노인의 정신건강 문제의 발견과 관련서비스 이용에 관한 연구
Study on the Early Detection of Mental Health Problems in the Elderly and the Utilization of Related Services
박경순*, 박영란**, 손덕순***, 염유식****
연세대학교 고령화융복합연구센터*, 강남대학교 실버산업학과**, 용인송담대학교 사회복지과***, 연세대학교 사회학과****
Kyungsoon Park([email protected])*, Yeong-Ran Park([email protected])**, Duksoon Son([email protected])***, Yoosik Yum([email protected])****
요약
본 연구는 가족돌봄자가 노인의 정신질환을 주로 어떤 증상을 통해 발견하였는지를 알아보는 한편, 가족돌 봄자를 중심으로 노인의 정신건강서비스를 이용하게 이끄는 주된 원인이 무엇인지를 실증적으로 검증하고자 하였다. 이를 위해 정신건강문제를 갖고 지역사회에 거주하는 노인을 돌보는 가족돌봄자를 대상으로 설문조사 를 실시하였으며 이를 통해 수집된 324명의 자료로 이항 로지스틱 회귀분석을 실시하였다. 연구결과를 보면 첫째, 가족돌봄자가 노인 환자의 정신건강질환을 의심하게 된 주된 증상은 기억력 저하와 다른 인지기능 저하 가 가장 많은 것으로 확인되었다. 둘째, 노인이 노인 정신건강서비스를 이용하는데 영향을 미치는 요인으로는 노인의 장기요양등급, 가족돌봄자의 나이, 노인을 돌본 기간, 가족돌봄자가 느끼는 돌봄 스트레스의 수준, 가족 돌봄자의 노년기 정신질환에 대한 이해, 가족돌봄자의 지역사회 정신건강서비스에 대한 인지도가 영향을 미치 는 것으로 확인되었다. 이러한 연구결과를 토대로 노인 가족돌봄자의 관점에서 노인 정신건강문제 조기 발견 과 대응 및 관련서비스 이용을 위한 정책적·실천적 함의를 제시하였다.
■ 중심어 :∣노인∣정신건강∣조기 발견∣정신건강서비스 이용∣가족돌봄자∣
Abstract
This study aims at investigating the major symptoms that help family carers detect mental illness in elderly patients. Another purpose of this study is to empirically verify the major factors determining the utilization of mental health services with a focus on family carers. The results of this study are as follows. First, the most commonly detected symptoms that caused the family carers to suspect mental illness in the elderly patients were memory decline and other forms of cognitive function decline.
Second, the determinants of the elderly’s utilization of mental health services included the patient's long-term care insurance level, the age of the family carer, the period of care, the level stress associated with the provision of care felt by the carer, his understanding of geriatric mental illness, and the level of perception about community mental health services. Based on these findings, this study suggests policies and practical implications for the early detection of and response to elderly mental health problems and the utilization of related services from the viewpoint of the family carers of the elderly.
■ keyword :∣Elderly∣Mental Health∣Early Detection∣Service Utilization∣Family Carer∣
* 본 연구는 2017년 정부(교육부)의 재원으로 한국연구재단(NRF-2017S1A3A2067165)의 지원과 보건복지부 정신건강기술개 발단(HM15C0995)의 지원을 받아 수행되었습니다
접수일자 : 2019년 07월 08일
수정일자 : 2019년 08월 09일 심사완료일 : 2019년 08월 09일
교신저자 : 박경순, e-mail : [email protected]
I. 서 론
The Korean society is rapidly becoming an ageing society and one that is highly-stressed.
This has led to the rise in the national prevalence rate of illnesses related to mental health, including various emotional disorders(anxiety, depression, obsession), cognitive disorders(mild cognitive impairment, dementia), developmental disorders(ADHD, learning disability, autism), cerebral apoplexy, addiction(gaming, alcohol), sleep disorders, stress disorders(chronic fatigue, headache, hwa-byung, panic disorder). According to the data of the Health Insurance Review and Assessment Service[1], more than half of the patients with mental and behavioral disorders falling under F00-99, G40, and G41 were in their 50s in 2014. The increasing trend in the number of patients with these disorders is expected to continue in the future due to the ageing of the society and the weakened family support. The increase in the prevalence rate of mental illness among aged people causes problems in elderly care with the rise in social costs.
