178
Utilization Pattern of Drug-Eluting Stents and Prognosis of Patients Who Underwent Drug-Eluting Stenting Compared with
Bare Metal Stenting in the Real World
Dong-Bin Kim, MD, Ki-Bae Seung, MD, Pum Joon Kim, MD, Sung-Ho Her, MD, Dong-Il Shin, MD, Jin-Man Cho, MD, Chul-Sool Park, MD,
Doo-Soo Jeon, MD, Sang Hong Baek, MD, Wook-Sung Chung, MD, Jae-Hyung Kim, MD, Soon-Jo Hong, MD and Kyu-Bo Choi, MD
Division of Cardiology, Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea
ABSTRACT
Background and Objectives:Currently, the drug-eluting stent (DES) has been widely used because of its excel- lent clinical outcome. We compared the utilization patterns and clinical outcomes between the DES and the bare metal stent (BMS) in the real world. Subjects and Methods:We retrospectively reviewed the stent registry at the Catholic Medical Center between January 2002 and October 2004. There were 1120 patients treated with DES (n=1837) who were compared to 910 patients who received BMS implantation (n=1238). Results:Patients with de novo lesions in the DES group more frequently had multivessel disease and received a greater number of stents than those in BMS group (p<0.001). The mean diameter of inserted stents was smaller in the DES group (p<
0.001). The follow-up rate for clinical and angiographic evaluations at 6 months after stenting was 91% and 65% (n=592) in the BMS group and 90% and 74% (n=829) in the DES group, respectively. The rate of major adverse cardiac events (death, nonfatal myocardial infarction, or target vessel revascularization) at 6 months was 7.3% in the DES group and 17.5% in the BMS group (p<0.001). The rates of target vessel revascularization in the DES group and in the BMS group were 4.2% and 12.9%, respectively (p<0.001). Conclusion:The patients in the DES group had longer length, smaller diameter and higher number of placed stents, compared to the BMS group. The rates of revascularization and major adverse cardiac events in the DES group were lower than those in the BMS group. (Korean Circulation J 2006;36:178-183)
KEY WORDS:Stents;Angioplasty;Prognosis.
Introduction
Restenosis is one of the main limitations of coronary stenting, with reported rates as high as 50% in more complex conditions.1) Recently introduced drug-eluting stents(DES) appear to be a “breakthrough” technology for the prevention of restenosis. Observational studies2) and randomized controlled clinical trials3-6) have shown a substantial reduction in the restenosis rate with DES compared to conventional stents. However, all clinical trials completed to date have included elective patients
with relatively straight forward lesions, and with low to moderate risk for restenosis. The effects of DES implan- tation in complex, unselected patients, in daily practice, remain largely unknown.7) Notably, restenosis in a small but significant proportion of patients in the SIRIUS trial, as well as other trials, occurred mainly in patients with diabetes, small vessels and long lesions.4)8) Moreover, restenosis after DES implantation has been recently shown to occur in association with complex procedures.9)
In the present study, we evaluated the impact of DES on the outcomes of patients treated in the “real world”, compared to conventional bare metal stent(BMS) im- plantation.
Subjects and Methods Study design and patient population
We reviewed patient’s angiographic findings and cli-
Received:June 1, 2005
Revision Received:October 13, 2005 Accepted:November 11, 2005
Correspondence:Ki-Bae Seung, MD,Division of Cardiology, Department of Internal Medicine, College of Medicine, The Catholic University of Korea, 505 Banpo-dong, Seocho-gu, Seoul 137-701, Korea
Tel: 82-2-590-2075, Fax: 82-2-591-1075 E-mail: [email protected]
nical data at Catholic Medical Center from January 2002 to October 2004. Almost a consecutive 1,120 patients with de novo lesions(n=1837) were treated with DES and they were compared to 910 patients who received BMS(n=1238) during the period just prior to the DES group.
