대한외과학회지:제 72 권 제 6 호
□ 증 례 □
Vol. 72, No. 6, June, 2007
서 론
성인형 스틸씨 병은 고열, 관절통, 발진 등의 임상 증상을 보이나 원인은 미상인 만성 전신염증질환이다. 간기능 부 전, 심장 눌림증, 파종성 혈관 내 응고, 호흡 곤란 증후군, 온혈구감소증(pancytopenia) 등의 생명에 위험을 줄 수 있는 식혈세포성 증후군이 종종 성인형 스틸씨 병에서 발생한 다.(1-4) 식혈세포성 증후군을 동반한 성인형 스틸씨 병은 조기 진단과 즉각적인 치료를 시행하지 않으면 환자는 치 명적인 상황에 이를 수 있다. 식혈세포성 증후군의 발현은 종종 패혈증으로 오인될 수 있으며, 패혈증의 일반적 치료 에 반응하지 않는다. 패혈증의 일반적 치료에 반응이 없을 때 성인형 스틸씨 병에 대한 의심을 한 번은 가져야 한다.
저자들은 급성 비결석 담낭염으로 복강경하 담낭절제술 후 발생한 성인형 스틸씨 병 1예를 경험하여 이에 문헌 고 찰과 함께 보고하고자 한다.
증 례
41세의 여자 환자가 3일간의 우상복부 통증과 고열을 주 소로 내원하였다. 과거력상 2년 전 폐렴으로 입원한 기왕력 이 있었다. 말초 혈액 검사상 백혈구 11,830/mm3 (중성구;
95%), 혈색소 12.1 g/dl, 헤마토크리트 37.2%, 혈소판 49,000/
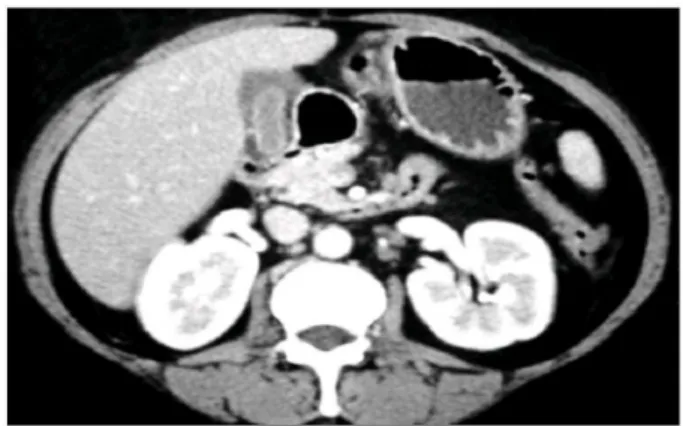
mm3, 혈액 화학 검사상 AST/ALT 275/316 IU/L, ALP 937 IU/L, T.Bil 1.2 mg/dl, HBs Ag/Ab -/+이었다. 복부 컴퓨터 단층 촬영상 비결석성 담낭염이 의심되어 복강경하 담낭절 제술을 시행하였다(Fig. 1). 수술 소견 시 심한 지방간의 소 견을 보였고 담낭의 벽은 비후되어 있었으며 또한 주위 조 직과 심한 유착을 보이고 있었다. 수술 후 환자는 특별한 합병증은 발생하지 않았고 수술 후 실시한 말초 혈액 검사 와 혈액 화학 검사상 정상 소견을 보여 수술 후 4일째 퇴원 하였다. 환자는 수술 후 27일째 다시 내원 2일 전부터 시작 된 고열, 관절통, 발진을 주소로 입원하였으며 말초 혈액 검 사상 백혈구 35,830/mm3(중성구; 87%), 혈색소 10.8 g/dl, 헤 마토크리트 34.1%, 혈소판 134,000/mm3였다. ESR 22 mm/hr, CRP 5.98 mg/dl, 혈액 화학 검사상 AST/ALT 393/686 IU/L, PT 66.2%, Total Protein/Albumin 4.7/2.1 g/dl, T.Bil 0.6 mg/dl,
담즙성 복막염으로 오인할 수 있는 성인형 스틸씨 병
포천중문의과대학교 외과학교실
한상문·김원우·정철운·이경포·이경식
책임저자:한상문, 서울시 강남구 역삼 1동 650-9
ꂕ 135-081, 포천중문의과대학교 강남차병원 외과 Tel: 02-3468-3369, Fax: 02-3468-3509
E-mail: [email protected]
접수일:2006년 11월 24일, 게재승인일:2007년 2월 12일
Adult Onset Still’s Disease Misunderstood as Sepsis with Bile Peritonitis
Sang Moon Han, M.D., Won Woo Kim, M.D., Chul Woon Chung, M.D., Kyung Po Lee, M.D. and Kyung Sik Lee, M.D.
