Effect of Simultaneous Nephrectomy on Perioperative Blood Pressureand Graft Outcome in Renal Transplant Recipients with Autosomal Dominant Polycystic Kidney Disease
8
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
(7)
(8)
수치
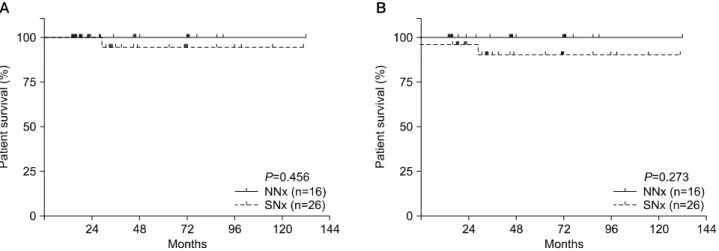

![Fig. 2. (A) Mean blood pressure (BP; mmHg, mean±SD [total no.]) and (B) units of antihypertensive medication during follow-up period after nephrectomy](https://thumb-ap.123doks.com/thumbv2/123dokinfo/5443568.651251/6.892.91.797.151.547/mean-blood-pressure-antihypertensive-medication-follow-period-nephrectomy.webp)
관련 문서