We reviewed the stent registry at the Catholic Medical Center with the goal of evaluating the safety and efficacy of DES implantation for patients treated in daily routine medical practice. To include a patient population repre- sentative of the ‘real world’, we have used DES treated patients since November of 2003. As the default stra- tegy for every percutaneous coronary intervention, we used the sirolimus-eluting stent(Cypher®, Johnson &
Johnson-Cordis unit, Miami Lakes, FL) and the paclita- xel-eluting stent(Taxus®, Boston Scientific, Natick, MA).
A total of 1120 patients with de novo lesions were treated with DES and were included in the DES study group. The appropriate DES size, diameter and length, were not always available and accounted for the most common reason for nonutilization of the DES. When DES could not be passed through stenotic lesions, or economic problems were encountered, we substituted the BMS for the DES.
Patients treated with DES were compared to a group of patients treated with BMS for de novo lesions during the preceding months. The present study population was consequently composed of 2,030 patients divided into two sequential cohorts, primarily distinguished by the interventional strategy applied, either BMS or DES.
Procedures and post intervention medications All interventions were performed according to current standard guidelines and the final interventional strategy was entirely left to the discretion of the operator. An- giographic success was defined if the luminal stenosis of at least one lesion was reduced to less than 30% of the luminal diameter by quantitative coronary angiogra- phy(QCA, Pie Medical Imaging, Maastricht, Nether- lands) in the presence of Thrombolysis In Myocardial Infarction(TIMI) grade 3 flow. The amount of stenosis of the target lesion, before and after the intervention, was calculated by QCA. Periprocedural antithrombotic medications were used according to the operator’s de- cision; all patients were advised to maintain lifelong aspirin(100 mg/day). A course of at least 1-month ticlo- pidine treatment(250 mg bid/day) was recommended for patients in the BMS group. For patients treated with DES, clopidogrel(75 mg/day) or ticlopidine(250 mg bid/day) were prescribed for at least 6 months.
End points definitions and clinical follow-up The primary clinical end point of the study was a composite of major adverse cardiac events(MACE) at 6 months defined as death, nonfatal myocardial infarc-
tion, or target vessel revascularization(TVR). A non- Q-wave AMI was defined as troponin I elevation above the upper limit of normal and creatine kinase-MB en- zyme elevation ≥3 times the upper limit of the normal.
When in addition to enzyme elevation, there were new pathological Q waves observed on the electrocardiogram, the event was defined as a Q-wave AMI. Target lesion revascularization(TLR) was defined as a repeat revas- cularization with a stenosis ≥50% within the stent or in the 5-mm distal or proximal segments adjacent to the stent; TVR was defined as repeat revascularization within the treated vessel.
Information about the in-hospital outcomes and post discharge outcomes were obtained from medical records.
Most patients received noninvasive testing for myocar- dial ischemia. During follow-up, coronary angiography was performed as per routine follow-up or if clinically indicated by symptoms or documentation of myocardial ischemia. We tried to do angiographic re-study on all patients after 6 months regardless of ischemic symp- toms. Clinically driven repeat revascularization was de- fined as any intervention motivated by a significant luminal stenosis(>50% diameter stenosis) in the pre- sence of anginal symptoms and/or proven myocardial ischemia in the target vessel territory by noninvasive testing.
Statistical analysis
Continuous data were expressed as mean±standard deviation(SD) and were compared by means of the Stu- dent unpaired t-test. Categorical variables were presented as counts and percentages and compared by means of the Chi-square test. All statistical tests were 2-tailed.
Computation was performed using the SPSS statistical package, version 11.5(SPSS Inc, Chicago, IL).
Results Patient characteristics
Between January 2002 and October 2004, 910 patients received the DES and 1120 patients received the BMS.
Clinical follow up at 6 months was achieved in 92%
(n=857) in the DES and in 89% patients(n=997) in BMS group(p=0.12); Angiographic follow-up was per- formed on 62%(n=564) in the DES group and 47%
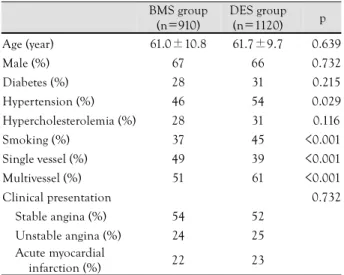
(n=526) in the BMS groups(p<0.001). With the ex- ception of a significantly higher percentage of hyper- tension, smoking and multivessel disease in the DES group, the two groups were similar with respect to all other variables examined. The patient characteristics in the study population are presented in Table 1.