The number of people aged 70 or older among patients with panic disorders, which are known to cause "greater pain than death,” has increased 3.4 times for the past 5 years(2010-2015)[2]. In a national survey on elderly life conditions in 2017, 21.1% of Korean senior citizens were found to have depression[3]. In addition, Korea's national suicide rate in the elderly, which has been the highest among OECD countries over the past decade, amounts to 54.8 per 0.1 million people, which is nearly three times higher than the OECD average of 18.4[4]. The number of
patients with dementia among the elderly aged 65 or older was 648,223 in 2015, which was estimated to be 9.8% of the total aged population[5]. As the ageing rate of the society has continued to accelerate, the number of elderly people suffering from mental health problems, which can degrade the quality of life as much as physical health problems, has been also on the rise. Among these problems, dementia, cognitive impairment, and depression are often recognized as general symptoms of ageing. In many cases, however, the severity of mental health-related diseases is recognized only after the elderly patients attempt suicide or such symptoms worsen. In addition, the prejudice and stigma by the Korean society against mental illness make difficult the acceptance of mental health problems of the elderly patients among their families.
Consequently, it also creates difficulty in accessing information about mental illness in the elderly, which hampers early treatment.
Although mental illness can be fully treated through early intervention, delayed treatment can cause chronicization, which may lead to more severe dysfunction[6].
Meanwhile, despite the change in the family
structure, many elderly parents are still
dependent on their adult children for social
support, such as emotional, instrumental,
informative, and evaluative support, even
though they live separately from them. For this
reason, if a mental health problem occurs in
the elderly, it is highly likely that their family
will detect it first. Elderly people with mental
health problems are more likely to have
difficulties in making the best autonomous
choices for their health problems than those
with physical health problems. Moreover, they
often rely on their families. In addition, the idea that adult children are responsible for the care of their elderly parents is still shared among middle-aged and aged people in Korea due to the influence of traditional Confucian culture.
Accordingly, the Korean society believes that making decisions about the medical treatment of elderly parents and providing for them are the responsibilities and obligations of their children. Therefore, it is considered that the family carers have significant decision-making influence to use mental health services for the elderly. However the lack of knowledge and information about mental health and prejudice in family carers can sometimes act as the factors that impede the early treatment of elderly mental health problems. Nevertheless, studies on mental health in the elderly carried out in Korea to date have shown little interest in family carers. Rather, their focus has been limited to other issues such as the stress or burden of family carers. Therefore, given the characteristics of Korean culture, it would be meaningful to empirically examine the influence of the factors related to the use of mental health services for the elderly with a focus on family carers.
Against this background, this study was conducted to investigate the major symptoms that help family carers detect mental illness in the elderly. This is under the assumption that the family is most likely to first identify the mental health problems in the elderly. In addition, it intended to focus on family carers and empirically examine the main factors affecting the elderly’s mental health service utilization.
Ⅱ. Theoretical Background
Preceding studies have reported many cases where the delay in the treatment of the elderly with dementia was due to their families' perception of its symptoms as part of ageing[7].
It is, however, ill-advised to apply this finding to other cases of the elderly with mental health problems due to the lack of research on geriatric mental health. In addition, it has been reported that family carers, the main carers of the elderly living in the community, have a low understanding of dementia and are caring for the elderly with dementia without the appropriate knowledge about its symptoms and coping measures[8]. In Korea, the responsibility of caring for elderly people with mental health problems has been imposed mainly on their families in the absence of public social support.
In this situation, it was difficult to ask adequate care for the elderly from their families.
Therefore, preceding studies on family carers
have also focused on the issues, including the
burden of care, care stress, or the quality of life
among family carers[9-13]. Many of preceding
studies on the use of elderly welfare services in
Korea pertain to the use intentions or
experiences related to home and facility
welfare services in terms of long-term care for
the elderly while few address the utilization of
elderly mental health services. Most of these
studies present analyses using the Andersen
model. There are also studies that were carried
out before the introduction of the long-term
care insurance system or analyses on the pilot
projects for the introduction of the system that
show a lack of consistency in their
results[14-17]. The long-term care insurance
system that was introduced in July 2008 brought
a great change to our society with the concept of social care. Among the preceding studies on the use of social welfare services for the elderly, those related to family carers after the implementation of the system are as follows.
First, Park and Yang(2008) reported that the age of the dependent, the status of his spouse, the provider's income, ADL limitations, and the provider's relationship with the dependent (spouse, daughter-in-law, etc.) influence the decision on hospital care[18]. Park(2010) found that there are differences in the use of facility or home services, visiting nursing services, and long-term care hospital services depending on the provider's age, household income, the number of diseases suffered by the elderly, alternative resources for support, level of long-term insurance, educational level of the provider, his relationship with the dependent(son, etc.), and whether or not the provider is living with the dependent[19].
