 있어6) 본 연구대상에서 제외하였다.
2. 연구방법
1) 설문조사각 수검자들은 자가기입식 설문지를 통하여 자신의 생활습관, 가 족력, 과거력 등을 기록하였고, 미완성된 부분에 대하여는 면담을 통 해 완성하였다. 생활습관을 묻는 질문에는 1주일간 음주빈도, 음주 종류와 상관없이 잔수를 기준으로 1회 음주량, 흡연 여부 등이 포함 되어 있으며, 1주일간 평균 운동 횟수는 하루 30분 이상을 1회로 하 여 조사되었다.
2) 신체계측 및 혈압
수검자들은 키, 몸무게, 혈압 등을 측정하였다. 키, 몸무게는 가벼 운 검진용 실내 가운 및 맨발상태 또는 양말 등의 상태에서 자동계측 기를 이용하여 측정하였고, 체질량지수(body mass index, BMI)는 몸 무게(kg)/키(m2)의 공식을 통하여 계산하였다.
3) 혈액검사
수검자들은 12시간 이상 금식한 상태에서 정맥혈을 채혈하여 공 복혈당(fasting glucose), TG, 총 콜레스테롤(total cholesterol), HDL 콜 레스테롤을 측정하였고, 저밀도지단백 콜레스테롤(low density lipo- protein [LDL] cholesterol)은 LDL cholesterol=total cholesterol–HDL cholesterol–TG/5 공식을 이용하여 계산하였다.
4) 음주군의 정의
수검자들이 작성한 설문지를 바탕으로 1주일간 음주횟수 0회, 음 주량 0잔인 군을 금주군(non-drinker)으로 하였다. 건강음주군 (healthy drinker)은 캐나다 건강음주지침14)을 기준으로 남자는 1회당 음주량이 3잔 이하이면서 1주일 15잔 이하인 경우, 여자는 1회당 음 주량이 2잔 이하이면서 1주일 10잔 이하인 경우로 하였다. 그 이상의 음주자는 대상에서 제외하였다.
5) 대사증후군 기준
대사증후군의 기준은 National Cholesterol Education Program Adult Treatment Panel III를 따랐다. 다만 건강검진 시 허리둘레는 BMI로 대 체하였다.16) (1) 복부비만: BMI 25 kg/m2 이상, (2) 고혈압: 수축기혈압 135 mm Hg 이상, 이완기혈압 80 mm Hg 이상 또는 고혈압 약물을 복 용 중인 자, (3) 고중성지방혈증: TG 150 mg/dL 이상 또는 이상지질혈 증으로 약물 복용 중인 자, (4) 저고밀도지단백혈증: HDL cholesterol 이 남자는 40 mg/dL 이하, 여성은 50 mg/dL 이하인 자, (5) 공복혈당: 공 복혈당이 100 mg/dL 이상이거나 당뇨병 약물을 복용 중인 자.
3. 통계분석
본 연구자료는 통계프로그램 R ver. 3.1.2 (Free Software Foundation Inc., Boston, MA, USA)을 사용하였다. 모든 분석은 남녀로 구분하여 시행하였으며, 실수, 평균± 표준편차 및 백분율로 표시하였다. 금주 군과 건강음주군의 평균 비교분석에서는 t-test, 카이제곱 검정 및 로 지스틱회귀분석법을 사용하여 분석하였다. P-value<0.05를 유의한 통계학적 수준으로 하였다.
결 과
1. 대상자의 기본 특성
연구대상자는 남자 2,867명(42.7%), 여자 3,846명(57.3%)으로 총 6,713명이었고, 평균 나이는 남자 53.7±12.1세, 여자 53.1±12.1세였다 (P= 0.069). 남자의 평균 수축기혈압 124.9±14.0 mm Hg, 이완기혈압 75.3±9.9 mm Hg으로 여자보다 높았으며, 남자 평균 BMI는 23.7±3.1 kg/m2, 평균 공복혈당은 100.3±33.1 mg/dL로 여자보다 높았다. HDL cholesterol은 남자 50.5±12.9 mg/dL, 여자 59.8±13.5 mg/dL로 여자에 서 더 높았다(Table 1).
