Korean J Gastroenterol Vol. 70 No. 3, 150-153 https://doi.org/10.4166/kjg.2017.70.3.150 pISSN 1598-9992 eISSN 2233-6869
IMAGE OF THE MONTH
Korean J Gastroenterol, Vol. 70 No. 3, September 2017 www.kjg.or.kr
혈관성 중심반흔을 보인 간세포암
이예다운, 남경한
1, 정보현
2, 윤정희, 김승호
인제대학교 의과대학 해운대백병원 영상의학과, 병리과1, 외과2
Hepatocellular Carcinoma with Vascular Central Scar
Yedaun Lee, Kyung Han Nam1, Bo-Hyun Jung2, Jung-Hee Yoon and Seung Ho Kim
Departments of Radiology, Pathology1 and Surgery2, Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2017. Korean Society of Gastroenterology.
교신저자: 이예다운, 48108, 부산시 해운대구 해운대로 875, 인제대학교 의과대학 해운대백병원 영상의학과
Correspondence to: Yedaun Lee, Department of Radiology, Haeundae Paik Hospital, Inje University College of Medicine, 875 Haeundae-ro, Haeundae-gu, Busan 48108, Korea. Tel: +82-51-797-0356, Fax: +82-51-797-0379, E-mail: chosai81@gmail.com
Financial support: None. Conflict of interest: None.
증례: 65세 남자 환자가 외부 검사에서 발견된 간종괴를 주소 로 내원하였다. 환자는 만성 B형간염 및 간경변증으로 정기적으로 추적 관찰 중이었고, 고혈압으로 Norvasc를 복용하는 중이었다.
내원 당시 활력 징후는 혈압 120/80 mmHg, 맥박수 71회/분, 체온 37oC로 측정되었다. 복부 압통이나 촉지되는 종괴 등의 이상 소견은 없었다. 말초혈액 검사에서 백혈구 6,170/μL, 혈색 소 15.0 g/dL, 혈소판 154,000/μL로 측정되었고, 생화학 검사에서 aspartate aminotransferase (AST)/alanine aminotransferase (ALT) 25/20 IU/L, 총 빌리루빈 0.6 mg/dL, 알부민 4.1 g/dL 로 측정되었다. 바이러스 간염 표지자는 hepatitis B surface antigen (HBsAg) 양성, antibody to hepatitis B core anti- gen (anti-HBc) 양성, antibody to hepatitis B surface an- tigen (anti-HBs) 음성, antibody to hepatitis C virus (anti HCV) 음성을 보였다. 종양표지자 검사상 alpha- fetoprotein (AFP) 22.5 ng/mL, protein induced by vitamin K absence or antagonist-II (PIVKA-II) 55 mAU/mL로 증가되어 있었다.
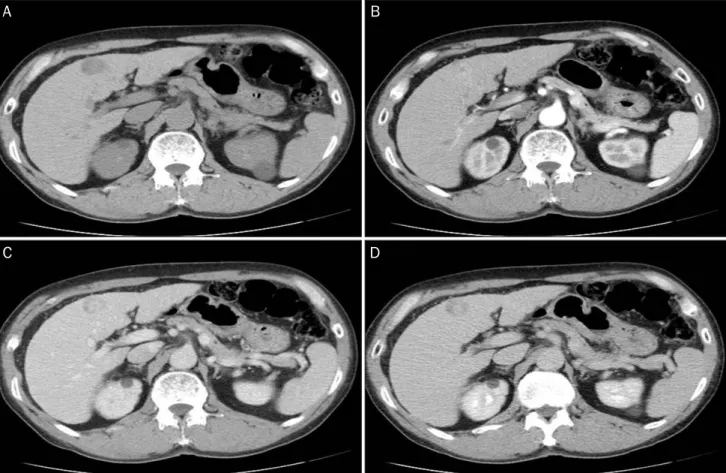
외부에서 시행한 간 역동성 전산화단층촬영에서 간 좌엽 제 4분절에 약 2.5 cm 크기의 동맥기에서 조영증강을 보이고, 문 맥기 조영 감소를 보이는 원형의 간종괴가 관찰되었다(Fig. 1).