Among preceding Korean studies on the use of mental health services for the elderly is that of G. Lee et al.(2010)[20]. The researchers investigated the factors affecting the intention to use mental health services among the elderly living in farming and fishing communities. The study reported that their educational level, participation level to social activities, and perception level of services, as well as whether they are living alone or with their children and grandchildren affect their intention to use mental health services. The study is significant in that it extended the scope of elderly healthcare into mental health services for the elderly while the preceding studies on the use of elderly welfare services had focused only on physical health services for aged people.
However, the study has a limitation that it only
examined use intention rather than the utilization status of services.
While domestic studies on the use of relevant services have been rare due to the short history of provision of mental health services for the elderly in Korea, a number of studies have been accumulated in countries where social welfare services are highly advanced. Neese et al.(1999) found that the determinants of the use of mental health services of older people in rural areas were marital status and types of health insurance[21]. In addition, since socioeconomic status(SES) affects an individual's mental health and accessibility to mental health services, older people with lower socioeconomic status showed higher morbidity rate for mental health diseases and thus higher usage of mental health services[22][23].
According to Volkert and others(2018), in a comparative study of older people living in various European communities, only 11% of them with mental health problems were using mental health services. Factors affecting mental health service utilization were gender, education level, residential area, functional impairment, and accompanying mental illness.
In other words, males rather than females, older people with lower education level, and residents of London rather than those in other European regions were less likely to use mental health services. Also, older people with more functional impairment and accompanying mental illness used more mental health services than their counterparts[24].
In a study of Chinese older people who
belong to a society with Confucian culture as in
Korea, residential areas, education levels,
marital statuses, health insurance statuses and
household incomes have been shown to affect
elderly people's utilization of mental health services[25]. That is, older people who live in urban areas, have higher education levels, are married, have medical insurances, and have higher household incomes were found to use mental health services more. In a broad sense, previous studies have found that accessibility to services, as well as individual, sociocultural and economic factors affect the older people’s utilization of mental health services.
Ⅲ. Study Methods
1. Study Subjects and Data Collection Methods
The subjects of this study were the family carers who were taking care of the elderly with mental health problems. The subjects were limited to the family members who were 20 years of age or older and who provided physical, emotional, and instrumental support to the elderly patients for at least one hour a day, whether they were living with or separately from the elderly. The elderly people cared for by the family carers included those who were 60 years of age or older and who were members of a regional community. This aged group had also been perceived to have an illness related to mental health by their families or diagnosed with such illness by doctors. Information on the study subjects was collected from the family carers using the elderly mental health centers, mental health centers, geriatric hospitals, long-term care hospitals, dementia centers, community health centers, and the elderly welfare institutions operating daycare facilities in Yongin and Suwon. The data was collected through the purposive sampling method with
the assistance of these institutions. The survey was conducted for about one month from April 11 to May 13, 2015, using a structured self-administered questionnaire. A total of 350 copies of the questionnaires were distributed and 324 copies were used for analyses, excluding 22 unreturned copies and 4 copies with unreliable or inappropriate answers.
2. Definition and Measurement of Variables As can be seen in [Table 1], the dependent variable is the experience of using elderly mental health service institutions in the community, specifically mental health centers, suicide prevention centers, addiction management centers, community health centers, psychiatric hospitals and clinics, geriatric hospitals, long-term care hospitals, day and night care centers, metropolitan/provincial dementia centers, and community dementia centers. The experience of using each of these institutions was coded as 1 and no experience as coded as 0. After totaling the values for each institution, the experience of using either of these institutions was re-coded as 1 and no such an experience was re-coded as 0 to be used in the analyses.
3. Analysis Methods
A frequency analysis and descriptive statistics
were performed to examine the general
characteristics of the subjects and the elderly
who were cared for by the subjects, the mental
health service utilization status, symptoms of
suspected mental illness, countermeasures,
reasons for delayed treatment, as well as the
subjects' understanding of geriatric mental
illness. In addition, to answer the research
questions of this study, a binary logistic
regression analysis was performed to identify the factors related to the experience of using mental health services for the elderly, which was operationalized as a nominal variable. In particular, the sociodemographic factors of the subjects and the elderly who were cared for were first put into the model, followed by the period of care, the level of care stress, the understanding of elderly mental illness, and the perception level of mental health services for the elderly, in order. This method was used to examine the influence of the factors related to elderly care on the service utilization with the controlled sociodemographic factors, from the viewpoint of the family carers. That is, a hierarchical binary logistic regression analysis was conducted to determine the effects of the conditions, understanding, and the perception of the family carers such as the period of care, level of care stress, the understanding of elderly mental illness, and the perception level of
mental health services for the elderly on the utilization of such services. The fit of the model was assessed using the chi-square goodness of fit statistic and significance, and the explanatory power of the model was measured by the Nagelkerke R². The effects of each factor on the decision to use mental health services for the elderly were analyzed by the regression coefficient(B), significance, and odds ratio [Exp(B)].