Procedural characteristics
The lesions in the two groups were treated similarly with the use of conventional techniques. We used cypher
(n=1003, 81%) and taxus stents(n=235, 19%) in the DES group. Bx velocity(n=409, 33%), Express(n=223, 18%), Tsunami(n=186, 15%), Coroflex(n=99, 8%), S7(n=124, 10%), MAC(n=74, 6%), Multilink(n=111, 9%), and other stents(n=12, 1%) were used in BMS group. Patients treated with DES had a significantly hig- her number of stents used(2.11±0.76 vs.1.52±0.62 in BMS group)(p<0.001). In addition, the total stented length per patient was longer in the DES group(35.3±
18.3 mm vs. 21.5±13.0 mm in BMS group)(p<0.001).
The primary success rate as measured by angiography was similar in both groups(Table 2).
The reference diameter was significantly smaller in the DES group(2.91±0.69 mm vs. 3.11±0.78 mm in BMS group). Complex lesions were more frequent in the DES group(p<0.001) and smaller diameters of the stents used were more frequent in the DES group(p<0.001) (Table 3).
Clinical outcomes
Follow-up clinical information was obtained from the medical record. The six-month risk for MACE was sig- nificantly reduced in the DES group(7.3% vs. 17.5% in the BMS group, p<0.001). The TVR was significantly lower in the DES group than in the BMS group(4.2%
vs. 12.9%, p<0.001)(Table 4).
Subgroup analysis
Among the 602 patients with diabetes(30 percent of the total study population; 255 patients in the BMS group and 347 patients in the DES group), the rates of 6-months MACEs were higher than those among pati- ents without diabetes in both treatment groups(23.1%
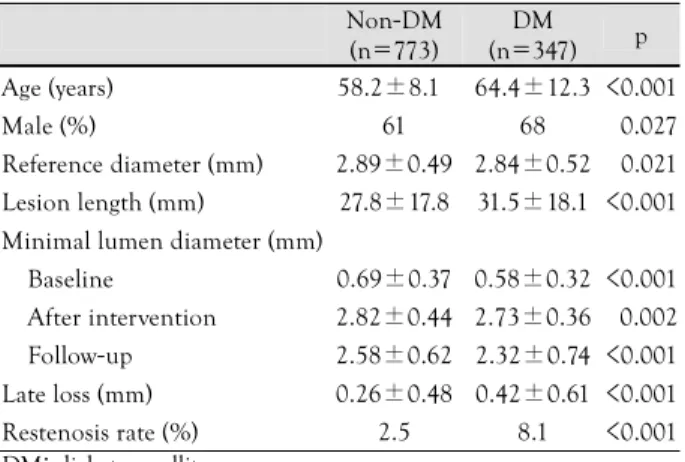
vs. 15.5% in BMS groups, 11.1% vs. 5.5% in DES group, respectively p<0.001). Patients with diabetes mellitus (DM) were older(64.4±12.3 years vs. 58.2±8.1 years, p<0.001), and included a higher percentage of males (68% vs. 61%, p=0.027), compared to patients without DM. The reference diameters were 2.84±0.52 mm in the DM patients and 2.89±0.49 mm in the non-DM patients(p=0.021). Lesion lengths were 31.5±18.1 mm in the DM patients and 27.8±17.8 mm in the non-DM patients(p<0.001). The minimal lumen diameters of the DM patients were narrower than those of patient with- out DM, before(0.58±0.32 mm vs. 0.69±0.37 mm, p<0.001) and after intervention(2.73±0.36 mm vs.
