O R IG IN A L A R T IC L E
KOREA J. ORTHOD. 1999. 2 9 (6 ) : 699-706
T h e skeletal cortical a nc ho ra ge
니sing tita n iu m microscrew implants
H y o S a n g P a r k 1)
A n ch o ra g e p la y s an im p o rta n t ro le in o rth o d o n tic tre a tm e n t. E ndosseous im p la n ts m a y be co n sid e re d adequate fir m anchorage. H o w e ve r, c lin ic ia n s ha ve h e s ita te d to use endosseous im p la n ts as o rth o d o n tic anchorage because o f lim ite d im p la n ta tio n space, h ig h co st, and lo n g w a itin g p e rio d b e fore o ss e o in te g ra tio n occurs.
R e ce n tly, som e c lin ic ia n s h ave trie d to use tita n iu m m in is c re w s and m ic ro s c re w s in tre a tm e n t due to th e ir m an y ad vantag es su ch as ease o f in s e rtio n and re m o v a l, lo w cost, im m e d ia te lo a d in g , and th e a b ility to place m ic ro s c re w s in a n y area o f a lv e o la r bone.
T h e a u th o r tre a te d a case w ith s k e le ta l c o rtic a l anchorage u s in g tita n iu m m ic ro s c re w im p la n ts . D u rin g s ix m o n th s o f o rth o d o n tic fo rc e a p p lic a tio n fro m s k e le ta l c o rtic a l anchorage, th e a u th o r co u ld g e t 4 m m b o d ily re tra c tio n and in tru s io n o f u p p e r a n te rio r te e th . T h e m o st o u ts ta n d in g re s u it w a s a 1.5 m m p o s te rio r re tra c tio n o f th e u p p e r p o s te rio r te e th . T h e tita n iu m m ic ro s c re w im p la n ts had rem a ine d fir m and sta b le th ro u g h o u t tre a tm e n t.
T he se re s u lts in d ic a te th a t s k e le ta l c o rtic a l anchorage m ig h t be a v e ry good o p tio n .
Key word : S k e le ta l c o rtic a l anchorage, T ita n iu m m ic ro s c re w im p la n ts
I
n o rth o d o n tic therapy, anchorage plays a c ru c ia l role. T here are tw o categories in discu ssin g anchorage: in tra o ra l and e xtra o ra l.In tra o ra l d e rive d anchorage is unstable, ne ce ssi- ta tin g appliances w h ic h can be com plicated, in e fn cie n t, and o fte n re q u ire th e e x tra c tio n o f dental u n its. Q n th e o th e r hand, e x tra o ra l appliances can be q u ite stable b u t depend on th e p a tie n t/s cooperation.
In o rd e r to p ro vid e acceptable anchorage fo r o rth o d o n tic appliances, endosseous im p la n ts have been suggested and used.12,14) B u t th e ir use fo r o rth o d o n tic anchorage has been lim ite d b y space, econom y, and tim e la g betw een im p la n ta tio n and orthodontic force application.
V D epartment of Orthodontics D entistry, College of M edicine, Keim yung University,
R e c e n tly , K a n o m i8' a n d C o s ta e t a l3) h a v e in tro d u c e d th e u s e o f tita n iu m m ic ro s c re w s as o rth o d o n tic a n c h o ra g e . T h e a d v a n ta g e s o f th e m ic ro s c re w s a re th a t th e y a re s m a ll e n o u g h to p la c e in a n y a re a o f a lv e o la r b o n e , e a se o f im p la n ta tio n a n d re m o v a l, lo w c o s t, a n d th e s h o rt in te r v a l b e tw e e n im p la n ta tio n a n d o rth o d o n tic fo rc e a p p lic a tio n .
H e re in , th e a u th o r p re s e n ts a ca se re p o rt o f tre a tm e n t w ith s k e le ta l c o rtic a l a n c h o ra g e u s in g tita n iu m m ic ro s c re w im p la n ts f o r r e tr a c tin g u p p e r a n te rio r te e th a n d d is c u s s e s th e c lin ic a l c o n s id e ra tio n s .
