Received March 4, 2013; Revised March 18, 2013, Accepted March 19, 2013 Corresponding author: Sungtae Koo
Divison of Meridian and Structural Medicine, School of Korean Medicine, Pusan National University, Beomeo-ri, Mulgeum-eup, Yangsan 626-870, Korea Tel: +82-51-510-8474, Fax: +82-51-510-8439, E-mail: [email protected]
This research was supported by Basic Science Research Program through the National Research Foundation of Korea(NRF) funded by the Ministry of Education, Science and Technology(2012R1A1A1043909).
CCThis is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License(http://creativecommons.org/licenses/ by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Repetitive Electroacupuncture Alleviate Neuropathic Pain in Association with Suppressing Activation of
Spinal Glial Cells
Heun Joo Lee, Bo Eun Jeong, Da Eun Song, Min Young Park, Sungtae Koo
Division of Meridian and Structural Medicine, School of Korean Medicine, Pusan National University
반복적인 전침 처치의 척수 교세포 활성 억제를 통한 신경병증성 통증 억제 효과
이흔주ㆍ정보은ㆍ송다은ㆍ박민영ㆍ구성태
부산대학교 한의학전문대학원 경락구조의학부
Objectives : Effects of repetitive electroacupuncture(EA) on the pain behavior and activation of spinal glial cells were examined in the rat model of neuropathic pain. Methods : Twenty one adult male Sprague-Dawley rats were randomly assigned into 3 groups(control group, SP6 group, ST36+GB34 group). Neuropathic pain was induced by tight ligation of L5 spinal nerve.
Mechanical and thermal hypersensitivity of hind paw were tested. Immunohistochemistry was performed in spinal cord L5/6 of all groups. EA was treated once in a day from the 5th day after surgery. Results : EA treatments applied to ST36 and GB34 reduced significantly both of mechanical and thermal hypersensitivity after 3 times of treatment throughout the experiments. In the SP6 group, the analgesic effect was also shown after 7 times of treatment. Immunohistochemistry demonstrated inhibition of microglia and astrocyte activation in the spinal cord L5/6 dorsal horn in the ST36+GB34 group. Conclusions : The present results suggest that repetitive EA exert strong analgesic effect on neuropathic pain. These analgesic effects in neuropathic pain are associated with suppressing the activation of microglia and astrocyte.
Key words : neuropathic pain, electroacupuncture, spinal nerve ligation, glial activation
Introduction
Currently, most of the estimates suggest that neuropathic pain may affect about 3% of the population1-3). In addition pharmacological treatments for the neuropathic pain gene-
rally use some combination of drugs such as opioids, non- steroidal anti-inflammatory drugs(NSAIDs)/analgesics. But various drugs provide 30∼50% reduction in pain in app- roximately 50% of patients. Unfortunately there is a diversity of side effects associated with drugs. The treatment of neu-
ropathic pain need to efforts to develop additional thera- peutic means4-6). Neuropathic pain is difficult to treat, partly due to our deficient understanding of its complex mecha- nisms7). It is characterized by spontaneous pain, hypersen- sitivity(a pain as a consequence of a stimulus which does not normally cause pain) and hyperalgesia(an elevated response to a normally painful stimulus). The mechanisms are complex and appear to cover both central and peripheral components of the nervous system8). Acupuncture analgesia for this pain condition has been studied about serious neuropathic pain9) such as diabetic neuropathy in patients10) and hyperalgesia in a neuropathic rat model11).
Acupuncture is a significant part of health care in Asian culture that can be traced back almost 3,000 years. Specially, electrical stimulation to specific acupuncture points help to recover patients to good health12). Recently, studies have expressed that EA alleviates the behavioral symptoms of hypersensitivity13,14) and hyperalgesia5,15,16) associated with neuropathic pain. It is well known that the EA analgesia are affected by descending pain inhibitory systems17,18), which mostly involve spinal opioid, serotonergic, adrenergic, dopa- minergic, and cholinergic receptors19-21).