2.82±0.44 mm, p<0.001). Late losses at 6 months were 0.42±0.61 mm in the DM patients and 0.26±0.48 mm in the non-DM patients(p<0.001). Restenosis rates at
Table 1. Baseline characteristics of patients treated with bare metal stents and drug eluting stents
BMS group (n=910)
DES group (n=1120) p Age (year) 61.0±10.8 61.7±9.7 <0.639
Male (%) 67 66 <0.732
Diabetes (%) 28 31 <0.215
Hypertension (%) 46 54 <0.029
Hypercholesterolemia (%) 28 31 <0.116
Smoking (%) 37 45 <0.001
Single vessel (%) 49 39 <0.001
Multivessel (%) 51 61 <0.001
Clinical presentation <0.732
Stable angina (%) 54 52
Unstable angina (%) 24 25
Acute myocardial
infarction (%) 22 23
BMS: bare metal stents, DES: drug eluting stents
Table 4. Six-month outcomes of patients treated with bare metal stents and drug eluting stents
BMS group (n=910)
DES group (n=1120)
p
MACE (%) 17.5 7.3 <0.001
Death (%) 01.4 0.8 <0.200
Nonfatal MI (%) 04.1 3.2 <0.338
TVR (%) 12.9 4.2 <0.001
TLR (%) 08.8 2.6 <0.001
Restenosis rate (%) 12.3 3.2 <0.001 MACE: major adverse cardiovascular event, MI: myocardial infarction, TVR: target vessel revascularization, TLR: target lesion revasculariza- tion, BMS: bare metal stents, DES: drug eluting stents
Table 2. Angiographic and procedural characteristics of patients trea- ted with bare metal stents and drug eluting stents
BMS group (n=910)
DES group (n=1120) p Number of implanted stents 1.52±0.62 2.11±0.76 <0.001 Total stented length per
patient (mm) 21.5±13.0 35.3±18.3 <0.001 Angiographic success of all
lesions (%) 99 98 <0.238
BMS: bare metal stents, DES: drug eluting stents
Table 3. Angiographic and procedural characteristics of stents accor- ding to bare metal stents and drug eluting stents
BMS groups (n=1238)
DES groups (n=1837)
p
Reference diameter (mm) 3.11±0.78 2.87±0.71 <0.001
Treated artery <0.545
Left main artery (%) 01 01
Left anterior descending
artery(%) 40 41
Left circumflex artery (%) 31 29 Right coronary artery (%) 29 29 ACC/AHA type
Type A (%) 14 09 <0.001
Type B1 (%) 26 23 <0.001
Type B2 (%) 33 28 <0.001
Type C (%) 27 39 <0.001
Mean diameter per stent (mm) 3.37±0.41 3.11±0.23 <0.001 Angiographic success (%) 99 98 <0.219 ACC/AHA: American College of Cardiology/American Heart Asso- ciation, BMS: bare metal stents, DES: drug eluting stents
6 months were 8.1% in the DM patients and. 2.5% in the non-DM patients(p<0.001)(Table 5).
The results of long-stenting were as follows. A total of 173 patients(178 lesions) were implanted with 1 DES or ≥2 DES with overlapping stents in a coronary lesion more than 30 mm in length. Follow up angiograms were done in 57 patients among 173 patients. The total bi- nary restenosis rate was 5.26%(3 of 57 patients). The mean clinical follow-up and angiographic follow-up were, relatively, 6.3±4.1 months and 5.6±2.5 months. Fol- low-up angiography showed the late lumen losses at 6 months were 0.16±0.18 mm(proximal 5 mm of in-seg- ment), 0.20±0.46 mm(within the stent) and 0.18±
0.34 mm(distal 5 mm of in-segment)(Table 6). The rate of MACE in long-stenting at 6 months was 8.7%(15 of 173 patients).
Discussion
DES implantation has been shown to markedly dec- rease the incidence of restenosis in the context of ran- domized trials.3-6) However, these studies have enrolled patient populations referred for elective intervention without complex lesions. As a consequence, the findings from these studies cannot be directly extrapolated to
many patients treated in everyday practice, where com- plex, nonselected cases are the rule rather than the excep- tion. In the present study, DES with paclitaxel or sirolimus was equivalent to BMS in terms of survival rate.