2. 남성 및 여성에서 금주군과 건강음주군 간의 대사증후군 각 요소의 차이
남성에서 건강음주군의 공복혈당은 98.4± 25.7 mg/dL로 금주군
김광진 외. 건강음주행태와 대사증후군의 관계 Korean Journal of Family Practice
KJFP
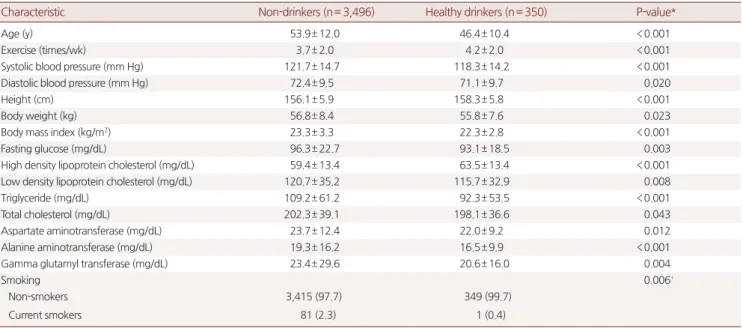
100.9±35.1 mg/dL에 비해 낮은 평균값을 보였으며, HDL cholesterol은 53.6±13.7 mg/dL로 높은 평균값을 보였고, 통계적으로도 유의하였 다(P<0.05). LDL cholesterol, TG, BMI 등은 금주군보다 낮은 값을 보 였으나 통계적으로 유의하지는 않았다(Table 2). 여성에서 건강음주 군에서 수축기혈압은 118.3±14.2 mm Hg, 이완기혈압 71.1±9.7 mm Hg로 금주군보다 낮았으며, BMI 22.3± 2.8 kg/m2, 공복혈당 93.1±18.5 mg/dL, TG 92.3±53.5 mg/dL, 총 콜레스테롤 198.1±36.6 mg/dL로 금
주군에 비해 낮았고, HDL cholesterol은 높은 평균값을 보였으며 통 계적으로 유의하였다(P<0.05) (Table 3).
3. 남성 및 여성에서 금주군과 건강음주군 간의 대사증후군 유병률 및 각 요소의 유병률 차이
남성의 건강음주군은 금주군에 비하여 대사증후군 유병률이 23.6%로 낮았고(P<0.05), 대사증후군 각 요소별로 모두 낮은 유병률
Table 1. Baseline characteristics of subjects
Characteristic Male (n= 2,867) Female (n= 3,846) P-value*
Age (y) 53.7± 12.1 53.1± 12.1 0.069
Exercise (times/wk) 4.0± 2.1 3.7± 2.0 <0.001
Systolic blood pressure (mm Hg) 124.9± 14.0 121.4± 14.6 <0.001
Diastolic blood pressure (mm Hg) 75.3± 9.9 72.3± 9.5 <0.001
Height (cm) 168.6± 6.6 156.3± 5.9 <0.001
Body weight (kg) 67.6± 10.5 56.7± 8.3 <0.001
Body mass index (kg/m2) 23.7± 3.0 23.2± 3.3 <0.001
Fasting glucose (mg/dL) 100.3± 33.1 96.0± 22.4 <0.001
High density lipoprotein cholesterol (mg/dL) 50.5± 12.9 59.8± 13.5 <0.001
Low density lipoprotein cholesterol (mg/dL) 116.5± 34.3 120.2± 35.0 <0.001
Triglyceride (mg/dL) 136.2± 83.2 107.7± 60.7 <0.001
Total cholesterol (mg/dL) 194.6± 38.0 202.0± 38.9 <0.001
Aspartate aminotransferase (mg/dL) 25.3± 10.9 23.6± 12.1 <0.001
Alanine aminotransferase (mg/dL) 25.3± 17.5 19.0± 15.7 <0.001
Gamma glutamyl transferase (mg/dL) 37.5± 49.5 23.2± 28.7 <0.001
Drinkers <0.001†
Non-drinkers 2,165 (75.5) 702 (24.5)
Healthy drinkers 3,496 (90.9) 350 (9.1)
Values are presented as mean± standard deviation or number (%) unless otherwise indicated.
*Calculated by t-test. †Pearson’s chi-square test.