C A S E
T h e p a tie n t w a s a 1 2 -y e a r -o id b o y w h o s e c h ie f c o m p la in ts w e re u p p e r p ro tr u s io n a n d c ro w d in g .
Hyo Sang Park 대치교정지 29권 6호, 1999년
Fig. 1. Initial facia l photos, lateral cephalom etric radiograph, intraoral photos, and panoram ic radiograph.
1 . D i a g n o s i s
1) Extraoral findings
The patient had a straight profile. The lateral photo showed protrusion of upper and lower lips and curved mentolabial fold (Fig. 1).
2) Intraoral findings
The patient showed Class D canine and molar relationships. The over-jet, overbite, and curve of Spee were 6 mm, 5 mm, 2 mm, respectively. The patient had moderate arch length deficiency(upper arch, 4.5 m m : lower arch, 4 mm) (Fig. 1).
3) Cephalometric analysis(Table 1)
The cephalometric measurements revealed the skeletal Class I w ith deep bite.
2 . T r e a t m e n t
1) Treatment plan
For the relief of upper crowding,extraction of upper first premolars and lower second premolars was plarmed. The anterior bite piate was utilized to extrude lower posterior teeth and enhance m andibular growth.
Vol. 29, No. 6, 1999. Korea. J. Orthod. Skeletal cortical anchorage 니sing titankjm m icroscrew implants
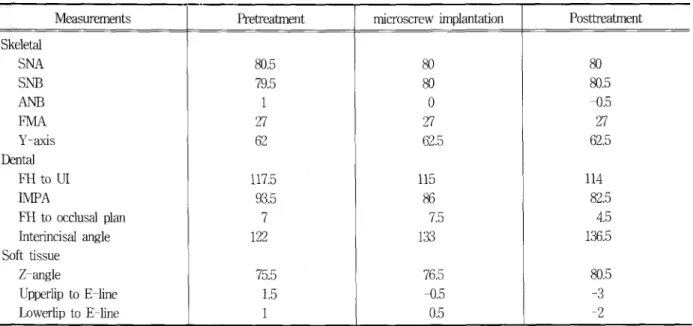
Table 1. S니m m ary o f c e p h a lo m e tric m ea s니rem ents.
Measurements Pretreatment microscrew implantation Posttreatment
Skeletal
SNA 80.5 80 80
SNB 79.5 80 80.5
ANB 1 0 -0.5
FMA 27 27 27
Y ᅳ axis 62 62.5 62.5
Dental
FH to U I 117.5 115 114
M P A 93.5 86 82.5
FH to occlusal plan 7 7.5 4.5
Interincisal angle 122 133 136.5
Soft tissue
Z-angle 75.5 76.5 80.5
Upperlip to E -line 1.5 -0.5 -3
Lowerlip to E -line 1 0.5 - 2
2) Treatment progress
After extraction, edgewise appliances were bonded and banded. In order to relieve anterior crowding, upper canines were retracted by power chain between canine and upper first molar. The patient was instructed to wear anterior bite piate full time and wear Class E elastics.
After 13 months of treatment, the author decided to im piant titanium microscrew implants, skeletal cortical anchorage, to intrude and retract upper anterior teeth, because of lack of p a tie n ti cooperation.
* Surgical procedure
Under local anesthesia, a stab incision was made on the alveolar mucosa between upper second premolar and first molar. A small pit (1.5 mm) was made by round bur under water cooling,and a mucoperiosteal flap was opened. D rilling was performed w ith 1 mm drill under water cooling.
Titanium microscrew(Leibinger Co, Germany), 6 mm in length and 1.2 mm in diameter, was inserted by screwdriver (Fig. 2). Three periapical radiographs were taken to evaluate whether microscrew was placed well between adjacent roots or not.
One month after microscrew im plantation,ortho
dontic force was applied. N iTi coii spring was ligated between titanium microscrew and hook, which was soldered on m ain archwire between upper lateral incisor and canine (Fig. 2). The force was approximately 150 gm on each side. The total treatment time was 20 months including 6 months of orthodontic force application from titanium microscrew implants,
3) Treatment resuit
The good facial harmony was obtained by superoposterior movement of upper anterior teeth segment, anterior repositioning and enhanced growth of mandible (Fig. 3 and Fig. 4).