However, DES implantation was associated with a reduc- tion in the rates of repeat revascularization and MACE at 1 year in unselected patients. Our results are suppor- ted by trials conducted in Germany and the Nether- lands.10)11)
Our study used a strategy that compared DES to con- ventional approaches that used BMS in the pre-DES era.
Although the two study groups were consecutively in- cluded over a total period of 3 years, some important differences were noted in the interventional strategy applied. Patients in the DES phase were treated with an aggressive interventional approach, with a significant increase in the number and length of implanted stents and a decrease in the diameter of the stents. Our fin- dings may also reflect an attempt to accomplish more complete lesion coverage and ensure uniform drug de- livery over the entire diseased segment; this is impor- tant since stent discontinuity and edge injury have been recently shown to be associated with post-DES reste- nosis.9) Moreover, the higher degree of complexity of patients treated with DES(e.g., high rates of multives- sel disease, type C lesions) may translate into a change in the decision-making process promoted by the avai- lability of DES. Although both study groups differed in some baseline and procedural characteristics, which may somewhat limit an unbiased comparison between them, hypertension, smoking and multivessel disease would traditionally be expected to increase the incidence of late complications in the DES treated patients.
The three principal determinants of restenosis after coronary-stent implantation are DM status, the refe- rence-vessel diameter and the lesion length.12) In parti- cular, patients with diabetes are prone to a diffuse and rapidly progressive form of atherosclerosis, which increa- ses their likelihood of requiring revascularization.13)14) The risk of restenosis was increased by approximately 50 percent among diabetic patients who received a BMS as compared with those without diabetes who received such a stent.15) By contrast, the risk of restenosis was re- duced by more than 80 percent among patients with diabetes who received a DES.16) The subgroup analysis of our DM patients showed that DES markedly reduced the incidence of restenosis when compared to BMS, both in patients without diabetes and in those with diabetes.
Recent studies show the same results.17)18) However, the restenosis rate is still higher in the DM group despite DES.16) Our results also showed that the restenosis rate is higher in the DM group in the DES era. Revascu- larization strategies for DM patients with multivessel disease have two options, percutaneous coronary inter- vention or aortocoronary bypass surgery. Aortocoronary
Table 6. Utilization pattern of drug eluting stents in patients with long lesions (lesion length >30 mm or overlapping stent)
Post-procedure Proximal 5 mm In-stent Distal 5 mm RD (mm) 2.83±0.47 2.86±0.51 2.52±0.39 MLD (mm) 2.61±0.46 2.46±0.45 2.23±0.46
% DS 08 14 12
Follow-up duration: 5.6±2.5 months
RD (mm) 2.78±0.49 2.82±0.52 2.44±0.39 MLD (mm) 2.45±0.52 2.26±0.55 2.05±0.46
% DS 12 20 16
Late lumen loss (mm) 0.16±0.18 0.20±0.46 0.18±0.34 RD: reference diameter, MLD: minimal lumen diameter, DS: diame- ter stenosis
Table 5. Utilization pattern of the drug eluting stent in diabetes mel- litus patients
Non-DM (n=773)
DM (n=347) p Age (years) 58.2±8.10 64.4±12.3 <0.001
Male (%) 61 68 <0.027
Reference diameter (mm) 2.89±0.49 2.84±0.52 <0.021 Lesion length (mm) 27.8±17.8 31.5±18.1 <0.001 Minimal lumen diameter (mm)
Baseline 0.69±0.37 0.58±0.32 <0.001 After intervention 2.82±0.44 2.73±0.36 <0.002 Follow-up 2.58±0.62 2.32±0.74 <0.001 Late loss (mm) 0.26±0.48 0.42±0.61 <0.001 Restenosis rate (%) 2.5 8.1 <0.001 DM: diabetes mellitus
bypass surgery is considered to be the preferred revas- cularization strategy as reported in the BARI study using a balloon technique.19) However, recent data using the BMS has demonstrated comparable survival rates bet- ween PCI and CABG in the DM groups.20-22) Therefore, using DES, for DM patients with multivessel disease, will improve both the survival rate and MACE.