Adult onset Still's disease (AOSD) is a rare systemic inflam- matory disorder of an unknown etiology, and its major clini- cal manifestations include high spiking fever, polyarthralgia, salmon-colored evanescent rash and neutrophilic leuko- cytosis. We describe here a 41 year old woman with AOSD who presented with non-remitting high fever, polyarthralgia, sore throat, skin rash, splenomegaly, thrombocytopenia, neutrophilic leukocytosis, hyperferritinemia and coagulopathy with disseminated intravascular coagulation (DIC). The patient had a history of laparoscopic cholecystectomy due to acalculous cholecystitis prior to admission. We suspected sepsis due to bile peritonitis after the previous laparoscopic cholecystectomy. Yet we could not detect infectious orga- nisms on the cultures or serologic studies. Finally, we sus- pected AOSD-associated hemophagocytic syndrome (HS). So, intravenous immunoglobulin and pulse methylprednisolone treatment brought about transient improvement of the fever and the neutrophilic leukocytosis, but the disease progressed and the patient expired due to acute renal failure. HS is a fatal cause of AOSD. If a patient has DIC and sepsis and these fail to respond to conservative treatment, then AOSD should be added to the differential diagnosis of sepsis and DIC. (J Korean Surg Soc 2007;72:505-508)
Key Words: Disseminated intravascular coagulation, Sep- sis, Hemophagocytic syndrome, Adult onset Still's disease
중심 단어: 파종성 혈관 내 응고, 패혈증, 식혈세포 성 증후군, 성인형 스틸씨 병
Department of Surgery, College of Medicine, Pochon CHA University, Seongnam, Korea
505
506 대한외과학회지:제 72 권 제 6 호 2007
Ferritin 1,650 ng/ml, FDP 80μg/ml, Fibrinogen 166 mg/dl, D-Dimer 5,474 ng/ml이었다. Direct/ Indirect Coombs' test -/
-, HBs Ag/Ab -/+, HBc Ab+였으며 dsDNA cardiolipin, VDRL, rheumatoid factor에 대한 항체 검사는 음성이었다.
복부 컴퓨터 단층 촬영상 간 종대와 비장종대의 소견이 보 였고(Fig. 2), 간밑오목(subhepatic fossa)에 복수가 고여 있었 으며, 창자간막임프절 종대의 소견이 보였다. 피부의 발진 에서 실시한 조직 검사는 표재성 세정맥 주위에 림프구 침 윤의 소견을 보이고 있었다. 담낭 수술 발생한 담즙 누출성 복막염에 의한 패혈증 상태가 의심되어 복수 천자와 DISIDA 핵 조영술이 시행되었다. 복수에서 시행된 미생물 검사상 세균은 발견되지 않았으며 DISIDA 핵 조영술에서 도 뚜렷한 담즙 누출 소견은 보이지 않았다(Fig. 3). 수술 후 37일째 환자의 상태는 악화되어 정신 혼동 상태를 보였으 며 백혈구 14,920/mm3(중성구; 87%), 혈색소 9.1 g/dl, 헤마 토크리트 29.3%, 혈소판 35,000/mm3였다. ESR 22 mm/hr,
CRP 4.54 mg/dl, 혈액 화학 검사상 AST/ALT 1,248/ 551, PT 17%, Total Protein/Albumin 5.8/2.5 g/dl, T.Bil 11.1 mg/dl, Ferritin 13,802 ng/ml, FDP 20μg/ml, Fibrinogen 185 mg/dl, D-Dimer 5,420 ng/ml였다. 류마티스과에 진료 의뢰되어 환 자는 성인형 스틸씨 병의 진단하에 스테로이드와 면역 글 로불린이 투여되었으며 백혈구 수치, AST/ ALT는 정상 수 치로 감소하였으며 정신 상태도 호전되었다. 환자의 임상 경과에 따른 검사실 수치는 Table 1에 표시하였다. 그러나, 환자는 계속적인 빌리루빈의 증가를 보여 수술 후 57일째 급성 신부전으로 사망하였다.