Microglia and astrocytes correlate with normal and abnor- mal processes of the central nervous system(CNS)22-25). There are positive evidence that microglia and astrocytes of CNS involve in inducement and maintenance of neuropathic pain26-31). Hence, suppression of activation of microglia and astrocytes is being watched with interests in these days. In the recent study, the repeated EA analgesia on mechanical and warm allodynia in a rat tail model of neuropathic pain which was investigated the clinical efficacy of EA as a long- term therapy, and also examined glial activation in the spinal cord to verify whether EA suppresses spinal glial activation32). In the present study, we examined the effect of repetitive EA treatment on neuropathic pain in spinal nerve ligated model and the suppressive effect of repetitive EA treatment on the spinal glial activation in an early phase of neuropathic pain.
Materials and Methods
1. Experimental animals
Experiments were performed on young adult male Spra- gue-Dawley rats(200∼250 g, Hyochang Science, Daegu, Korea). Animals were housed in groups of two in plastic cages with soft bedding and were provided free access to food and water under a 12/12 hour reversed light-dark cycle(dark cycle: 8:00 A.M.∼8:00 P.M.). All animals were ac- climated for 7 days before the experiment began. All ex- perimental procedures were carried out in accordance with the Animals(Scientific Procedures) Act 2008(Korea) and all complied with the recommendations of the National Institute of Health’s Guide for the Care and Use of Laboratory Animals, and efforts were made to minimize animal suffering and to reduce the number of animals used in this study. The study was also approved by the Ethics Committee on Animal Research at Pusan National University(PNU-2012-0090).
2. Experimental procedures
In order to assess the effects of EA on neuropathic pain, we selected similar clinical situation. The rats were randomly divided into three groups: the spinal nerve ligated control group, group of EA applied to the SP6 point(SP6 group), group of EA applied to both of ST36 and GB34 points(ST36+
GB34 group). After baseline measurement tests on day0, the animals received neuropathic surgery and were monitored on days 2 by neuropathic surgery. From day 5, EA was given every day followed by mechanical allodynia and thermal hyperalgesia test at 2 h later of EA termination. In each group, L5-6 spinal cord of the rats was removed to analyze with immunohistochemistry on days 5 and 13.
3. Neuropathic surgery(spinal nerve ligation, SNL) Rats were anesthetized with isoflurane(3% induction, 2%
maintenance) in a mixed N2O/O2, then the L5 spinal nerve was tightly ligated as described before(Kim and Chung, 1992).
Briefly, a midline skin incision was made on the back at the lower lumbar region, the paraspinal muscles were retracted, and the left transverse process of the L6 vertebra was
removed under the dissection microscope. The left L5 spinal nerve was identified and gently separated from the adjacent L4 spinal nerve; it was then tightly ligated using 6-0 silk thread. The wound was cleaned with saline, closed with wound clips, and rats were returned to their cage after recovering from anesthesia.
4. Electroacupuncture(EA)
Under gaseous anesthesia(3% to induce and 1.5% to main- tain in a mixed N2O/O2), EA was applied by stimulating acupuncture points with electrical current through a pair of bipolar stimulating electrodes, which were modified acu- puncture needles. A stainless steel acupuncture needle(size:
0.25 mm in diameter and 40 mm in length) were mounted on a holder. The needle was inserted into a specific point at a depth of 5 mm and electrical stimulation was applied by a Pulsemaster Multi-channel Stimulator SYS-A300(World Precision Instruments, Inc., Berlin, Germany). Pulses repeated at a rate of 2 Hz were delivered at an intensity of 5 times of the muscle twitch threshold(muscle twitch threshold was usually around 200μA). The total duration of EA stimulation was 30 minutes. Immediately after the termination of EA, anesthesia was discontinued and the rats usually resumed full activity within 5∼10 minutes.