Long stenting using BMS is an independent predictor of restenosis and adverse events. Long stenting is fre- quently associated with prolonged intracoronary manipu- lation due to multiple and overlapping stent placement, which may lead to injury to vessel wall integrity. More- over, the greater metal density may potentially be asso- ciated with a higher degree of local vascular injury; these concerns may increase the risk of cardiac events and restenosis. The incidence of late complications has been reported to be directly proportional to the total length of stents implanted.23)24) Previously, Schalij et al repor- ted a 25% incidence of major adverse events for patients treated with the BMS at a mean stented length of 45 mm.25) The Additional Value of NIR Stents for the Treat- ment of Long Coronary Lesions(ADVANCE) Study26) showed the reported MACE rate was 23%. However, recent studies with DES(Degertekin et al.23) and Scho- fer et al.24)) showed a reduced restenosis as well as re- duced MACEs rate. Our study also revealed the relatively low incidence of MACEs rate(8.9%) with a long length implanted DESs(40±10.1 mm on average).
Overall, the treatment results from DES were signifi- cantly better than BMS. However, the presence of dia- betes and the treatment of long lesions were shown to independently increase the incidence of complications.
These findings highlight the need for further study with a larger group of patients to fully determine the clini- cal impact of DES in higher-risk patients and in-stent restenosis27-29) in these patients.
Conclusion
This study demonstrates that utilization of DES in the “real world” is safe and effective for reducing reva- scularization and incidence of MACEs at 6 months, compared to BMS implantation.
REFERENCES
1) Lowe HC, Oesterle SN, Khachigian LM. Coronary in-stent res- tenosis: current status and future strategies. J Am Coll Cardiol 2002;39:183-93.
2) Sousa JE, Costa MA, Abizaid AC, et al. Sustained suppression of neointimal proliferation by sirolimus-eluting stents: one-year an- giographic and intravascular ultrasound follow-up. Circulation 2001;104:2007-11.
3) Park SJ, Shim WH, Ho DS, et al. A paclitaxel-eluting stent for the prevention of coronary restenosis. N Engl J Med 2003;348:
1537-45.
4) Moses JW, Leon MB, Popma JJ, et al. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coro-
nary artery. N Engl J Med 2003;349:1315-23.
5) Morice MC, Serruys PW, Sousa JE, et al. A randomized compa- rison of a sirolimus-eluting stent with a standard stent for coronary revascularization. N Engl J Med 2002;346:1773-80.
6) Stone GW, Ellis SG, Cox DA, et al. A polymer-based, paclitaxel- eluting stent in patients with coronary artery disease. N Engl J Med 2004;350:221-31.
7) Seung KB. Drug eluting stent and percutaneous coronary inter- vention. Korean Circ J 2003;33:857-60.
8) Yoon HJ, Kim KS, Park HS, et al. Clinical and angiographic factors affect on in-stent restenosis. Korean Circ J 2003;33:
1084-92.
9) Lemos PA, Saia F, Ligthart JM, et al. Coronary restenosis after sirolimus-eluting stent implantation: morphological description and mechanistic analysis from a consecutive series of cases.
Circulation 2003;108:257-60.
10) Zahn R, Hamm CW, Zeymer U, et al. “Real life” use of sirolimus- eluting coronary stents in Germany. Z Kardiol 2004;93:287-94.
11) Lemos PA, Serruys PW, van Domburg RT, et al. Unrestricted utilization of sirolimus-eluting stents compared with conventional bare stent implantation in the “real world”. Circulation 2004;
109:190-5.
12) Serruys PW, Kay IP, Disco C, Deshpande NV, de Feyter PJ.
Periprocedural quantitative coronary angiography after Palmaz- Schatz stent implantation predicts the restenosis rate at six months: results of a meta-analysis of the Belgian Netherlands Stent Study (BENESTENT) I, BENESTENT II pilot, BENESTENT II and MUSIC trials. J Am Coll Cardiol 1999;34:1067-74.