Table 2. Subject characteristics of non-drinkers vs. healthy drinkers on male
Characteristic Non-drinkers (n= 2,165) Healthy drinkers (n= 702) P-value*
Age (y) 54.3± 12.0 51.9± 12.2 <0.001
Exercise (times/wk) 3.9± 2.0 4.4± 2.0 <0.001
Systolic blood pressure (mm Hg) 124.8± 13.8 125.2± 14.4 0.455
Diastolic blood pressure (mm Hg) 75.2± 9.6 75.6± 10.2 0.374
Height (cm) 168.2± 6.7 169.8± 6.2 <0.001
Body weight (kg) 67.4± 10.9 68.2± 9.3 0.057
Body mass index (kg/m2) 23.8± 3.2 23.6± 2.7 0.271
Fasting glucose (mg/dL) 100.9± 35.1 98.4± 25.7 0.045
High density lipoprotein cholesterol (mg/dL) 49.5± 12.4 53.6± 13.7 <0.001
Low density lipoprotein cholesterol (mg/dL) 116.8± 34.9 115.4± 32.4 0.334
Triglyceride (mg/dL) 136.8± 84.0 134.1± 80.9 0.460
Total cholesterol (mg/dL) 194.0± 39.1 196.2± 34.4 0.162
Aspartate aminotransferase (mg/dL) 25.3± 11.3 25.5± 9.6 0.650
Alanine aminotransferase (mg/dL) 25.5± 18.2 24.7± 14.8 0.219
Gamma glutamyl transferase (mg/dL) 36.4± 51.7 40.7± 41.8 0.046
Smoking 0.180†
Non-smokers 1,427 (66.0) 482 (68.7)
Current smokers 738 (34.0) 220 (31.3)
Values are presented as mean± standard deviation or number (%) unless otherwise indicated.
*Calculated by t-test. †Pearson’s chi-square test.
Kwang-Jin Kim, et al. Healthy Drinking Habits and Metabolic Syndrome
Korean Journal of Family Practice
KJFP
을 보였으나 LDL에서만 통계적으로 유의하였고, 다른 항목에서는 통 계적으로 유의하지 않았다. 여성에서는 건강음주군의 대사증후군 유병률은 38명(10.9%)이었였다. 건강음주군에서 대사증후군 각 요소 별로 보면 복부비만 53명(15.1%), 고혈압 102명(29.1%), 공복혈당 62명 (17.7%), 저고밀도지단백혈증 59명(16.9%), 고중성지방혈증 42명(12.0%) 로 나타났다. 여성에서 건강음주군의 대사증후군 유병률이 10.9%로 금주군에 비하여 낮았으며 통계적으로 유의하였다(P<0.05). 대사증 후군 각 요소별로 유병률 역시 모든 항목에서 금주군에 비하여 낮은 유병률을 보였으며 통계적으로 유의하였다(P<0.05) (Table 4).
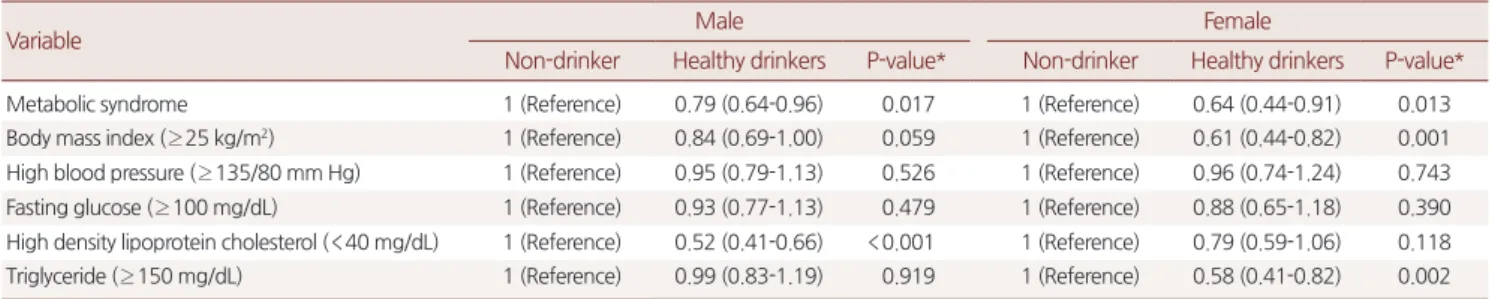
4. 남성 및 여성에서 금주군과 건강음주군 간의 대사증후군 및 각 요소의 교차비
남성의 대사증후군 발생 교차비를 보면 건강음주군은 금주군에
비하여 0.79배(0.64-0.96)만큼 적게 발생하는 것으로 조사되었다. BMI 는 0.84배(0.69-1.00), 고혈압 0.95배(0.79-1.13), 저고밀도지단백혈증 0.52배(0.41-0.66) 등으로 나타났다. 여성의 경우 대사증후군은 0.64배 (0.44-0.91)로 조사되었고, 각 요소별로는 BMI 0.61배(0.44-0.82), 고중 성지방혈증 0.58배(0.41-0.82)로 조사되었다(Table 5).