Ⅳ. Study Result
1. General Characteristics of the Study Subject
The subjects of this study were the family carer of the elderly with mental health problems. The general characteristics of the subjects were as follow. First, 57.3% of the subjects were female, slightly surpassing the Table 1. Definition and Measurement of Variables
Variable Operational definition Attribute
Dependent
variable The elderly’s utilization of
mental health services Experience of using community institutions
providing mental health services for the elderly1 = have experience 0 = no experience
Independent variables
Characteri stics of the elderly cared for
Gender Gender of the elderly patient 1 = male, 0 = female
Age Age of the elderly patient Ratio variable
Educational level Highest educational level of the elderly patient From no education to college graduate or higher (6 levels), ordinal variable Long-term care
insurance level Long-term care insurance level of the elderly
patient Long-term care insurance levels (1~5), not belonging
to any level, no level (Level 7), ordinal variable
Characteri stics of f a m i l y carers
Gender Gender of the family carer 1 = male, 0 = female
Age Age of the family carer Ratio variable
Educational level Highest educational level of the family carer From no education to college graduate or higher (6 levels), ordinal variable Marital status Spouse of the family carer 1 = married
0 = single Subjective health
conditions Subjectively perceived health conditions 5-point Likert scale Economic status Subjectively perceived household economic status 5-point Likert scale Period of care Period for which the family carer has taken care
of the elderly Total period in months
Care stress Stress that the family carer feels taking care of
the elderly Mean value of the ratings of 12 statements (4-point scale) about care stress
Understanding of geriatric
mental illness Understanding of the normal symptoms of ageing and those of geriatric mental illness
Total value of the ratings of 12 statements (1, 0) about the normal symptoms of ageing and those of geriatric mental illness
Perception level of mental
health services for the elderlyPerception level of mental health services for
the elderly provided by community institutionsTotal value of ratings of the perception (1, 0) of 11 community mental health service providers
male group number, which accounted for 42.7%. About 87% of the subjects had a spouse and 13% were single by virtue of being unmarried, bereaved, or divorced. The ages of the subjects ranged from less than 30 years to their 70s or older: 14.1% less than 30 years, 40%
in their 40s, 31.9% in their 50s, 10.2% in their 60s, and 3.8% in their 70s or older. The average age of the subjects was 49.5 years. With respect to the educational level, 6.5% of the subjects had, at most, attended or graduated from middle-school, while 28.7% were high school graduates, 53.1% were college graduates, and 11.7% were holders of a master's degree or higher. In summary, over two-thirds of the family carers were college graduates or higher.
The characteristics of the elderly cared for by the family carers were as follow. First, the most common disease identified through a multiple-response item was depression(35.5%), followed by dementia(33.9%), sleep disorders(22.6%), chronic mental illness(3.6%), alcoholism(2.4%), and suicidal attempts(2%). As for long-term care status level, 4.4% were classified into Level 1, 6% into Level 2, 12.1%
into Level 3, 9.2% in Level 4, and 3.5% in Level 5. About 5.4% of the subjects did not belong to any level but were able to use the local government's elderly care services, and 59.4%
were not covered by the current long-term care insurance level system. The age of the elderly who were cared for ranged from their 60s to their 90s or older: 19.1% in their 60s, 43.1% in their 70s, 30% in their 80s, and 7.8% in their 90s or older. Their average age was 76.9 years. With respect to gender, 38.2% of the elderly were men and 61.8% were women, who doubled the number of men.
2. Symptoms that Caused the Family Carers to Suspect Mental Illness in the Elderly Patients
The most prominent symptom that caused the family carers to suspect mental illness in the elderly was memory decline(37.9%), which was followed by other forms of cognitive function decline(19.9%). More than half of the family carers(57.8%) suspected mental illness in the elderly patients due to their deterioration of memory and cognitive functions. Other major symptoms included changes in appetite/ eating habits(10.6%), depression/discouragement(8.7%), neurobehavioral symptoms(6.8%), and difficulties in daily living(3.9%). Other symptoms mentioned by fewer respondents were sleep disorders/nocturnal behaviors(3.2%), others(3.2%), anxiety(2.3%), delusions/
persecution complexes (2.3%). and anxiousness /aggression(1.3%). There were also the respondents who reported no particular symptoms(2.2%), digestive disorders rather than mental disorders(0.6%), and head/hand tremor (0.3%). Memory or cognitive function decline in the elderly can be easily accepted as general symptoms of ageing. However, a sudden decrease in memory and cognitive functions that is perceivable by family carers require attention and care.