EA was applied into three different points on ipsilateral side(left) of the hind limb, which was equivalent to specific human acupuncture points. The first point was the Sa- meumgyo point which was designated as the SP6 point by the World Health Organization(WHO)33). The SP6 point is located on the medial aspect of the leg, posterior to the medial border of the tibia, 3/13 the distance from the pro- minence of the medial malleolus to the depression of inferior to the medial epicondyle of the tibia.34) The second point was the Joksamli point(ST36). The ST36 point is located at the anterior aspect of the leg, lateral to the tibial tubercle on the midway of anterior tibialis muscle34). The third point used was the Yangneungcheon point or the GB34 point by WHO nomenclature. The GB34 point is located on the fibular aspect of the leg, in the depression anterior and distal to the head of the fibula34). In the SP6 group, one set of two needles
were inserted with a 1-mm separation between the tips. In the ST36+GB34 group, one needle was inserted for each ST36 and GB34 point. Therefore, two needles were inserted in both groups.
5. Behavioral tests
Mechanical allodynia was assessed using a Dynamic Plantar Anesthesiometer(Ugo Basile, Italy) by measuring the latency to withdraw the hind paw from a graded force applied to the plantar surface of the paws using a Von Frey filament.
The cutoff force was set at 50 g. Following acclimatization after cessation of exploratory behavior, the operator placed the touch stimulator unit under the animal’s paw, using the adjustable angled mirror to position the filament below the target area of the paw. After pressing the “start” key, an electrodynamic actuator of proprietary design lifted a straight metal filament, which touched the plantar surface and began to exert an increasing upward force at a preset rate of ap- plication until a stop signal(when the animal removed the paw) was attained. The paw withdrawal threshold was numerically shown in grams on the digital screen.
Thermal hyperalgesia was assessed by the method of Hargreaves et al.(1988) by measuring the latency to with- draw the hind paw from a focused beam of radiant heat (thermal intensity: infrared 3.0) applied to the plantar surface, using a commercial apparatus(Ugo Basile, Varese, Italy). The cutoff time was set at 30 s. To measure rat hind paw thermal thresholds, each rat was placed in a clear plastic com- partment of a three-compartment box with a glass floor and allowed to acclimatize for 10∼20 min. A paw-flick response was elicited by a high intensity infrared beam focused on the plantar surface of left and right paws(Ugo Basile, Italy). The time that elapsed before reflex removal of the hind paw from the beam(paw withdrawal latency, PWL) was monitored.
PWL was defined as the mean of three measurements at interstimulus interval of one minute. Rats were trained for at least three days in order for the variability between these trials to be approximately 0.5 s. Both ipsilateral and con- tralateral paw thresholds were measured to monitor develop- ment of thermal hypersensitivity in SNL rats.
Fig. 1. Effect of repetitive EA on the mechanical allodynia and thermal hyperalgesia. EA treatment started on the 5th day after surgery.
The effect of EA applied to ST36 and GB34 point(ST36+GB34) and applied to SP6 point(SP6) on mechanical allodynia(A) and on thermal hyperalgesia(B) is shown. Repetitive EA produce significantly increased mechanical and thermal threshold com- pared with control group(CON). Each group represents the mean of 7 rats, and the vertical lines indicate the SEM *p<0.05(one way ANOVA followed by Dunnett’s test).
6. Immunohistochemistry
The L5-6 segments of the spinal cords were fixed in 4%
paraformaldehyde and immersed in 30% gradient sucrose for 48h at 4oC for cryoprotection. Frozen tissue were sectioned at 20μm-thick on a freezing microtome(CM3050S, Leica biocyctems, Wetzlar, Germany). All the sections were blocked with CAS-block(Invitrogen-Molecular Probes, Inc., Camo- rillo, CA, USA) for 9 mins at room temperature(RT) and incubated with mouse anti-glial fibrillary acidic protein (GFAP) at a dilution 1:400 or mouse anti-Iba-1 at a dilution 1:100 following primary antibodies overnight in PBS at 4oC.
After washed with PBS containing Tween-20 (PBST), the sections were incubated with the secondary antibody, anti- mouse IgG-FITC(Vector Laboratories, Inc. Burlingame, CA) for 2 h at RT and then washed with PBST. Immunoreactivity was visualized by incubating the sections in a soulation consisting of 0.05% 3,3-diaminobenzidine(DAB) for appro- ximately 1 min 40 sec.
7. Data analysis
The data of results are presented as mean±SEM. Statis- tical significance of differences between groups was per- formed by one-way ANOVA followed by Dunnett’s test using Systat Sigmaplot Version 12.2. p values(p<0.05) were con- sidered statistically significant.
