Application of imputation methods with adjusting multi-center effect on Crohns disease data in Korea †
Hanna Yoo 1
1 Department of Computer Software, Busan University of Foreign Studies
Received 15 January 2018, revised 8 March 2018, accepted 19 March 2018
Abstract
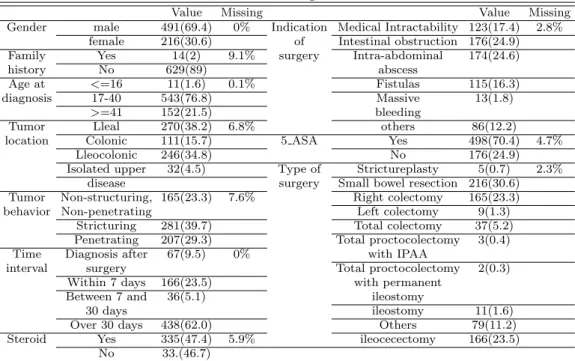
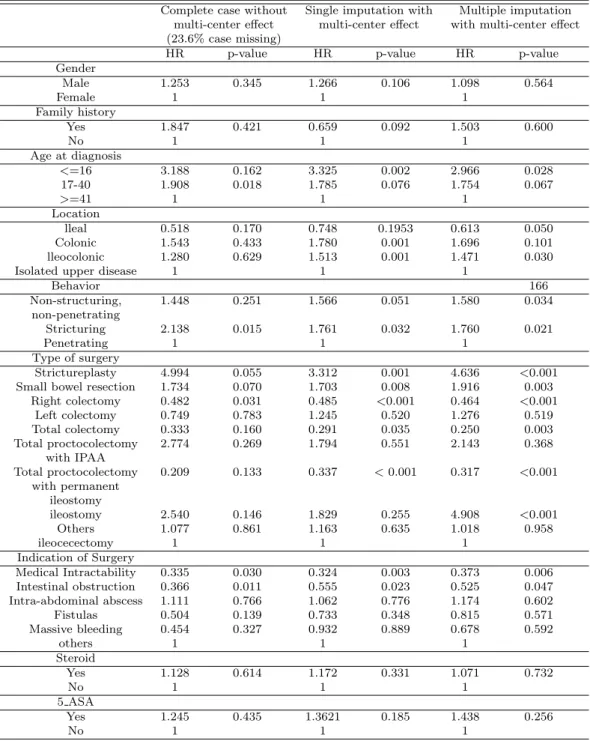
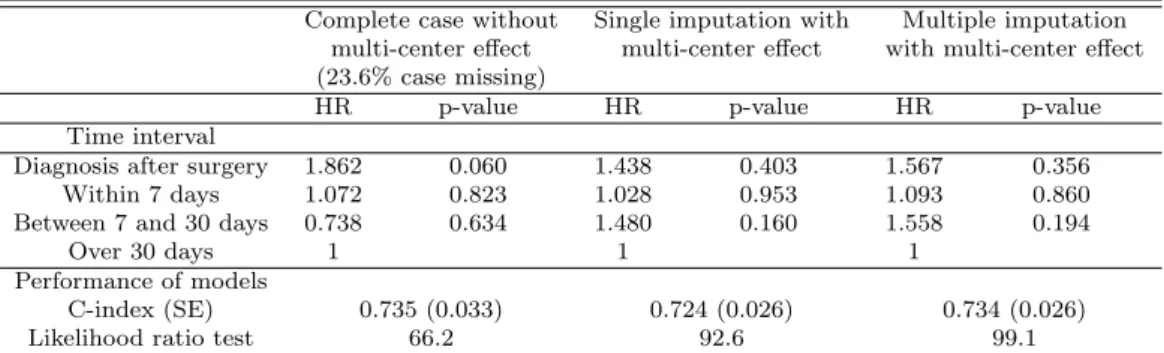
The purpose of this study is to assess the risk factors for recurrence time after the first abdominal surgery in Korean patients with Crohns disease (CD). CD patients who underwent abdominal surgery from January 2000 to December 2009 were collected from seventeen university hospitals (Lee et al. 2012). We assessed the risk factors for recurrence time after the first abdominal surgery CD using Cox regression analysis with imputing the missing covariates using single and multiple imputation methods and also adjusting for the multi-center effect. We compared our results with the complete case analysis. Using imputation methods with considering the multi-center effect, model performance was improved. Comparing between the imputation methods, multiple im- putation method showed better performance than single imputation method.
Keywords: Crohns disease, imputation methods, missing covariates, multi-center effect.
1. Introduction
In many epidemiological studies, missing data is a common problem. For survival data which deals with time to a certain event, censoring occurs due to many reasons (loss to follow up, drop out etc.) and this censoring is what makes survival analysis special and differentiated from other analytical methods. There are many statistical methods considering censoring at the time to event. However few studies have been dealt with missing covariates. Furthermore, when the data is clustered (eg. multi-center data), studies dealing with missing covariates are rare. Burton and Altman (2004) reviewed 100 articles of cancer prognostic studies with missing covariates assessing potential prognostic factors using multivariate survival analysis.
In the review, 81 articles had missing covariates, 15 articles reported complete data and the remaining 4 articles were unknown of the presence of missing covariates. Of the 81 articles that reported missing covariates only 38% mentioned for handling missing covariates.
Complete and available case analysis was the most commonly used methods and three articles used single imputation and multiple imputations were used in only one article. Disregarding
† This work was supported by the research grant of the Busan University of Foreign Studies in 2018.
1