고 찰
스틸씨 병은 류마티스양 관절염의 이형 질환으로 1896년 Still(5)에 의하여 처음으로 보고되었으며 1971년에 Bywaters(6) 는 성인형 스틸씨 병을 보고하였다. 성인형 스틸씨 병은 Magadur-Joly 등(7)에 의하면 인구 100,000명당 0.16에서 발 생하는 매우 드문 질환으로 원인은 아직 정확히 밝혀지지 않은 전신성 염증 질환이다.
소아 스틸씨 병은 3∼5세 사이에 장막염, 림프절병증, 간 기능 이상을 동반하는 전신 질환으로 발생하고, 성인형은 16∼35세에 발생하며(8) 관절염, 발진, 열, 호중구 증가를 보 인다. 특징적인 혈청학적 이상 소견이 없고, 특별한 원인 인 자가 없는 이유로 많은 진단 기준이 제안되었지만 현재 Yamaguchi와 Ohta(9)가 제안한 진단 기준이 사용되고 있다 (Table 2). 저자들의 환자는 고열, 관절통, 발진, 백혈구 증가 증, 인후통, 비장종대, 간기능 이상, 류마티스 인자 음성으 로 Yamaguchi가 제안한 진단 기준에 모두 합당한 소견을 보였다.
식혈세포성 증후군은 세망내피계통을 통한 조직구의 과 도한 증식과 식혈 작용을 특징으로 하는 드문 질환이며 과 도하게 활성화된 T 세포와 큰 포식세포, IL-1, IL-6, IFN-γ Fig. 1. Computed tomographic findings of abdomen showing acal-
culous cholecystitis (A thick wall of gall bladder with peri- cholecystic fluid collection).
Fig. 2. Computed tomographic findings of abdomen showing severe hepatosplenomegaly.
Fig. 3. DISIDA scan shows no main duct bile leakage of the patient.
한상문 외:담즙성 복막염으로 오인할 수 있는 성인형 스틸씨 병 507
와 같은 사이토카인의 과형성 등이 원인으로 제기되고 있 다.(10) 이러한 식혈세포성 증후군의 특징적인 임상적 증상 및 검사실 소견은 계속되는 고열, 정신상태의 변화, 간비장 종대, 장막염, 혈구 감소증, 아미노전이효소의 증가, 고빌리 루빈혈증, 락트산탈수소효소(lactic acid dehydrogenase)의 증 가, 프로트롬빈 시간과 활성화부분트롬보플라스틴시간의 증가를 보이는 소모응고병증, 저섬유소원혈증(hypofibrino- genemia), 섬유소원분해산물(fibrinogen degradation products) 의 출현, 고페리틴혈증(hyperferritinemia) 등을 보이며 임상 적 증상과 검사실 이상 소견이 면역 억제 치료에 의해 완전 관해를 보일 때 식혈세포성 증후군의 진단을 고려할 수 있 다.(10-13) 식혈세포성 증후군은 종종 진단과 치료가 늦어 지게 된다. 저자들의 환자에서도 담즙성 복막염에 의한 패 혈증을 의심하였으며 초기 치료의 지연을 가져왔다. 고페 리틴혈증은 식혈세포성 증후군의 진단과 성인형 스틸씨 병 의 활성도를 나타내는 중요한 특징적 소견이다. 식혈세포
성 증후군의 환자는 1,000∼250,000 ng/ml의 페리틴 농도를 보이며(14,15) 저자들의 환자에서도 입원 당시 1,650 ng/ml 인 페리틴 농도가 환자의 상태가 악화되어 정신 혼돈 상태 를 보일 때 13,802 ng/ml까지 증가하였다.
심한 성인형 스틸씨 병이나 식혈세포성 증후군 시 종종 급성 복통을 동반하는데, 복막의 염증, 장간막 림프절 병증, 기능상 장폐색 등이 원인이 된다.(8) 급성 장막염에 의한 비 결석성 담남염이 종종 발생하는데 저자들의 환자에서도 비 결석성 담낭염으로 복강경하 담낭절제술을 시행 받았다.