Results
1. Repetitive EA reduced hypersensitivity
After SNL surgery, all of the rats were developed with hypersensitivity. Noticeably reduced group of mechanical hypersensitivity was ST36+GB34 group when compared SP6 and the control group(days 7∼13, n=7, *p<0.05)(Fig. 1A).
Significant reduction of hypersensitivity was found after 3 times of treatment. The mechanical hypersensitivity of SP6 group was reduced when compared to the control group after 7 times of treatment(Fig. 1A). In the thermal hyper- sensitivity test, Repetitive EA treatment of ST36 and GB34 points also showed significant increase of withdrawal latency
after 4 times of treatment(days 8∼13, n=7, *p<0.05)(Fig. 1B).
In the SP6 group, the hypersensitivity was reduced compared to the control group after 8 times of treatment(Fig. 1B).
2. Repetitive EA suppressed activation of glial cells After the last treatment on day 13, the immunohisto- chemistry was performed to determine whether EA inhibit the activation of glial cell. A total of 12 L4 to L5 spinal cord sections from 3 per group and 3 rats on 5 days from control group were obtained. Immunohistochemistry analysis of glial
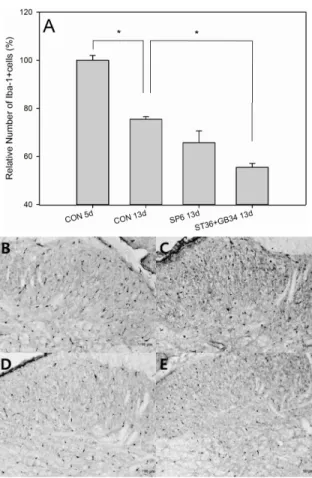
Fig. 2. Effect of repetitive EA on microglial activation.
Immunohistochemical analysis of L5/6 ipsilateral spinal cord was performed on day 5 and day 13 after SNL surgery(n=3). Repetitive EA significantly suppress microglial activation(A). Data are presented as mean±SEM of relative number of Iba-1 positive cells. *Indicates values significantly different(p<0.05) from the value of 13 day of control group by the one-way ANOVA followed by the Dunnett’s post-hoc test. (B) 5th day after SNL (C) 13th day after SNL (D) 13th day after SNL with SP6 treatment (E) 13th day after SNL with ST36 and GB34 treatment.
Fig. 3. Effect of repetitive EA on astrocytic activation.
Immunohistochemical analysis of L5/6 ipsilateral spinal cord was performed on day 5 and day 13 after SNL surgery(n=3). Repetitive EA significantly suppress astrocytic activation(A). Data are presented as mean ± SEM of relative number of GFAP positive cells. *Indicates values significantly different(p<0.05) from the value of 13 day of control group by the one-way ANOVA followed by the Dunnett’s post-hoc test. (B) 5th day after SNL (C) 13th day after SNL (D) 13th day after SNL with SP6 treatment (E) 13th day after SNL with ST36 and GB34 treatment.
cell activation in L5-L6 ipsilateral spinal cord was performed.
Activation of microglial cells and astrocytic cells were analy- zed in each group. On the 5 days after SNL surgery, microglial cells(Iba-1 positive cells) when compared ST36+GB34 came best. On the 13 days after SNL surgery, astrocytic cells(GFAP positive cells) were reduced noticeably in ST36+ GB34 group.
Iba-1 and GFAP positive cells were measured in the laminae I-IV. There were statistically significant differences in the number of Iba-1 positive cells among the groups(CON 13d vs ST36+GB34 13d, p<0.05)(Fig. 2A). There were also statistically significant differences in the number of GFAP positive cells among the groups(CON 13d vs SP6 13d, p<
0.05, CON 13d vs ST36+GB34 13d, p<0.05)(Fig. 3A).
Discussion
1. Repetitive EA reduced hypersensitivity
In the present study, we chose two acupoint groups for EA. One is combination of ST36 and GB34. The other is SP6.