동맥기에서 종괴의 중심 부분에 저음영을 보이는 중심반흔으 로 생각되는 부위가 보이고, 이 부위는 문맥기와 지연기에는 조영증강이 되는 양상이었다. 간은 간표면의 결절성 변화를 보이는 간경변을 보이고, 문맥혈전이나 커진 림프절은 보이지
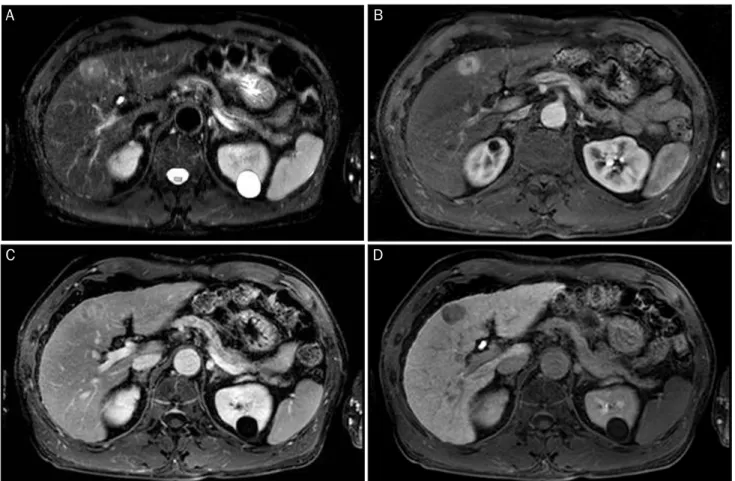
않았다. 보다 정확한 진단을 위해 시행한 자기공명영상에서 종괴는 T1강조영상에서 간실질보다 저신호강도를 보였고, T2 강조영상에서는 약간 고신호강도를 보였다. 중심반흔으로 생 각되는 부위는 T2강조영상에서 고신호강도를 보였다. 역동학 적 조영증강영상의 동맥기 영상에서 종괴는 경계가 비교적 분 명하면서 조개껍데기 모양의 경계를 보였고(Fig. 2), 문맥기, 지 연기로 가면서 저신호강도를 보였으며, 간담도기 영상에서 저신 호강도를 보였다. 중심반흔으로 생각되는 부위는 동맥기 영상에 서 저신호강도를 보였고, 지연기에서 조영증강을 보였다.
환자는 간세포암 진단하에 간 좌엽 절제술을 시행하였다.
조직학적으로 종괴는 중등분화 간세포암이었고, 중심반흔은 섬유조직의 간질 내에 많은 혈관들이 관찰되어 혈관성 반흔을 보이는 간세포암으로 진단되었다(Fig. 3).
진단: 혈관성 중심반흔을 보인 간세포암
본 증례는 간경변이 있는 환자에서 1 cm 이상의 크기, 동 맥기 영상에서 조영증강을 보이고, 문맥기의 씻김을 보여 영 상의학적 진단 기준에 적합한 간세포암이나, 조개껍데기 양상 의 변연을 보이면서 T2강조영상에서 고신호강도를 보이는 중 심반흔을 동반하였던 점에서 국소결절성과증식과 비슷한 영 상의학적 소견을 보여 소개하였다.
중심반흔은 국소결절성과증식, 섬유층판 간세포암, 거대 혈 관종 등의 병변에서 주로 동반된다.1중심반흔은 조직학적으
Lee Y, et al. Hepatocellular Carcinoma with Vascular Central Scar
151
Vol. 70 No. 3, September 2017
Fig. 1. Liver dynamic computed tomography (CT). CT images show an enhancing nodule in segment IV. The nodule shows low attenuation in precontrast image (A), enhancement in arterial phase (B) and wash out in portal and delayed phase (C, D). The central scar shows low attenuation in arterial phase and enhancement in delayed phase.