고 찰
우리나라의 1인당 술 소비량은 1987년 약 10.6 리터/년/인이었으나 이후 지속적으로 감소하였다.17) 2013년 Organization for Economic Cooperation and Development (OECD)에서 발표한 자료에 의하면 우 리나라의 15세 이상 1인당 평균 연간 술 소비량은 8.9 리터로 전체 OECD회원국 34개국 중에서 22위인 것으로 나타났으나 고위험 음주 Table 3. Subject characteristics of non-drinkers vs. healthy drinkers on female
Characteristic Non-drinkers (n= 3,496) Healthy drinkers (n= 350) P-value*
Age (y) 53.9± 12.0 46.4± 10.4 <0.001
Exercise (times/wk) 3.7± 2.0 4.2± 2.0 <0.001
Systolic blood pressure (mm Hg) 121.7± 14.7 118.3± 14.2 <0.001
Diastolic blood pressure (mm Hg) 72.4± 9.5 71.1± 9.7 0.020
Height (cm) 156.1± 5.9 158.3± 5.8 <0.001
Body weight (kg) 56.8± 8.4 55.8± 7.6 0.023
Body mass index (kg/m2) 23.3± 3.3 22.3± 2.8 <0.001
Fasting glucose (mg/dL) 96.3± 22.7 93.1± 18.5 0.003
High density lipoprotein cholesterol (mg/dL) 59.4± 13.4 63.5± 13.4 <0.001
Low density lipoprotein cholesterol (mg/dL) 120.7± 35.2 115.7± 32.9 0.008
Triglyceride (mg/dL) 109.2± 61.2 92.3± 53.5 <0.001
Total cholesterol (mg/dL) 202.3± 39.1 198.1± 36.6 0.043
Aspartate aminotransferase (mg/dL) 23.7± 12.4 22.0± 9.2 0.012
Alanine aminotransferase (mg/dL) 19.3± 16.2 16.5± 9.9 <0.001
Gamma glutamyl transferase (mg/dL) 23.4± 29.6 20.6± 16.0 0.004
Smoking 0.006†
Non-smokers 3,415 (97.7) 349 (99.7)
Current smokers 81 (2.3) 1 (0.4)
Values are presented as mean± standard deviation or number (%) unless otherwise indicated.
*Calculated by t-test. †Pearson’s chi-square test.
Table 4. The prevalence of metabolic syndrome and its components Variable
Male Female
Non-drinker (n= 2,165)
Healthy drinkers
(n= 702) P-value* Non-drinker (n= 3,496)
Healthy drinkers
(n= 350) P-value*
Metabolic syndrome 633 (29.2) 166 (23.6) 0.004 796 (22.8) 38 (10.9) <0.001
Body mass index (≥ 25 kg/m2) 727 (33.65) 217 (30.9) 0.191 955 (27.3) 53 (15.1) <0.001
High blood pressure (≥ 135/80 mm Hg) 1,102 (50.9) 335 (47.7) 0.143 1,395 (39.9) 102 (29.1) <0.001
Fasting glucose (≥ 100 mg/dL) 721 (33.3) 211 (30.1) 0.111 929 (26.6) 62 (17.7) <0.001
High density lipoprotein cholesterol (<40 mg/dL) 517 (23.9) 93 (13.2) <0.001 870 (24.9) 59 (16.9) 0.001
Triglyceride (≥ 150 mg/dL) 733 (33.9) 232 (33.0) 0.694 876 (25.1) 42 (12.0) <0.001
Values are presented as number (%) unless otherwise indicated.
*Pearson’s chi-square test.