We intended to argue for the specificity of these acupoints for the treatment of hypersensitivity result from neuropathic pain. The SP6 was known to be less effective when used alone in the treatment of neuropathic pain model35). The
analgesic effect of EA treatment which was performed twice a day quite a long time was reported32). However, in the present study, we showed a relatively early effect of daily EA treatment. Although the current study showed an analgesic effect in the rat model of neuropathic pain, more studies are required to investigate the underlying mechanism of repe- titive EA.
2. Repetitive EA inhibited microglial and astrocyte activation
Astrocytes play a role in the early stage of acute pain and maintenance of chronic pain. Microglia responses precede astrocytes activation and are involved in initiation of chronic pain36,37). Astrocytes start to increase between 3 to 7 days after SNL38). We performed the EA on 5 days after SNL when microglia and astrocytes will be high level in L5/6 dorsal horn. In the immunohistochemistry analysis of L5/6 spinal cord dorsal horns, activation of microglia and astrocyte were decreased especially in the ST36+GB34 group compared EA untreated group(Fig. 2A, Fig. 3A). It is well known that microglia and astrocytes activation are increased in the spinal cord under pain conditions. In addition, microglia and astro- cytes synthesize multiple inflammatory mediators, and may rev up each other39-41). Astrocytes are sited in extremely close contact with neurons, and are sensitive to change in neuronal environment. Microglial responses typically precede astrocyte activation37). Consequently, EA induced inhibition of mecha- nical and thermal hypersensitivity parallel glial activation.
The results are in agreement with previous study that sup- pression of microglia and astrocytes activation reduced mechanical and thermal allodynia4,32,42,43)
.
Conclusion
In the present study, we showed that repetitive EA re- duced hypersensitivity result from spinal nerve ligation;
neuropathic pain model. Repetitive EA alleviated mechanical allodynia and thermal hyperalgesia and suppressed glial activation in a point specific manner.
Acknowledgements
This research was supported by Basic Science Research Program through the National Research Foundation of Korea(NRF) funded by the Ministry of Education, Science and Technology(2012R1A1A1043909).
References
1. Foley KM. Opioids and chronic neuropathic pain. N Engl J Med.
2003 ; 348 : 1279-81.
2. Verma S, Estanislao L, Simpson D. HIV-associated neuropathic pain: epidemiology, pathophysiology and management. CNS Drugs. 2005 ; 19 : 325-34.
3. Werhagen L, Budh CN, Hultling C, Molander C. Neuropathic pain after traumatic spinal cord injury--relations to gender, spinal level, completeness, and age at the time of injury. Spinal Cord. 2004 ; 42 : 665-73.
4. Tawfik VL, Nutile-McMenemy N, Lacroix-Fralish ML, Deleo JA.
Efficacy of propentofylline, a glial modulating agent, on exist- ing mechanical allodynia following peripheral nerve injury.
Brain Behav Immun. 2007 ; 21 : 238-46.
5. Kim JH, Min BI, Na HS, Park DS. Relieving effects of electro- acupuncture on mechanical allodynia in neuropathic pain model of inferior caudal trunk injury in rat: mediation by spinal opioid receptors. Brain Res. 2004 ; 998 : 230-6.
6. Butera JA. Current and emerging targets to treat neuropathic pain. J Med Chem. 2007; 50: 2543-6.
7. Sinatra R. Role of COX-2 inhibitors in the evolution of acute pain management. J Pain Symptom Manage. 2002 ; 24 : S18-27.
8. Bridges D, Thompson SW, Rice AS. Mechanisms of neuropathic pain. Br J Anaesth. 2001 ; 87 : 12-26.
9. Filshie J. The non-drug treatment of neuralgic and neuropathic pain of malignancy. Cancer Surv. 1988 ; 7 : 161-93.
10. Goodnick PJ, Breakstone K, Wen XL, Kumar A. Acupuncture and neuropathy. Am J Psychiatry. 2000 ; 157 : 1342-3.
11. Omana I, Olvera V, Santos P, Calderon JL. Naloxone prevents reduction of pain responses evoked by acupuncture in neuro- pathic rats. Proc West Pharmacol Soc. 1994 ; 37 : 135-6.