The upper anterior teeth showed 4 mm bodily posterior and intrusive movement during orthodontic force application from skeletal cortical anchorage.
The upper posterior teeth moved backward 1.5 mm (Fig. 5).
The FH to occlusal plane was changed from 7.5 to 4.5 during skeletal cortical anchorage treatment resulting from intrusion of upper anterior teeth. The panoramic radiograph showed good root paralleling.
Hyo Sang Park 대치교정지 29권 6호’ 1999년
Fig. 3. Fmal facial photos lateral cephalom etric radiograph, intraoral photos, and panoram ic radiograph.
J k 하
-』 一■ j
쎄 ^ .
.•m —
Fig. 2. Intraoral photos showing implanting tita n i니m m icroscrew w ith screwdriver, and o rth o d o n tic force applicatiori by NiTi coii spring from skeletal cortical anchorage to 니pper anterior teeth.
■■
i
I
%
Vol. 29, No. 6, 1999. Korea. J. Orthod, Skeletal cortical anchorage using titanium m icroscrew implants
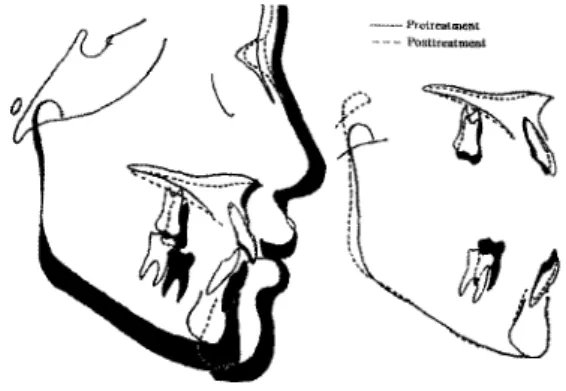
- ^ rc trca im e n i - Posttreatmenl
- M icroscn:w u n o l^ ta tio n - Posttreatoicnt
Fig. 4. S니perim position o f pretreatm ent and p o s ttr- eatm ent c e p h a lo g ra m s; Enormous amount o f m andib니lar growth as com pared with maxillary growth was observed.
D IS C U S S IO N
Fig. 5. S uperim positiᄋn o f tita n iu m microsGrew impl
antation and po sttre a tm e n t ce p h a lo g ra m:
Upper anterior teeth showed 4 mm bodily posterior and intr니sive m ovem ent; Upper posterior te e th showed 1.5 mm posterior movem ent during six months o rthodontic force application from skeletal cortical anchorage.
A t times orthodontists encounter problem cased caused by lack of anchorage. Noteworthy advanceᅳ ments in endosseous implants may help solve such problems. Orthodontists have begun to take an interest in using im plants for orthodontic anchor职 e.
In early 1945,Gainsforth and Higley5) examined the possibility of vitallium screws in orthodontic anchorage. The next reported use of implants as anchors for tooth movement was by Linkow n> There were many studies to evaluate the possibility of endosseous implants and screws as orthodontic
6ao.i3,i5,i6fi9)
^ orthopedic anchorage17) in animals.After Branemark et aTs2> research, in which he observed successful osseointegration of implants w ith bone, clinical approaches were performed.12,14,21) In 1994, Roberts et al12) presented retromolar im piant which was implanted in the mandibular retromolar area and used to close the extracted lower molar space.
Block and Hof&nan1} introduced the on-plant which was implanted on midpalatal area subperiosteally. As mentioned earlier, endosseous implants have many lim itations for orthodontic anchorage.
Creekmore and Eklund4) reported a case that intrusion of upper anterior teeth by using vitallium
screw, which was implanted to the bone just below anterior nasal spine. Umemori et al20) reported openᅳbite cases treated w ith skeletal anchorage system using surgical miniplates. Recently,Kanomi8) and Costa et al3) presented the use of small titanium microscrews as orthodontic anchorage. In regard to the extensiveness of the procedure, a skeletal anchorage system using surgical miniplates is more extensive than microscrew implants. In regard to the amount of force which can be withstood, the skeletal anchorage system is superior. But, in a biological point of view, the amount of force to retract anterior teeth does not exceed 1 N. Conceming the amount of force applied on implants, many researchers observed that implants could withstand 1 N to 6 N of force.7’13’21) There were no studies dealing with the amount of force on titanium microscrews except a study of Gray et al.6) According to Gary et aTs6) study, a 1.6 mm vitallium srew could withstand 180 gm of horizontal loading. The author had applied many different force levels in many cases.