김광진 외. 건강음주행태와 대사증후군의 관계 Korean Journal of Family Practice
KJFP
자 비율은 2005년 14.9%에서 2009년 17.1%로 증가하였다.18) 또한 2014 년 World Health Organization (WHO)에서 발표한 자료에 따르면 간 경변 등의 알코올 관련 질환(alcohol used disorder)의 유병률은 우리 나라가 6.3%(나이 보정)로 알코올 소비가 많은 일본 3.3%, 호주 3.7%보 다 더 높아 음주의 질이 좋지 않은 것으로 나타났으며.19) 과거 알코올 소비가 적었던 여성이나 저연령에서의 알코올 소비도 꾸준히 증가하 는 경향을 보이고 있다.20)
본 연구결과에서 여성에서 건강음주군의 수축기 및 이완기혈압 의 평균값이 금주군에 비하여 낮은 수치를 나타냈으며, 통계적으로 유의하였다. Klatsky 등21)이 83,947명을 대상으로 알코올 섭취와 혈압 과의 관계를 비교한 연구에서 비음주자와 하루 2-3잔을 마시는 음주 군과의 혈압은 유사한 결과를 보여 본 연구결과와 크게 다르지 않음 을 알 수 있다.
알코올 섭취량과 혈압과의 관계는 일반적으로 선형적 관계인 것 으로 알려져 있으나 하루 2-3잔의 음주가 혈압을 낮춘다는 보고도 있으며, 이는 소량의 알코올이 혈관이완작용(vasodilator)을 하기 때 문인 것으로 알려져 있다.9) 본 연구의 대사증후군 각 요소 중 고혈압 유병률 비교에서도 건강음주군의 고혈압 유병률이 남성 30.9%, 여성 15.1%로 금주군에 비하여 낮은 수치를 보였다(Table 4). 2010년 국민건 강영양조사를 이용한 Ryu와 Kim22)의 연구에 따르면 남성에서 low- risk drinking (Alcohol Use Disorder Identification Test [AUDIT] 점수 1-7)군이 non-drinking (AUDIT 0)이나 medium-level alcohol problem (AUDIT 8-15) 또는 high level alcohol problem (AUDIT>16)에 비하여 수축기혈압 135 mm Hg 이상 유병률이 11.9% (P= 0.006)로 다른 군에 비하여 가장 낮은 수치를 나타냈다는 보고도 있어 소량의 알코올 섭 취가 혈압을 낮추는 효과가 있는 것으로 생각된다.
35-59세 성인 일본 남성 832명을 대상으로 알코올 섭취와 혈청지질 의 관계를 본 Choudhury 등8) 연구에서 알코올을 섭취할수록 그렇지 않은 군에 비해 HDL cholesterol 및 TG는 증가하고 반면 LDL choles- terol은 낮아지는 결과를 보였다. 본 연구에서 HDL cholesterol은 남성,
여성 모두에서 건강음주군이 금주군에 비하여 높은 평균값을 보였 으며, 통계적으로 유의하였다. 남성 건강음주군의 HDL cholesterol 교 차비는 0.52배(0.41-0.66)로 낮은 발생률을 보였으며 통계적으로 유의 하였다(P<0.05). LDL cholesterol및 TG는 모두 낮은 평균값을 보였으 며, 여성에서 고중성지방혈증의 교차비는 0.58배(0.41-0.82)였고 통계 적으로 유의하였다. 적절한 알코올 섭취는 HDL cholesterol 수치를 상 승시켜 죽상동맥경화의 위험을 낮추는 것으로 보고 되었으나 아직 명확한 기전은 밝혀지지 않은 상태이다.10,11,23)
음주량에 따른 당뇨발생 또는 내당능장애 발생 등에 대해 아직 논 란이 많다. 적당한 알코올 섭취는 당뇨의 위험을 감소시킨다는 결과 도 있고, 다른 연구에서는 오히려 당뇨위험을 증가시킨다는 결과도
있다.23,24) 본 연구에서 남성 여성 모두에서 건강음주군의 공복혈당
이 금주군에 비해 낮은 결과를 보였으며 통계적으로 유의하였다.
알코올 섭취량에 따른 대사증후군 요소와의 관계를 알아본 Wak- abayashi25) 연구에서 허리둘레, TG 등에서 알코올 섭취량에 따라 J- and U- shape의 관계를 보였고, 대사증후군 유병률 또한 남녀 모두에 서 건강음주군이 금주군에 비해 대사증후군 유병률이 낮은 결과를 보였다. 본 연구에서도 건강음주군의 대사증후군 유병률 및 발생률 이 금주군에 비하여 낮았으며 통계적으로 유의하였다.