로 염증성, 혈관성 혹은 교원성 조직요소의 충만도에 따라 세 단계로 분류된다. 염증성 반흔은 주로 반흔 형성의 초기 단계 에 발생하며, 해면상 혈관종에서 주로 나타난다. 혈관성 반흔 은 풍부한 혈관들을 보이는 것이 특징이며, 주로 국소결절성 과형성에서 혈관 기형이나 혈관 손상의 결과로 나타난다. 염 증성과 혈관성 반흔은 둘 다 T1강조영상에서 저신호강도, T2 강조영상에서 고신호강도를 보인다. 반면 교원성 반흔은 반흔 형성의 마지막 단계로 간세포암에서 주로 발견되며, T2강조 영상에서 저신호강도를 보인다.2
간세포암에서 중심반흔은 섬유층판 간세포암에서 주로 보 이는 소견으로 알려져 있고, 섬유층판 간세포암의 약 20-71%
에서 중심반흔이 동반되는 것으로 보고되어 있다.3-5섬유층판 간세포암의 중심반흔은 T1강조영상 및 T2강조영상에서 저신 호강도를 보이며, 중심반흔 내에 석회화를 잘 동반한다. 반면 국소결절성과증식에서의 중심반흔은 혈관성 반흔으로 T2강조 영상에서 고신호강도를 보인다는 점에서 감별점이 될 수 있다.6 고식적 간세포암에서도 중심반흔을 동반할 수 있으며, 한 보고에 따르면 총 1,043예의 간세포암 증례 중 3%가 중심반 흔을 가진 간세포암이었고, 이러한 중심반흔을 동반한 간세포
암은 단순 결절형 간세포암과 비교하였을 때 더 높은 생존율 을 보였다.7하지만 여기에서 소개된 간세포암들의 중심반흔 은 조직학적으로 섬유조직으로 이루어져 있었고, 이러한 점에 서 본 증례와는 다르다.
본 증례와 같이 혈관성 반흔을 가졌던 간세포암은 지금까 지 한 증례가 보고되어 있으며, 이 증례 역시 중심반흔은 T2 강조영상에서 고신호강도를 보이고, 조직학적으로 많은 다양 한 크기의 혈관을 포함하고 있었다.8 이러한 혈관성 반흔은 국소결절성과증식으로 오인하게 만드는 소견이 될 수 있다.
국소결절성과증식은 간경변이 없는 환자에서 생기는 양성 종양이다. 그러나 간경변이 있는 환자에서도 국소결절성과증 식과 비슷한 병리 소견을 보이는 국소결절성과증식양결절이 생길 수 있고, 특히 알코올성 간경변증 환자에서 잘 동반된 다.9전형적으로 국소결정성과증식 및 국소결절성과증식양결 절은 역동학적 조영증강영상에서 동맥기에는 중심반흔을 제 외하고 균일한 조영증강을 보이고, 문맥기와 지연기에는 등음 영 또는 약간의 고음영을 보인다. 중심반흔은 동맥기에는 저 음영으로 보이고, 지연기로 가면 조영증강될 수 있다.10 그러 나 일부 국소결절성과증식 및 대부분의 국소결절성과증식양
C D
A B
152
이예다운 등. 혈관성 중심반흔을 보인 간세포암The Korean Journal of Gastroenterology
Fig. 2. Liver magnetic resonance images (MRI). (A) MRIs show a nodule with central scar showing high signal intensity on T2 weighted image.
(B, C) The nodule shows scalloped margin and homogenous enhancement on arterial phase (B), low signal intensity on hepatic phase (C).
The central scar shows low signal intensity on arterial phase and delayed enhancement on hepatic phase. (D) On hepatobiliary phase, the nodule shows low signal intensity.
Fig. 3. Pathologic findings of surgical specimen. (A) Gross appearance of the resected liver shows a well-defined, whitish-yellow mass with a central scar. (B) Microscopic finding of the tumor shows a central scar consisting of many thin-walled blood vessels within a fibrous stroma (H&E, ×40).