13) Kornowski R, Mintz GS, Kent KM, et al. Increased restenosis in diabetes mellitus after coronary intervention is due to exaggera- ted intimal hyperplasia. Circulation 1997;95:1366-9.
14) Syeda B, Wexberg P, Gyongyosi M, et al. Mechanism of lumen gain during coronary stent deployment in diabetic patients com- pared with non-diabetic patients. Coron Artery Dis 2002;13:
263-8.
15) Kastrati A, Schomig A, Elezi S, et al. Predictive factors of res- tenosis after coronary stent placement. J Am Coll Cardiol 1997;
30:1428-36.
16) Hermiller JB, Raizner A, Cannon L, et al. Outcomes with the polymer-based paclitaxel-eluting TAXUS stent in patients with diabetes mellitus: the TAXUS-IV trial. J Am Coll Cardiol 2005;45:
1172-9.
17) Dibra A, Kastrati A, Mehilli J, et al. Paclitaxel-eluting or siroli- mus-eluting stents to prevent restenosis in diabetic patients. N Engl J Med 2005;353:663-70.
18) Fajadet J, Morice MC, Bode C, et al. Maintenance of long-term clinical benefit with sirolimus-eluting coronary stent: three-year results of the RAVEL trial. Circulation 2005;111:1040-4.
19) Bypass Angioplasty Revascularization Investigation Investigators.
Comparison of coronary bypass surgery with angioplasty in pa- tients with multivessel disease. N Engl J Med 1996;335:217-25.
20) Gwon HC, Choi SH, Choi BI, Cho SY, Ro YM, Lee WR. Per- cutaneous coronary intervention versus coronary artery bypass grafting for patients with multivessel coronary artery disease.
Korean Circ J 2003;33:786-96.
21) Feit F, Brooks MM, Sopko G, et al. Long-term clinical outcome in the bypass angioplasty revascularization investigation registry:
comparison with the randomized trial. Circulation 2000;101:
2795-802.
22) Kurbaan AS, Bowker TJ, Ilsley CD, et al. Difference in the mor- tality of the CABRI diabetic and non-diabetic populations and its relation to coronary artery disease and the revascularization mode. Am J Cardiol 2001;87:947-50.
23) Degertekin M, Arampatzis CA, Lemos PA, et al. Very long si-
rolimus-eluting stent implantation for de novo coronary lesions.
Am J Cardiol 2004;93:826-9.
24) Schofer J, Schluter M, Gershilck AH, et al. Sirolimus-eluting stents for treatment of patients with long atherosclerotic in small coro- narhy arteries: double-blind, randomized controlled trial (E- SIRIUS). Lancet 2003;362:1093-9.
25) Schalij MJ, Udayachalerm W, Oemrawsingh P, Jukema JW, Rei- ber JH, Bruschke AV. Stenting of long coronary artery lesions:
initial angiographic results and 6-month clinical outcome of the micro stent II-XL. Catheter Cardiovasc Interv 1999;48:105-12.
26) Serruys PW, Foley DP, Suttorp MJ, et al. A randomized compa- rison of the value of additional stenting after optimal balloon angioplasty for long coronary lesions: final results of the addi-
tional value of NIR stents for treatment of long coronary lesions (ADVANCE) study. J Am Coll Cardiol 2002;39:393-9.
27) Sousa JE, Costa MA, Abizaid A, et al. Sirolimus-eluting stent for the treatment of in-stent restenosis: a quantitative coronary an- giography and three-dimensional intravascular ultrasound study.
Circulation 2003;107:24-7.
28) Degertekin M, Regar E, Tanabe K, et al. Sirolimus-eluting stent for treatment of complex in-stent restenosis: the first clinical ex- perience. J Am Coll Cardiol 2003;41:184-9.
29) Saia F, Lemos PA, Arampatzis CA, et al. Routine sirolimus eluting stent implantation for unselected in-stent restenosis: insights from the rapamycin eluting stent evaluated at Rotterdam Cardiology Hospital (RESEARCH) registry. Heart 2004;90:1183-8.