본 연구의 제한점으로는 첫째, 자기기입식 설문지를 통하여 생활 습관을 조사하여 대상자의 주관적인 의견이 포함되어 실제와 다르 게 조사되었을 가능성이 있다. 둘째, 검진을 받으러 오는 성인을 대상 으로 하였기 때문에 일반적인 인구집단에 비해 건강에 대한 관심이 높고, 그에 따라 평소 양호한 생활습관을 위해 노력했을 가능성이 있다. 셋째, 식사량 등의 생활습관요소 및 사회활동 유무, 소득수준 등의 사회경제적 요소가 대사증후군 요소들과 밀접한 관계가 있으
나,26,27) 본 연구에 사용된 검진데이터에는 이러한 자료가 포함되어
있지 않아 사용하지 못한 제한점이 있다. 마지막으로 본 연구는 단면 연구로 적당한 알코올 섭취와 대사증후군과의 인과관계를 설명하기 에는 한계가 있다.
Table 5. The results of logistic regression analysis of metabolic syndrome and its components
Variable Male Female
Non-drinker Healthy drinkers P-value* Non-drinker Healthy drinkers P-value*
Metabolic syndrome 1 (Reference) 0.79 (0.64-0.96) 0.017 1 (Reference) 0.64 (0.44-0.91) 0.013
Body mass index (≥ 25 kg/m2) 1 (Reference) 0.84 (0.69-1.00) 0.059 1 (Reference) 0.61 (0.44-0.82) 0.001 High blood pressure (≥ 135/80 mm Hg) 1 (Reference) 0.95 (0.79-1.13) 0.526 1 (Reference) 0.96 (0.74-1.24) 0.743 Fasting glucose (≥ 100 mg/dL) 1 (Reference) 0.93 (0.77-1.13) 0.479 1 (Reference) 0.88 (0.65-1.18) 0.390 High density lipoprotein cholesterol (<40 mg/dL) 1 (Reference) 0.52 (0.41-0.66) <0.001 1 (Reference) 0.79 (0.59-1.06) 0.118 Triglyceride (≥ 150 mg/dL) 1 (Reference) 0.99 (0.83-1.19) 0.919 1 (Reference) 0.58 (0.41-0.82) 0.002 Values are presented as odds ratio and 95% confidence interval unless otherwise indicated. Odds ratio are adjusted for age, smoking, and exercise.
*Logistic regression analyzed.
Kwang-Jin Kim, et al. Healthy Drinking Habits and Metabolic Syndrome
Korean Journal of Family Practice
KJFP
본 연구에서 캐나다 가이드라인에 따라 건강음준군을 정한 이유 는 WHO에서의 건강음주는 적정 알코올 섭취량을 기준으로 남자 40 g/일, 여자 20 g/일로 정의하고 있고, 우리나라 역시 비슷한 1회 음 주량을 기준으로 되어 있는 반면, 캐나다의 기준은 1회 알코올 섭취 량뿐만 아니라 주당 알코올 섭취량까지 포함되어 있어, 1회 알코올 섭취는 적으나 알코올 섭취 빈도가 많아 주당 알코올 섭취량이 많은 대상자는 건강음주군에서 배제하여 보다 정확한 건강음주군을 정 할 수 있었기 때문이다. 그러나 캐나다의 알코올 종류에 따라 한 잔 에 포함된 알코올량이 우리나라와 다를 수 있어 건강음주군에 대한 기준이 제한적인 요소로 작용할 수 있겠다.21)
결론적으로, 본 연구에서 건강음주군의 대사증후군의 각 요소별 평균값이나 유병률, 발생률이 금주군에 비하여 양호한 결과를 보였 으며, 이는 건강음주행태가 대사증후군 위험도 감소에 주요한 역할 을 할 가능성을 제시한다. 따라서 향후 이에 대한 전향적 연구가 필 요하다.