비결석성 담낭염의 유발인자는 심한 외상이나 대수술, 심 한 화상, 장기간 비경구 영양 요법과 인공호흡기 사용, 대량 의 수혈, 대량의 진정제 복용, 혈관 질환 등이 있는데 주로 만성형보다는 급성형 비결석성 담낭염의 유발인자로 알려 져 있다.(16) 그러나, 현재 유발 인자를 발견할 수 없는 경우 가 더 많아, 안 등(17)은 비결석성 담낭염의 52%, 고 등(18) 도 71.4%에서 유발 인자를 알 수 없다고 보고하였다. 유발 인자를 모르는 질환 중 전신 염증 질환인 성인형 스틸씨 병이 하나의 원인으로 보고되고 있다.(4)
성인형 스틸씨 병은 급성, 자기 한정적, 재발, 만성 등의 다양한 과정을 보이며 치료가 어렵다. 일반적으로 1차 치료 약물로 비스테로이드성 항염증 약물과 고용량 스테로이드 가 사용되며, 1차 약물에 저항하는 경우 methotrexate, cyclo- sporine, cyclophosphamide 등이 사용된다.(19-21) 또한 Infli- ximab의 투여에 의한 치료도 보고되고 있다.(22,23)
성인형 스틸씨 병은 매우 드문 질환으로 진단이 어렵다.
식혈세포성 증후군 동반 시 더욱 더 진단은 어려워진다. 그 러나, 계속되는 고열, 혈관 내 파종성 응고장애, 패혈증 등 의 의심 상황에서 대증적인 치료 실패 시, 꼭 한 번은 성인 형 스틸씨 병을 염두에 두어야 할 것이다. 성인형 스틸씨 Table 1. Finding of the patient before and after laparoscopic cholecystectomy
Postoperative days (laparoscopic cholecystectomy)
40 (pulse steroid+
-4 (Preop) 3 (Post LC) 27 (Readmission) 37 (Mental change)
immunoglobulin)
WBC (mm3) 11,830 8,960 35,830 14,920 3,410
Hg (g/dl) 12.1 10.0 10.8 9.1 10.1
Platelet (mm3) 49,000 222,000 134,000 35,000 29,000
ESR (mm/hr) 14 16 22 22 16
AST/ALT (IU/L) 275/316 21/68 393/686 1,248/551 265/328
T. Bil (mg/dl) 1.2 0.4 0.6 11.1 20.1
T.P/Alb (g/dl) 6.1/3.3 5.6/3.0 4.7/2.1 5.8/2.5 6.7/3.0
Fibrinogen (mg/dl) 166 185 212
FDP (μg/ml) 80 20 10
D-dimer (ng/ml) 5,474 5,420
Ferritin (ng/ml) 1,650 13,802 3,193
Table 2. Diagnostic criteria on adult Still's disease Major criteria Intermittent high fever
Arthralgia Typical rash Leukocytosis Minor criteria Sore throat
Lymphadenopathy and/or splenomegaly Liver dysfunction
Negative rheumatoid factor and antinuclear antibody Diagnosis: Five or more criteria, including 2 major ones.
508 대한외과학회지:제 72 권 제 6 호 2007
병은 조기 진단과 치료가 중요하며 진단이 지연됨으로써 발생하는 합병증을 예방하기 위해 더욱 더 관심을 가져야 할 것으로 생각된다.
REFERENCES
1) Yokoyama M, Suwa A, Shinozawa T, Fujii T, Mimori T, Akizuki M, et al. A case of adult onset Still's disease complicated with adult respiratory distress syndrome and disseminated intravascular coagulation. Nihon Rinsho Meneki Gakkai Kaishi 1995;18:207-14.
2) Takeshita A, Takeuchi T, Nakagawa A, Tsuda Y, Fukuda A, Nariyama K, et al. Adult onset Still's disease with hemopha- gocytic syndrome and severe liver dysfunction. Hepatol Res 2000;17:139-44.
3) Dino O, Provenzano G, Giannuoli G, Sciarrino E, Pouyet M, Pagliaro L. Fulminant hepatic failure in adult onset Still's disease. J Rheumatol 1996;23:784-5.