Microscrew implants could withstand 200 gm of force(unpublished data). Skeletal cortical anchorage may be strong enough to remain stable in this range of force application. The author decided to use
Hyo Sang Park 대치교정지 29권 6호. 1999년
150ᅳ200 gm ox conunuous fo rce to re tra c t a n te rio r teeth. In th is case, tita n iu m m icro scre w im p la n ts rem ained firm and sta b le th ro u g h o u t tre a tm e n t. A M T i c o ii s p rin g w as selected fo r fo rce a p p lica tio n because i t o ffe re d con tin uous lig h t force.
T h e a u th o r d ire cte d th e fo rce to be passed th ro u g h th e center o f resistance o f th e a n te rio r te e th as m uch as possible. A fte r s ix m onths o f fo rce a p p lica tio n , th e upper a n te rio r te e th show ed 4 m m b o d ily p o s te rio r and in tru s iv e m ovem ent. T h e m o st o u tsta n d in g re s u it w as th e p o s te rio r m ovem ent o f th e upper p o s te rio r teeth, w h ic h w ere u s u a lly th e anchor u n it in conventional orthodontic treatment (F ig . 5). In other w ords, m a x illa ry w h o le d e n titio n w as m oved b a ckw a rd a g a inst sm a ll tita n iu m m icro scre w im p la n ts. These re s u lts in d ica te th a t ske le ta l c o rtic a l anchorage u sin g tita n iu m m icro scre w im p la n ts can be an absolute anchorage system fo r o rth o d o n tic m ovem ent and can re tra c t e n tire d e n titio n as fa r as i t p e rsists. T h is is co n siste n t w ith S outhard e t aTs o b se rva tio n .18)
Because th e v e c to r o f fo rce passed o ve r th e center o f resistance o f tfie w h o le m a x illa ry d e n titio n , th e occlu sal plane w as fla tte n e d I t m ay be h e lp fu l to reposm on th e m andible fo rw a rd .
T h e re w as m in o r in fla m m a tio n around tita n iu m m icro scre w im p la n ts and th e N iT i c o ii sp rin g . Because th e a u th o r used lig a tu re w ire to connect N iT i coii spring to titanium microscrew irr^lants, ligated w ire around m icro scre w neck m u st have acted as an irrita n t. L in d h e e t a l10> also found th e placem ent o f plaque re te n tiv e lig a tu re s around th e im p ia n t neck re s u ltin g in in fla m m a tio n . T h e a u th o r is p la n n in g to develop a new typ e o f tita n iu m m icro scre w im p la n ts th a t have a hook on th e head o f th e m icro scre w fo r a tta ch in g th e N iT i c o ii sp rin g . In c lin ic a l w o rk, the a u th o r trie d to use p o lye th yle n e tu b in g to w ra p th e N iT i c o ii sp rin g . I t can be a m eans o f redu cing in fla m m a tio n .
T h e studie s d e a lii^ w ith th e tim in g o f fo rce
印p lic a tio n a fte r im p la n ta tio n can be d ivid e d in to tw o groups. One grou p o f studies stated th a t th e c lin ic ia n should delay th e fo rce a p p lica tio n u n til osse o inte - g ra tio n occurred. R o b e its e t a l13) concluded fro m an
experim ent in th e fe m u rs o f ra b b its th a t im m ediate lo a d in g needed to be avoided. T h e o th e r gro u p o f studies in s is te d on im m ediate fo rc e a ^ lic a tio n3의 A s G ray e t aTs observa tion,6> as fa r as u sin g tita n iu m m icro scre w im p la n ts as o rth o d o n tic anchorage, o sseo integ ration m ig h t n o t be necessary. H e fou n d firm sta b le screw s a fte r fo rce ap p lica tio n th a t had con nective tis s u e encapsulation. In m y opim on, once s o ft tis s u e is healed i t is possib le to a p p ly o rth o d o n tic force.