요 약
연구배경:
알코올은 대사증후군 및 심뇌혈관질환과 관련된 위험인 자이다. 본 연구에서는 건강한 성인을 대상으로 적절한 음주와 대사 증후군과의 관계를 알아보고자 하였다.방법:
2014년 대구의료원 건강증진센터에 방문한 20-70세 10,534명 중 과음군 및 데이터가 누락된 3,821명을 제외한 남자 2,867명, 여자 3,846명, 총 6,713명을 대상으로 실시하였다. 음주종류와 상관없이 잔 수를 기준으로 1주일간 음주횟수 0회, 음주량 0잔인 대상자를 금주 군으로, 캐나다 건강음주지침에 따라 남자는 1회 음주량이 3잔 이하 이면서 1주일 음주량이 15잔 이하인 대상자, 여성은 1회 음주량이 2 잔 이하이면서 1주일 음주량이 10잔 이하인 대상자를 건강음주군으 로 분류하여 대사증후군 각 요소 및 간기능검사 등으로 조사하여 각 군의 평균값, 유병률 및 발생률을 t-test, 카이제곱 검정, 로지스틱 회귀분석으로 비교분석하였다.결과:
남성에서 건강음주군의 고밀도지단백이 금주군에 비해 유의 하게 증가되었으나(P<0.001), 저밀도지단백, 중성지방 등은 낮은 평 균값을 보였고, 통계적으로 유의하지 않았다. 건강음주군의 대사증 후군 유병률은 23.6%, 교차비는 0.79 (0.64-0.96)로 금주군에 비하여 낮았다(P<0.05). 여성에서 건강음주군은 수축기혈압, 이완기혈압, 체 질량지수, 공복혈당, 저밀도지단백, 중성지방, 총 콜레스테롤 및 간기 능 수치가 금주군에 비해 낮았으며 통계적으로 유의하였다(P<0.05).고밀도지단백은 건강음주군에서 더 높았으며, 통계적으로 유의하였 다(P<0.05). 여성의 건강음주군에서 대사증후군 유병률은 10.9%, 교
차비는 0.64 (0.44-0.91)로 금주군에 비하여 낮았으며, 대사증후군 각 요소별 발생률 역시 모두 낮은 경향을 보였다.
결론:
본 연구에서 건강음주군의 대사증후군의 각 요소별 평균값이 나 유병률, 발생률이 금주군에 비하여 양호한 결과를 보였으며, 이는 건강음주행태가 대사증후군 위험도 감소에 주요한 역할을 할 가능 성을 제시한다. 따라서 향후 이에 대한 전향적 연구가 필요하다.중심단어:
알코올; HDL Cholesterol; 대사증후군; 혈압; 건강음주군 REFERENCES1. Lim S, Shin H, Song JH, Kwak SH, Kang SM, Won Yoon J, et al. Increasing prevalence of metabolic syndrome in Korea: the Korean National Health and Nutrition Examination Survey for 1998-2007. Diabetes Care 2011;34:1323-8.
2. Liese AD, Mayer-Davis EJ, Tyroler HA, Davis CE, Keil U, Schmidt MI, et al.
Familial components of the multiple metabolic syndrome: the ARIC study.
Diabetologia 1997;40:963-70.
3. Nam SM, Yu HY, Lee MY, Koh JH, Shin JY, Shin YG, et al. Alcohol consump- tion, liver enzymes, and prevalence of metabolic syndrome in Korean adult men. J Korean Diabetes Assoc 2007;31:253-60.
4. Pannier B, Thomas F, Eschwege E, Bean K, Benetos A, Leocmach Y, et al.
Cardiovascular risk markers associated with the metabolic syndrome in a large French population: the “SYMFONIE” study. Diabetes Metab 2006;32(5 Pt 1):467-74.
5. Yoon YS, Oh SW, Baik HW, Park HS, Kim WY. Alcohol consumption and the metabolic syndrome in Korean adults: the 1998 Korean National Health and Nutrition Examination Survey. Am J Clin Nutr 2004;80:217-24.
6. Costanzo S, Di Castelnuovo A, Donati MB, Iacoviello L, de Gaetano G. Al- cohol consumption and mortality in patients with cardiovascular disease: a meta-analysis. J Am Coll Cardiol 2010;55:1339-47.
7. Kloner RA, Rezkalla SH. To drink or not to drink?: that is the question. Cir- culation 2007;116:1306-17.
8. Choudhury SR, Ueshima H, Kita Y, Kobayashi KM, Okayama A, Yamakawa M, et al. Alcohol intake and serum lipids in a Japanese population. Int J Epi- demiol 1994;23:940-7.
9. Dyer AR, Stamler J, Paul O, Berkson DM, Shekelle RB, Lepper MH, et al. Al- cohol, cardiovascular risk factors and mortality: the Chicago experience.
Circulation 1981;64(3 Pt 2):III 20-7.
10. De Oliveira E Silva ER, Foster D, McGee Harper M, Seidman CE, Smith JD, Breslow JL, et al. Alcohol consumption raises HDL cholesterol levels by in- creasing the transport rate of apolipoproteins A-I and A-II. Circulation 2000;102:2347-52.