Table 2. Major Symptoms of Suspected Mental Illness
Unit: person, %Major symptom Frequ
ency Percent age
Memory decline 118 37.9
Other forms of cognitive function decline 62 19.9 Changes in appetite/eating habits 33 10.6
Depression/discouragement 27 8.7
Neurobehavioral symptoms 21 6.8
Difficulties in daily living 12 3.9
Others 10 3.2
Sleep disorders/nocturnal behaviors 10 3.2
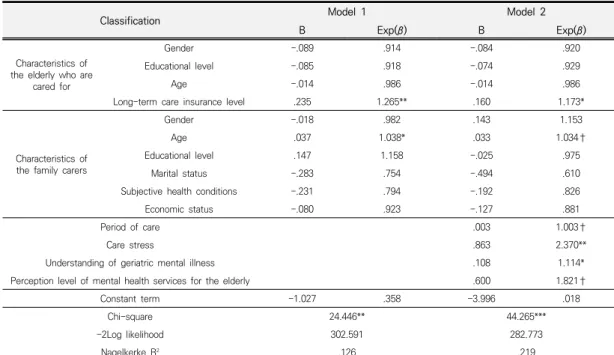
3. Determinants of the Utilization of Elderly Mental Health Services
A binary logistic regression analysis was performed to identify the determinants of the use of mental health services for the elderly.
The analysis was performed by using a hierarchical method of putting the sociodemographic characteristics of the elderly and their family carers, the period of care, care stress, the understanding of elderly mental illness, and the perception level of mental health services for the elderly into the models in two steps. Only the characteristics of the elderly who were cared for and the family
carers were put in Model 1, which showed that the long-term care insurance level of the elderly(B=.235, p<.01) and the age of the family carer(B=.037, p<.05) impacted the elderly’s utilization of mental health services.
The fit of Model 2, which is Model 1 where independent variables, such as the period of care, care stress, the understanding on geriatric mental illness, and the perception level of mental health services for the elderly were put, was also verified with the values of the –2Log likelihood and Chi-square(χ²), which were 282.773 and 44.265, respectively(p<.001). The explanatory power of Model 2 verified by the Nagelkerke R²was 21.9%.
As a result, the determinants of the utilization of mental health services for the elderly were identified as follow: the long-term care insurance level of the elderly (B=.160, p<.05),
Anxiety 7 2.3
Delusions/persecution complexes 7 2.3
Anxiousness/aggression 4 1.3
Total 311 100
Table 3. Determinants of the Utilization of Elderly Mental Health Services
Classification Model 1 Model 2
B Exp(β) B Exp(β)
Characteristics of the elderly who are
cared for
Gender -.089 .914 -.084 .920
Educational level -.085 .918 -.074 .929
Age -.014 .986 -.014 .986
Long-term care insurance level .235 1.265** .160 1.173*
Characteristics of the family carers
Gender -.018 .982 .143 1.153
Age .037 1.038* .033 1.034†
Educational level .147 1.158 -.025 .975
Marital status -.283 .754 -.494 .610
Subjective health conditions -.231 .794 -.192 .826
Economic status -.080 .923 -.127 .881
Period of care .003 1.003†
Care stress .863 2.370**
Understanding of geriatric mental illness .108 1.114*
Perception level of mental health services for the elderly .600 1.821†
Constant term -1.027 .358 -3.996 .018
Chi-square 24.446** 44.265***
-2Log likelihood 302.591 282.773
Nagelkerke R² .126 .219
†p<.10, *p< .05, **p< .01.
Note: The criterion variable of the dummy variables, such as the gender of the elderly, the gender of the family carer, and marital status, is a man with a spouse.
the age of the family carer(B=.033, p<.10), the period of care(B=.003, p<.10), the level of care stress felt by the family carer(B=.863, p<.01), and the carer’s understanding of geriatric mental illness(B=.108, p<.05) and perception level of mental health services for the elderly provided by the community(B=.600, p<.10).