12. Wang SM, Kain ZN, White P. Acupuncture analgesia: I. The sci- entific basis. Anesth Analg. 2008 ; 106 : 602-10.
13. Dong ZQ, Ma F, Xie H, Wang YQ, Wu GC. Down-regulation of GFRalpha-1 expression by antisense oligodeoxynucleotide at- tenuates electroacupuncture analgesia on heat hyperalgesia in a rat model of neuropathic pain. Brain Res Bull. 2006 ; 69 : 30-6.
14. Dai Y, Kondo E, Fukuoka T, Tokunaga A, Miki K, Noguchi K. The effect of electroacupuncture on pain behaviors and noxious stimulus-evoked Fos expression in a rat model of neuropathic pain. J Pain. 2001 ; 2 : 151-9.
15. Hwang BG, Min BI, Kim JH, Na HS, Park DS. Effects of electro- acupuncture on the mechanical allodynia in the rat model of neuropathic pain. Neurosci Lett. 2002 ; 320 : 49-52.
16. Huang C, Li HT, Shi YS, Han JS, Wan Y. Ketamine potentiates the effect of electroacupuncture on mechanical allodynia in a rat model of neuropathic pain. Neurosci Lett. 2004 ; 368 : 327-31.
17. Takeshige C, Sato T, Mera T, Hisamitsu T, Fang J. Descending pain inhibitory system involved in acupuncture analgesia. Brain Res Bull. 1992 ; 29 : 617-34.
18. Li A, Wang Y, Xin J, Lao L, Ren K, Berman BM, et al.
Electroacupuncture suppresses hyperalgesia and spinal Fos ex- pression by activating the descending inhibitory system. Brain Res. 2007 ; 1186 : 171-9.
19. Eisenach JC. Muscarinic-mediated analgesia. Life Sci. 1999 ; 64 : 549-54.
20. Millan MJ. Descending control of pain. Prog Neurobiol. 2002 ; 66 : 355-474.
21. Gao X, Xin BM, Zhu CB, Wu GC, Xu SF. Effect of intrathecal in- jection of dopamine receptor agonists/antagonists on pain and acupuncture analgesia in rats. Sheng Li Xue Bao. 1998 ; 50 : 43-8.
22. Miller G. Neuroscience. The dark side of glia. Science. 2005 ; 308 : 778-81.
23. Markiewicz I, Lukomska B. The role of astrocytes in the physiol- ogy and pathology of the central nervous system. Acta Neurobiol Exp(Wars). 2006 ; 66 : 343-58.
24. Allen NJ, Barres BA. Neuroscience: Glia-more than just brain glue. Nature. 2009 ; 457 : 675-7.
25. Benarroch EE. Neuron-astrocyte interactions: partnership for normal function and disease in the central nervous system.
Mayo Clin Proc. 2005 ; 80 : 1326-38.
26. Cao H, Zhang YQ. Spinal glial activation contributes to patho- logical pain states. Neurosci Biobehav Rev. 2008 ; 32 : 972-83.
27. Lee S, Zhao YQ, Ribeiro-da-Silva A, Zhang J. Distinctive re- sponse of CNS glial cells in oro-facial pain associated with in- jury, infection and inflammation. Mol Pain. 2010 ; 6 : 79.
28. Zhuang ZY, Wen YR, Zhang DR, Borsello T, Bonny C, Strichartz GR, et al. A peptide c-Jun N-terminal kinase(JNK) inhibitor blocks mechanical allodynia after spinal nerve ligation: re- spective roles of JNK activation in primary sensory neurons and spinal astrocytes for neuropathic pain development and maintenance. J Neurosci. 2006 ; 26 : 3551-60.
29. Watkins LR, Maier SF. Beyond neurons: evidence that immune and glial cells contribute to pathological pain states. Physiol Rev. 2002 ; 82 : 981-1011.
30. Suter MR, Wen YR, Decosterd I, Ji RR. Do glial cells control pain?
Neuron Glia Biol. 2007 ; 3 : 255-68.