11. Stampfer MJ, Colditz GA, Willett WC, Speizer FE, Hennekens CH. A pro- spective study of moderate alcohol consumption and the risk of coronary disease and stroke in women. N Engl J Med 1988;319:267-73.
12. Dietary Guidelines Advisory Committee. Report of the Dietary Guidelines Advisory Committee on the Dietary Guidelines for Americans, 2010 [Inter- net]. Washington (DC): U.S. Department of Agriculture; 2010 [cited 2015
김광진 외. 건강음주행태와 대사증후군의 관계 Korean Journal of Family Practice
KJFP
Feb 12]. Available from: http://www.cnpp.usda.gov/sites/default/files/di- etary_guidelines_for_americans/2010DGACReport-camera-ready- Jan11-11.pdf.
13. Health N, Council MR. Australian guidelines to reduce health risks from drinking alcohol [Internet]. Canberra: Commonwealth of Australia; 2009 [cited 2015 Feb 12]. Available from: https://www.nhmrc.gov.au/_files_nhm- rc/publications/attachments/ds10-alcohol.pdf.
14. National Alcohol Strategy Advisory Committee, Canadian Centre on Sub- stance Abuse. Canada’s low-risk alcohol drinking guidelines 2013 [Internet].
Ottawa: Canadian Centre on Substance Abuse; 2013 [cited 2015 Feb 12].
Available from: http://www.ccsa.ca/Resource%20Library/2012-Canada- Low-Risk-Alcohol-Drinking-Guidelines-Brochure-en.pdf.
15. Ministry of Health and Welfare. National health plan 2020 [Internet]. Sejong:
Ministry of Health and Welfare; 2011 [cited 2015 Feb 12]. Available from:
http://www.mindbank.info/item/4070.
16. Miranda PJ, DeFronzo RA, Califf RM, Guyton JR. Metabolic syndrome:
definition, pathophysiology, and mechanisms. Am Heart J 2005;149:33-45.
17. National Tax Service. Statistical yearbook of national tax, all relevant years [Internet]. Sejong: National Tax Service; 1985, 1995, 2000, 2005 [cited 2015 Feb 12]. Available from: http://stats.nts.go.kr/.
18. Chun S. The social meaning of alcohol consumption in Korea. J Korean Dia- betes 2012;13:57-60.
19. World Health Organization. Global status report on alcohol and health 2014 [Internet]. Geneva: World Health Organization; 2014 [cited 2015 Feb 12].
Available from: http://www.who.int/substance_abuse/publications/global_
alcohol_report/en/.
20. Ministry of Health and Welfare. Korea health statistics, 2005: Korea National Health and Nutrition Examination Survey (KNHANES III) 2005 [Internet].
Cheongju: Korea Centers for Disease Control and Prevention; 2005 [cited 2015 Feb 12]. Available from: http://knhanes.cdc.go.kr.
21. Klatsky AL, Friedman GD, Siegelaub AB, Gerard MJ. Alcohol consumption and blood pressure Kaiser-Permanente Multiphasic Health Examination data. N Engl J Med 1977;296:1194-200.
22. Ryu JY, Kim DH. Gender differences in the relationship between alcohol use behaviors and metabolic syndrome: Korean National Health and Nutrition Examination Survey (KNHANES) V 2010. Korean J Health Educ Promot 2013;30:83-93.
23. Koppes LL, Dekker JM, Hendriks HF, Bouter LM, Heine RJ. Moderate alco- hol consumption lowers the risk of type 2 diabetes: a meta-analysis of pro- spective observational studies. Diabetes Care 2005;28:719-25.
24. Rimm EB, Williams P, Fosher K, Criqui M, Stampfer MJ. Moderate alcohol intake and lower risk of coronary heart disease: meta-analysis of effects on lipids and haemostatic factors. BMJ 1999;319:1523-8.
25. Wakabayashi I. Cross-sectional relationship between alcohol consumption and prevalence of metabolic syndrome in Japanese men and women. J Ath- eroscler Thromb 2010;17:695-704.
26. Loucks EB, Magnusson KT, Cook S, Rehkopf DH, Ford ES, Berkman LF. So- cioeconomic position and the metabolic syndrome in early, middle, and late life: evidence from NHANES 1999-2002. Ann Epidemiol 2007;17:782-90.
27. Park MJ, Yun KE, Lee GE, Cho HJ, Park HS. A cross-sectional study of socio- economic status and the metabolic syndrome in Korean adults. Ann Epide- miol 2007;17:320-6.