결절은 문맥기 및 지연기 영상에서 저음영을 보일 수 있다.11 Gadoxetic acid와 같은 간세포 특이 조영제를 이용한 자기공 명영상의 간담도기영상에서 주변 간조직에 비해 비슷하거나
혹은 더 높은 신호강도를 보이고, 중심반흔은 간담도기영상에 서 저신호강도로 보이며, 간혹 중심반흔의 저신호강도가 더 강조되어 보여 전체적으로 저신호강도를 보이는 것으로 오인
A B
A B
C D
Lee Y, et al. Hepatocellular Carcinoma with Vascular Central Scar
153
Vol. 70 No. 3, September 2017
될 수 있다.12-14 이렇게 국소결절성과증식 및 국소결절성과증 식양결절이 문맥기와 지연기에서의 저음영 및 간담도영상에 서의 저신호강도를 보이는 경우 간세포암과 감별이 어려울 수 있다.
본 증례와 같이 혈관성 반흔을 가지는 간세포암은 매우 드 물지만, 간혹 국소결절성과증식 및 국소결절성과증식양결절 과 혼동될 수 있어 주의가 필요할 것으로 생각된다.
REFERENCES
1. Kim T, Hori M, Onishi H. Liver masses with central or eccentric scar. Semin Ultrasound CT MR 2009;30:418-425.
2. Rummeny E, Weissleder R, Sironi S, et al. Central scars in primary liver tumors: MR features, specificity, and pathologic correlation.
Radiology 1989;171:323-326.
3. Blachar A, Federle MP, Ferris JV, et al. Radiologists’ performance in the diagnosis of liver tumors with central scars by using specif- ic CT criteria. Radiology 2002;223:532-539.
4. McLarney JK, Rucker PT, Bender GN, Goodman ZD, Kashitani N, Ros PR. Fibrolamellar carcinoma of the liver: radiologic-pathologic correlation. Radiographics 1999;19:453-471.
5. Ichikawa T, Federle MP, Grazioli L, Madariaga J, Nalesnik M, Marsh W. Fibrolamellar hepatocellular carcinoma: imaging and pathologic findings in 31 recent cases. Radiology 1999;213:
352-361.
6. Hussain SM, Terkivatan T, Zondervan PE, et al. Focal nodular hy- perplasia: findings at state-of-the-art MR imaging, US, CT, and pathologic analysis. Radiographics 2004;24:3-17; discussion
18-19.
7. Yamamoto M, Ariizumi S, Yoshitoshi K, Saito A, Nakano M, Takasaki K. Hepatocellular carcinoma with a central scar and a scalloped tumor margin resembling focal nodular hyperplasia in macroscopic appearance. J Surg Oncol 2006;94:587-591.
8. Yamauchi M, Asayama Y, Yoshimitsu K, et al. Hepatocellular car- cinoma with a prominent vascular scar in the center: MR imaging findings. Radiat Med 2006;24:467-470.
9. Quaglia A, Tibballs J, Grasso A, et al. Focal nodular hyper- plasia-like areas in cirrhosis. Histopathology 2003;42:14-21.
10. Kamel IR, Liapi E, Fishman EK. Focal nodular hyperplasia: lesion evaluation using 16-MDCT and 3D CT angiography. AJR Am J Roentgenol 2006;186:1587-1596.
11. Kobayashi S, Matsui O, Kamura T, et al. Imaging of benign hyper- vascular hypatocellular nodules in alcoholic liver cirrhosis: differ- entiation from hypervascular hepatocellular carcinomas. J Comput Assist Tomogr 2007;31:557-563.
12. Yoneda N, Matsui O, Kitao A, et al. Hepatocyte transporter ex- pression in FNH and FNH-like nodule: correlation with signal in- tensity on gadoxetic acid enhanced magnetic resonance images.
Jpn J Radiol 2012;30:499-508.
13. Fujiwara H, Sekine S, Onaya H, Shimada K, Mikata R, Arai Y.
Ring-like enhancement of focal nodular hyperplasia with hep- atobiliary-phase Gd-EOB-DTPA-enhanced magnetic resonance imaging: radiological-pathological correlation Jpn J Radiol 2011;
29:739-743.
14. Grazioli L, Bondioni MP, Heradome H, et al. Hepatocellular ad- enoma and focal nodular hyperplasia: value of gadoxetic acid-en- hanced MR imaging in differential diagnosis. Radiology 2012;
262:520-529.