31. Scholz J, Woolf CJ. The neuropathic pain triad: neurons, im- mune cells and glia. Nat Neurosci. 2007 ; 10 : 1361-8.
32. Gim GT, Lee JH, Park E, Sung YH, Kim CJ, Hwang WW, et al.
Electroacupuncture attenuates mechanical and warm allodynia through suppression of spinal glial activation in a rat model of neuropathic pain. Brain Res Bull. 2011 ; 86 : 403-11.
33. World Health Organization. Standard acupuncture nomen- clature. Manila: World Health Organization, Regional Office for the Western Pacific. 1993.
34. Koo ST, Kim SK, Kim EH, Kim JH, Youn DH, Lee BH, et al.
Acupuncture point locations for experimental animal studies in rats and mice. Korean Journal of Acupuncture. 2010 ; 27 : 75-86.
35. Cidral-Filho FJ, da Silva MD, More AO, Cordova MM, Werner MF, Santos AR. Manual acupuncture inhibits mechanical hyper- sensitivity induced by spinal nerve ligation in rats. Neuro- science. 2011 ; 193 : 370-6.
36. Romero-Sandoval A, Chai N, Nutile-McMenemy N, Deleo JA. A comparison of spinal Iba1 and GFAP expression in rodent mod- els of acute and chronic pain. Brain Res. 2008 ; 1219 : 116-26.
37. Kreutzberg GW. Microglia: a sensor for pathological events in the CNS. Trends Neurosci. 1996 ; 19 : 312-8.
38. Liu FY, Sun YN, Wang FT, Li Q, Su L, Zhao ZF, et al. Activation of
satellite glial cells in lumbar dorsal root ganglia contributes to neuropathic pain after spinal nerve ligation. Brain Res. 2012 ; 1427 : 65-77.
39. Watkins LR, Maier SF. Glia: a novel drug discovery target for clinical pain. Nat Rev Drug Discov. 2003 ; 2 : 973-85.
40. Watkins LR, Milligan ED, Maier SF. Glial activation: a driving force for pathological pain. Trends Neurosci. 2001 ; 24 : 450-5.
41. DeLeo JA, Yezierski RP. The role of neuroinflammation and neu- roimmune activation in persistent pain. Pain. 2001 ; 90 : 1-6.
42. Mika J, Osikowicz M, Rojewska E, Korostynski M, Wawrzczak- Bargiela A, Przewlocki R, et al. Differential activation of spinal microglial and astroglial cells in a mouse model of peripheral neuropathic pain. Eur J Pharmacol. 2009 ; 623 : 65-72.
43. Zhuang ZY, Gerner P, Woolf CJ, Ji RR. ERK is sequentially acti- vated in neurons, microglia, and astrocytes by spinal nerve liga- tion and contributes to mechanical allodynia in this neuro- pathic pain model. Pain. 2005 ; 114 : 149-59.
국문초록
목적 : 신경병증성 통증 쥐 모델에서 통증 행동과 척수 교세포의 활성화에 대한 반복적 전침의 영향을 실험하였다. 방법 : 21마리 Sprague-Dawley 성체 수컷 쥐를 무작위적으로 대조군, SP6 군, ST36+GB34 군으로 나누었다. 신경병증성 통증은 L5 척수신경을 단단하게 묶는 것으로 유도하였다. 신경병증성 통증이 유도된 뒷발에 기계적 및 열적 민감도를 조사하였다. 모든 군의 L5/6 척수에서 면역조직화학염색 법을 수행하였다. 수술 이후 5일째부터 하루에 한번씩 전침을 시행하였다. 결과 : 족삼리(ST36)와 양릉천(GB34)에 적용된 전침은 3번의 처치 이후 실험기간 내내 기계적 및 열적 민감도를 모두 감소시켰다. 삼음교(SP6) 군에서는 진통 효과가 7번의 처치 이후 감소됨을 보였다. 면역조 직화학염색법은 ST36+GB34 군에서 L5/6 척수 후각에서 교세포와 성상세포의 활성화가 억제됨을 보였다. 결론 : 이 결과는 반복적인 전침은 신경병증성 통증에 강한 진통 효과를 발휘 하는 것을 시사한다. 신경병증성 통증에서 이 진통 효과는 교세포와 성상세포의 활성화를 억제하는 것과 관련이 있다.