4) Park JH, Bae JH, Choi YS, Lee HS, Jun JB, Jung S, et al.
Adult-onset Still's disease with disseminated intravascular coagulation and multiple organ dysfunctions dramatically treated with cyclosporine A. J Korean Med Sci 2004;19:137- 41.
5) Still GF. On a form of chronic joint disease in children. Med Chir Trans 1897;80:1-13; reprinted Am J Dis Child 1978;132:
195-200.
6) Bywaters EG. Still's disease in adult. Ann Rheum Dis 1971;
30:121-33.
7) Magadur-Joly G, Billaud E, Barrier JH, Pennec YL, Masson C, Renou P, et al. Epidemiology of adult Still's disease:
estimate of the incidence by a retrospective study in west France. Ann Rheum Dis 1995;54:587-90.
8) Ohta A, Yamaguchi M, Kaneoka H, Nagayoshi T, Hiida M.
Adult Still's disease: review of 228 cases from the literature.
J Rheumatol 1987;14:1139-46.
9) Yamaguchi M, Ohta A. Adult Still's disease. Nippon Naika Zasshi 1991;80:1771-4.
10) Imashuku S. Differential diagnosis of hemophagocytic synd- rome: underlying disorders and selection of the most effective treatment. Int J Hematol 1997;66:135-51.
11) Emmenegger U, Frey U, Reimers A, Fux C, Semela D, Cottagnoud P, et al. Hyperferritinemia as indicator for intra-
venous immunoglobulin treatment in reactive macrophage activation syndromes. Am J Hematol 2001;68:4-10.
12) Emmenegger U, Reimers A, Frey U, Fux Ch, Bihl F, Semela D, et al. Reactive macrophage activation syndrome: a simple screening strategy and its potential in early treatment initiation.
Swiss Med Wkly 2002;132:230-6.
13) Stephan JL, Kone-Paut I, Galambrun C, Mouy R, Bader- Meunier B, Prieur AM. Reactive haemophagocytic syndrome in children with inflammatory disorders. A retrospective study of 24 patients. Rheumatology 2001;40:1285-92.
14) Coffernils M, Soupart A, Pradier O, Feremans W, Neve P, Decaux G. Hyperferritinemia in adult Still's disease and the hemophagocytic syndrome. J Rheumatol 1992;19:1425-7.
15) Kumakura S, Ishikura H, Munemasa S, Adachi T, Murakawa Y, Kobayashi S. Adult onset Still's disease associated hemo- phagocytosis. J Rheumatol 1997;24:1645-8.
16) Richard RB. Acute acalculous cholecystitis. J Clin Gastroen- terology 1992;15:235-8.
17) Ahn BY, Yun YK, Whang YJ. Clinical analysis of acalculous cholecystitis. J Korean Surg Soc 1997;53:579-87.
18) Ko SH, Moon JH, Lee BD. Clinical analysis of cholecystitis:
acalculous cholecystitis compared to calculous cholecystitis. J Korean Surg Soc 2002;62:249-58.
19) Fautrel B, Borget C, Rozenberg S, Meyer O, Le Loet X, Masson C, et al. Corticosteroid sparing effect of low dose methotrexate treatment in adult Still's disease. J Rheumatol 1999;26:373-8.
20) Marchesoni A, Ceravolo GP, Battafarano N, Rossetti A, Tosi S, Fantini F. Cyclosporine A in the treatment of adult onset Still's disease. J Rheumatol 1997;24:1582-7.
21) Chaouat D, Belange G, Gompel H. Efficiency of cyclophos- phamide bolus in Still's disease in adults. A case. Rev Rhum Mal Osteoartic 1992;59:285-7.
22) Maini RN, St Clair EW, Breedveld F, Furst D, Kalden J, Weisman M, et al. Infliximab (chimeric anti-tumour necrosis factor alpha monoclonal antibody) versus placebo in rheuma- toid arthritis patients receiving concomitant methotrexate: a randomized phase III trial. Lancet 1999;354:1932-9.
23) Cavagna L, Caporali R, Epis O, Bobbio-Pallavicini F, Monte- cucco C. Infliximab in the treatment of adult Still's disease refractory to conventional therapy. Clin Exp Rheumatol 2001;
19:329-32.