Ⅴ. Conclusions and Implications
This study conducted a survey on the family carers who take care of the elderly who have mental health problems and are living in regional communities. The study investigated how these carers detect mental illness in the elderly and intended to identify the major factors determining the elderly’s utilization of mental health services provided by their communities.
Firstly, the most prominent symptoms that caused the family carers to suspect mental illness in the elderly were memory decline(37.9%) and other forms of cognitive function decline(19.9%). The family carers also detected mental illness in the elderly patients through such symptoms as changes in appetite/eating habits(10.6%), depression /discouragement(8.7%), neurobehavioral symptoms(6.8%), and difficulties in daily living(3.9%). Symptoms like memory decline or cognitive function decline, depression, appetite loss, and sleep disorders can be easily perceived as the general symptoms of ageing that most people experience when they get old[26].
Accordingly, there seems to be a need for education that helps family carers enhance their understanding of the elderly and the ageing process. This education should help
family carers distinguish between normal and pathological ageing symptoms. In other words, it provides family carers with information such as the elderly mental illness, treatment of mental illness, cure information, and local elderly mental health service providers.
Education and information on the mental illnesses of the elderly can reduce the cases that do not lead to treatment.
Secondly, the factors affecting the elderly's mental health service utilization were identified as follow: the elderly's long-term care insurance level the age of the family carer, period of care, care stress felt by the carer, his understanding of geriatric mental illness, and the perception level of community mental health services for the elderly. First, the higher the long-term care insurance level was, the worse the health conditions of the elderly were. Therefore, the elderly seem to satisfy the needs that cannot be met by themselves or with family support through public mental health services.
Therefore, many aged people living in the
community receive care from their spouses
rather than from their children. In this case,
since the life expectancy of the female elderly
is higher than that of the male elderly, female
spouses are more likely to take care of their
male spouses. In addition, the higher the age of
the spouses is, the more difficult it is for them
to care of the patients. This observation seems
to suggest that the elderly spouses are
influenced to seek community mental health
services for the elderly. Meanwhile, a longer
period of care indicates that it has been long
time since the elderly patients showed the
symptoms of mental illness. This suggests that
the elderly who have been cared for over a
longer period of time are in worse conditions
than those who have been cared for over a shorter period of time. In addition, family carers are more likely to use various community support services if they have a higher level of care stress. The period of care and level of care stress were found to be positively correlated in several preceding studies. The longer the period of care was, the worse the elderly patients' conditions and the higher the level of care stress in their family carers were[27-29].
The understanding of geriatric mental illness in family carers was found to affect the elderly's use of mental health services. If family carers have knowledge about the symptoms of geriatric mental illness, they perceive them as those of a pathological nature and seek community mental health services. According to the above presented frequency analysis, about half of the family carers surveyed accepted the symptoms of geriatric mental illness as part of the natural ageing process that can be experienced by all aged people. If family carers who observe the elderly patients most closely have a proper understanding of geriatric mental illness and its symptoms, they can better recognize mental diseases in the elderly patients when such symptoms are manifested and take measures for early treatment. Thus, it is considered that education and information provision on geriatric mental illness will reduce the number of cases where the detection of geriatric mental illness symptoms does not lead to treatment.
The higher the perception level of mental health services for the elderly is, the higher the probability of using community mental health services among the elderly will be. In the study by Lee et al. (2010), the perception level of mental health services for the elderly influenced
the intention to use such services[20].
Moreover, in the study by Lim and Yun (2009), the perception level of the services impacted the utilization of the services[30]. Thus, it is imperative that mental health services that can meet the needs of the elderly patients and the family carers who look after them in the community become available. Then, family carers must be educated about the available services and detailed programs to utilize such facilities. In Korea, mental health service delivery system for the elderly is very complicated. Depending on the type of diseases, services are provided through a complex process where both health and welfare authorities are involved, which indicates the lack of linkage and cooperation between the two sectors. Therefore, it is necessary to improve the delivery system so that elderly people with mental health problems can easily access medical/welfare services in the early stage of the detection of such symptoms. In this sense, it is suggested that information on mental health service institutions currently operating in regional communities be actively shared to the public and the primary registration of the elderly with mental health problems be made no matter which institution they visit. The registered elderly patients should be referred to the most suitable institutions according to their diseases and symptoms by the registration institutions for treatment and follow-up management, as part of efforts to provide continuous services to consumers and to increase service accessibility.
The academic significance of this study lies in
its investigation of the major symptoms that
help family carers detect mental illness in
elderly patients and the initial countermeasures
that they take to cope with these symptoms.
The study also identified the reasons why the detection of the symptoms does not lead to treatment of mental illness and empirically verified the major factors determining the elderly's utilization of mental health services based on a survey on family carers.