S ke le ta l c o rtic a l anchorage u sin g tita n iu m m ic ro screw im p la n ts has ju s t sta rte d to be used fo r c lin ic a l purposes. T h e re are m any c lin ic a l co n sid era tio ris w e m u st c la rify s c ie n tific a lly such as th e tim in g o f fo rce ap plication, th e am ount o f force, m ethod o f force a p p lica tio n and in fla m m a tio n .
D espite some lim ita tio n s , ske le ta l c o rtic a l anchorage u sin g tita n iu m m icro scre w im p la n ts m ay be a good o p tio n fo r re in fo rc in g anchorage.
S U M M A R Y
T h e a u th o r tre a te d a p a tie n t w ith ske le ta l c o rtic a l anchorage u sin g tita n iu m m icro scre w im p la n ts a fte r p a tie n t fa ile d to cooperate d u rin g 13 m onths o f co nven tional m echanotherapy. D u rin g s ix m onths o f o rth o d o n tic fo rce a p p lica tio n usin g tita n iu m m icro scre w im p la n ts, th e upper a n te rio r te e th show ed 4 m m b o d ily and in tru s iv e m ovem ent. T h e m ost p o s itiv e re s u it w as 1.5 m m p o s te rio r m ovem ent o f upper p o s te rio r teeth. T h e tita n iu m m icro scre w im p la n ts had rem ained firm and stable th ro u g h o u t tre a tm e n t.
These re su ts in d ica te th a t ske le ta l c o rtic a l anchorage m ay be used as a n c h o r^ e fo r o rth o d o n tic m ovem ent.
R E F E R E N C E
1. B lock MS, Hof&nan DR. A N ew Device fo r Absolute Anchorage fo r O rth o d o n tics,A m J Orthod Dentofac Orthop 1995 : 107 : 251-158.
2. Branem ark PI, Breine U, H allen ᄋ,et al. Repair of Defects in the M andible , Scand J Plast Heconstr Surg 1970 : 4 : 100-108.
Vol. 29, No. 6, 1999. Korea. J. Orthod. Skeletal cortical anchorage using titanium microscrew implants
3. Costa A , R a ffini M , Melsen B. M icroscrew s as O rthodontic Anchorage , In t J A d u lt Orthod O rthogn Surg 1998 : 13 : 201-209.
4. Creekmore TD , Eklund M K . The P o ssibility o f Skeletal Anchorage , J C lin Orthod 1983 : 17 :
266-269.
5. G ainsforth BL, H igley LB . A Study o f O rthodontic Anchorage P ossibilities in Basal B o n e ,A m J Orthod Oral Surg 1945 : 31 : 406-417.
6. Gray JB, Steen M E, K ing GJ,C lark AE. Studies on the E fficacy o f Im plants as O rthodontic A n chora ge,A m J Orthod 1983 : 83 : 311-317.
7. H urzeler M B ; Quinones CR, Kohal RJ, et al; Changes in P eri—im piant Tissues Subjected to O rthodontic Forces and Ligature Breakdown in Monkeys , J Periodontol 1998 : 69 : 396-404.
8. Kanom i R. M in i-im p la n t fo r O rthodontic A nchorage,
J C lin Orthod 1997 : 31 : 763-767.
9. K ohri M , Cooper EP, Ferracane JL, W aite DF.
Comparative Study o f H ydroxyapatite and T itanium D ental Im plants in D o g s ,J O ral M axillofac Surg 1990 : 샌 : 1265-1273.
10. Lindhe J, B erglundh T ,Ericsson B, Liljenberg B, M arinello C, Experim ental Breakdown o f P e ri- im piant and Periodontal T issues-A Study in the Dog
,C lin O ral Im pl Res 1992 •• 3 : 9-16.
11. Linkow L I. The Endosseous Blade Im piant and Its Use in O rthodontics , In t J Orthod 1969 : 18 : 149-154.
12. Roberts W E, Nelson CL, Goodacre CJ. R igid Im piant Anchorage to Close a M andibular F irs t M olar E xtraction S ite , J C lin Orthod 1994 : 28 : 693-704.
