https://doi.org/10.20307/nps.2017.23.3.169
169
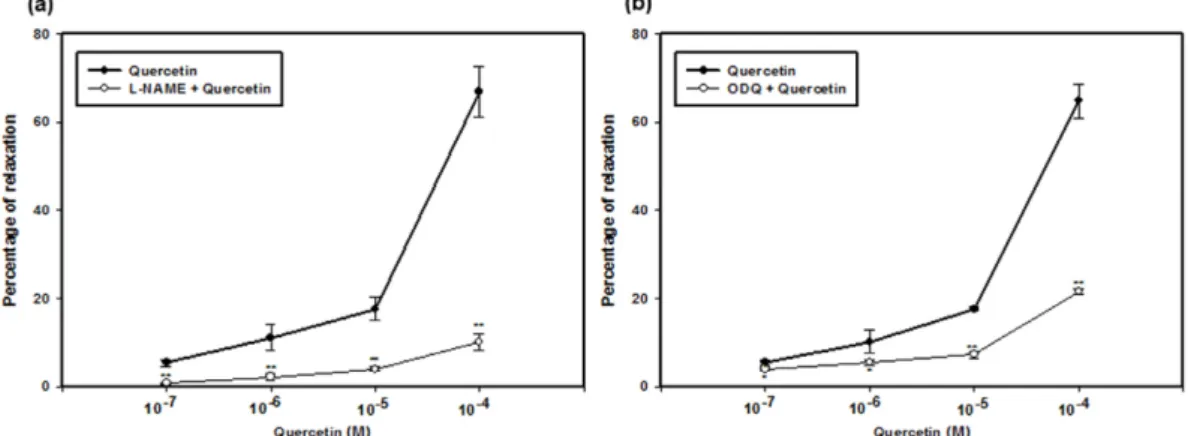
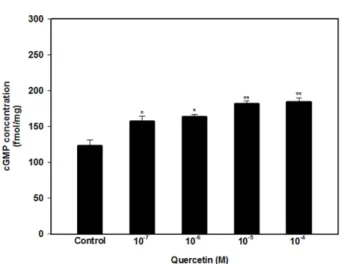
Quercetin Relaxed the Smooth Muscle of Rabbit Penile Corpus Cavernosum by Activating the NO-cGMP Signaling Pathway
Bo Ram Choi
1, Hye Kyung Kim
2,*, and Jong Kwan Park
1,*
1
Department of Urology, Chonbuk National University and Research Institute of Clinical Medicine of Chonbuk National University-Biomedical Research Institute and Clinical Trial Center of Medical Device of Chonbuk National University,
20, Geonji-ro, Deokjin-gu, Jeonju 54896, Korea
2