Nevertheless, there are limitations in interpreting and generalizing the results of this study for all the cases of family carers as the data used in the analyses were collected through the significant sampling method among the family carers living in some urban areas.
Therefore, it is suggested that follow up studies expand the study subjects to family carers living in various areas.
참 고 문 헌
[1] Health Insurance Review & Assessment Service,
National Health Insurance Service,National Health Insurance Statistical Yearbook, 2016.
[2] Ministry of Health and Welfare, “The Elderly Aged over 70 Suffering Panic Disorders Causing Deadly Fear Increases by 3.4 Times,”
News release on March 19, 2017.
[3] G. H. Jeong,
The 2014 National Survey on Aged Population,Korea Institute for Health and Social Affairs, 2014.
[4] Korea Ranks First Among OECD Countries in Suicide Rate (2017, November 11), Sejong Economy News, Retrieved from http://www.seenews365.com/
[5] National Institute of Dementia.
The 2016 National State of Dementia Patients,National Institute of Dementia, 2016.
[6] J. P. Hong,
The Survey of Mental Disorders in Korea,Ministry of Health and Welfare, 2016.
[7] D. U. Lee, S. H. Yu, and S. J. Cho, “The
Development of Community-Based Elderly Mental Health Care Mode,” Report on Research Entrusted by the National Mental Health Center Research Center, pp.1-148, 2009.
[8] N. C. Kim, J. H. Kim, and Y. M. Lim, “A Study on Community-dwelling Elders with Dementia, their Primary Caregiver, and Living Environments,” The Journal of Korea Community Health Nursing Academic Society, Vol.16, No.1, pp.13-29, 2002.
[9] Y. H. Park, “Family Caregivers' Stress of the Old Adults,” Stress, Vol.15, No.4, pp.331-337, 2007.
[10] Y. O. Gwak, Y. S. Kim, and G. H. Seo, “Factors of Stress Responses and Quality of Life among Stroke Patients' Family Caregivers: Focused on ADL and Social Supports,” The Korean Journal of Stress Research, Vol.16, No.3, pp.261-269, 2008.
[11] G. H. Seo and G. I. Cheon, “The Moderating Effect of Social Support on Family Caregivers' Burdens and Health and Quality of Life While Taking Care of Demented Patients,” The Korean Journal of Culture and Social Issues, Vol.15, No.3, pp.339-357, 2009.
[12] M. S. Jeon, “Effects of the Characteristics of the Elderly and Family Caregivers on the Caregiving Stresses,” The Journal of the Korea Contents Association, Vol.14, No.12, pp.274-282, 2014.
[13] S. Y. Kwon, H. J. Lee, and J. Y. Lee, “The Effects of Care Hours on the Burden Placed on the Family Caregiver with regard to the Elderly with Dementia-Focusing on the Moderating Effects of the Attachment,” Journal of Social Science, Vol.31, No.2015.2, pp.317-337, 2015.
[14] H. S. Yoon, “Factors Affecting the Intention and Necessity to Use Home Welfare Services in Family Carers of Elderly Patients,” Journal of the Korea Gerontological Society, Vol.21, pp.141-161, 2001.
[15] G. O. Lee and M. J. Lee, “A Study on Older
Adults' Utilization Determinants of Community Care Services,” Journal of the Korea Gerontological Society, Vol.21, pp.113-124, 2001.
[16] D. Y. Song, “A Study on Factors Affecting the Intention of Family Caregivers to Use Home Welfare Services,” Korean Journal of Social Welfare, Vol.53, No.5, pp.105-128, 2003.
[17] E. Y. Kim, E. S. Nam, Y. R. Chae, and H. K.
Lee, “Factors Affecting the Elderly's Preference for Utilization of Long-Term Care Services Based on Andersen's Behavioral Model,”
Journal of the Korea Gerontological Society, Vol.28, No.3, pp.585-602, 2008.
[18] C. J. Park and B. M. Yang, “Determinants of Hospital Care Choice of Family with the Demented Elderly,” Journal of Welfare for the Aged Institute, Vol.41, pp.79-102, 2008.
[19] C. J. Park, “Determinants of Long Term Care Service Use of Family Caregiver,” Journal of Community Welfare, Vol.33, pp.69-92, 2010.
[20] G. Y. Lee, S. S. Choi, H. S. Park, and H. J. Lim,
“A Study of Factors Affecting on the Preference of the elderly's Mental Health Services Utilization in Rural Areas-Application of Andersen and Newman's Model,” Korean Journal of Social Welfare, Vol.62, No.2, pp.257-278, 2010.