13. Roberts W E, Sm ith RK, Zilberm an Y , M ozsary PG, Sm ith RS. Osseous Adaptation to Continuous Loading o f R igid Endosseous Im p la n ts ,A m J Orthod 1984 : 86 : 95-111.
14. Shapiro PA, K okich VG. Uses o f Im plants in O rtho
dontics ,Dent C lin N orth A m 1988 : 32 : 539- 550.
15. Sherman AJ. Bone Reaction to O rthodontic Forces on V itreous Carbon Dental Im plants ,A m J Orthod 1978
: 74 : 79-87.
16. Smalley W M , Shapiro PA, Hohl T H , K okich VG, Branem ark PI. Osseointegrated T ita nium Im plants fo r M axillofacial P rotraction in M o n ke ys,A m J Orthod Dentofac Orthop 1988 : 94 : 285-295.
17. Sm ith JR. Bone Dynam ics Associated w ith the C ontrolled Loading o f B ioglass-coated Alum inum E n d o ste a l Im p la n ts ,A m J O rth o d 1979 : 76 : 618-636.
18. Southard T E , B uckley M J,Spivey JD, K rizan KE, Casko JS. Intru sion Anchorage Potential o f Teeth Versus R igid Endosseous Im plants : A C linical and Radiographic E v a lu a tio n ,A m J Orthod Dentofac Orthop 1995 : 107 : 115-120.
19. T u rley PK, Kean C, Schur J, et al, O rthodontic Force A pplication to T itanium Endosseous Im piant A n g le,
O rthod 1988 : 58 : 151-162.
20. Umemori M , Sugawara J,M ita n i H, Nagasaka H, Kawam ura H . Skeletal Anchorage System fo r O pen-bite C o rre ctio n ,A m J Orthod Dentofac Orthop 1999 : 115 : 166-174.
21. W ehrbein H, M erz BR, Hammerle CHF, Lang NP.
B one-to-Im piant Contact o f O rthodontic Im plants in Humans Subjected to H orizontal Loading ,C lin Oral Im pl Res 1998 : 9 : 348-353.
Hyo Sang Park 대치교정지 29권 6호, 1999년
국문초록
iltanmm microscrew impiant 늘 이용한 skeletal cortical anchorage
계명대학교 의과대학 치과학교실
박 효 상
고정원의 조절은 교정치료에 있어서 매우 중요한 요소로 이를 보강하기 위 한 많은 노력 이 있어 왔다. 골융합성 임프 란트의 경우 확실한 고정원으로서 가능성이 인정되고 있고, 또 임상에서 많이 시도되고 있다. 그러나 임프란트를 매식 하기 위해서는 무치악이 존재해야 하거나 하악구치 후방부위에 식림해야 하는 등 장소의 제약이 있고,값이 비싸며, 골융합을 위하여 기다리는 시간이 필요하다는 등의 단점으로 인하여 보편화되고 있지는 않다.
최근 몇몇 임상가에 의하여 수술용 titanium microscrew 나 mimscrew를 교정치료시의 고정원으로 사용하려는 시 도가 있었는데, 이것은 골융합성 임프란트보다 수술이 간단하며, 가격이 저렴하고, 치조골 어느 부위이든지 식림할 수 있다는 장점이 있다.
저자는 titanium microscrew im piant를 사용한 skeletal cortical anchorage를 이용하여 통상적 인 교정치 료 동안 협 조도가 고갈된 환자를 치료하였다. 6 개월간의 titanium microscrew로 부터 가해진 교정력에 의하여 상악 전치부는 4 mm 후방 치체이동과 압하이동을 얻었다. 통상의 교정치료에서 고정원역할을 하는 상악 구치부도 1.5 mm 후방이동 되었다. titanium microscrew는 치료기간 동안 움직임없이 잘 유지되었다.
비록 과학적으로 밝혀져야할 임상적인 문제가 있기는 하나,skeletal cortical anchorage는 확실한 고정원으로서의 역할 을 할 수 있을 것으로 생각된다.
주요단어: Skeletal cortical anchorage. Titanium microscrew implants