[21] J. B. Neese, I. L. Abraham, and K. C.
Buckwalter, “Utilization of mental health services among rural elderly,” Archives of Psychiatric Nursing, Vol.13, No.1, pp.30-40, 1999.
[22] F. Amaddeo and J. Jones, “What is the impact of socio-economic inequalities on the use of mental health services?,” Epidemiologia e Psichiatria Sociale, Vol.16, pp.16-19, 2007.
[23] V. Donisi, F. Tedeschi, M. Percudani, A.
Fiorillo, L. Confalonieri, C. De Rosa, D.
Salazzari, M. Tansella, G. Thornicroft, and F.
Amaddeo, “Prediction of community mental health service utilization by individual and ecological level socio-economic factors,”
Psychiatry research, Vol.209, No.3, pp.691-698, 2013.
[24] J. Volkert, S. Andreas, M. Härter, M. C.
Dehoust, S. Sehner, A. Suling, B. Ausín, A.
Canuto, M. J. Crawford, C. Da Ronch, L. Grassi, Y. Hershkovitz, M. Muñoz, A. Quirk, O.
Rotenstein, A. B. Santos-Olmo, A. Y. Shalev, J.
Strehle, K. Weber, K. Wegscheider, H. U.
Wittchen, and H. Schulz, “Predisposing, enabling, and need factors of service utilization in the elderly with mental health problems,” International psychogeriatrics, Vol.30, No.7, pp.1027-1037, 2018.
[25] C. Guo, N. Li, G. Chen, and X. Zheng, “Mental health service utilization and its associated social factors among elderly people with a mental disability in China: A national population-based survey,” Scandinavian journal of public health, Vol.47, No.2, pp.215-220, 2017.
[26] J. Y. Park, “Characteristics of Elderly Mental Health and Clinical Intervention,” The proceedings of the Korea Academy of Mental Health Social Work Symposium, pp.363-386, 2004.
[27] E. P. Stoller and K. L. Pugliesi, “Other roles of caregivers: Competing responsibilities or supportive resources,” Journal of Gerontology, Vol.44, No.6, pp.S231-S238, 1989.
[28] Y. H. Yang, “The Relationship among the Care Conditions of Family Members Caring for Chronic Patients, Stress and Social Support,”
Korean Journal of Adult Nursing, Vol.7, No.1, pp.85-105, 1995.
[29] Y. R. Kim, “Analysis on Factors Affecting Elderly Care work Hours and Stresses in Care work among Family Caregivers,” Journal of Women’s Studies, Vol.72, pp.31-72, 2007.
[30] Y. O. Lim and H. S. Yoon. "Longitudinal Study
on Factors Affecting Older Adults` Welfare
Service Utilization," Journal of the Korea
Gerontological Society, Vol.29, pp.1063-1085,
2009.
저 자 소 개
박 경 순(Kyungsoon Park) 정회원
▪ 1998년 8월 : 광주대학교 신문방송 학과(학사)
▪ 2010년 2월 : 강남대학교 사회복지 학과(석사)
▪ 2013년 6월 : 강남대학교 사회복지 학과(박사)
▪ 2014년 9월 ~ 현재 : 연세대학교 고령화융복합연구센터 전임연구원
<관심분야> : 노인복지, 노인장기요양, 커뮤니티케어
박 영 란(Yeong-ran Park) 정회원
▪ 1984년 2월 : 연세대학교 신문방송 학과(학사)
▪ 1988년 2월 : 연세대학교 사회사업 학과(석사)
▪ 1995년 6월 : University of Washington (박사)
▪ 1996년 6월 ~ 2004년 2월 : 여성 개발원
▪ 2014년 3월 ~ 현재 : 강남대학교 실버산업학과/사회복지 학과 겸직 교수
<관심분야> : 노인복지, 실버산업, 노인장기요양
손 덕 순(Duksoon Son) 정회원
▪ 1996년 2월 : 광주대학교 사회복지 학과(학사)
▪ 1998년 8월 : 강남대학교 대학원사 회사업학과(석사)
▪ 2005년 8월 : 강남대학교 대학원 사회사업학과(박사)
▪ 2007년 2월 ~ 2008년 8월 : 재)경 기도가족여성연구원 정책개발실 연구위원
▪ 2008년 9월 ~ 현재 : 용인송담대학교 사회복지과 교수 <관심분야> : 노인복지, 정신건강사회복지
염 유 식(Yoosik Yum) 정회원