Effects of Isokinetic Strength Exercise of the Hemiparetic Knee Joint on Lower Extremity Sensorimotor and Gait Functions in Patients With
Chronic Stroke: Open Kinetic Chain Versus Closed Kinetic Chain
Chang-man An1, MSc, PT, Jung-suk Roh2, PhD, PT
1Department of Physical Therapy, The Graduate School, Hanseo University
2Department of Physical Therapy, Division of Health Science, Hanseo University
Abstract
1)Background: After stroke, in order to improve gait function, it is necessary to increase the muscle strength and to enhance the propriocetive function of the lower extremity.
Objects: This study aimed to compare the effects of open kinetic chain (OKC) versus closed kinetic chain (CKC) isokinetic exercise of the hemiparetic knee using the isokinetic equipment on lower extremity sensorimotor function and gait ability in patients with chronic stroke.
Methods: Thirty participants with chronic hemiplegia (> 6 months post-stroke) were randomly divided into 2 equal groups: CKC group and OKC group. Patients from both groups attended conventional physiotherapy sessions 3 times a week for 6 weeks. Additionally, subjects from the CKC group performed isokinetic exercise using the CKC attachment, while those from the OKC group performed isokinetic exercise using the OKC attachment. The isokinetic knee and ankle muscles strength, position sense of the knee joint, and spatiotemporal gait parameters were measured before and after interventions.
Results: The knee muscles peak torque/body weight (PT/BW) and hamstring/quadriceps (H/Q) ratio significantly increased in both groups (p<.01). In particular, ankle plantarflexors PT/BW, position sense of the knee, gait velocity, and spatial gait symmetry significantly improved in the CKC group (p<.01, p<.05, p<.01, and p<.01, respectively).
Conclusion: CKC isokinetic exercise can be an effective therapeutic intervention for the improvement of sensorimotor function of the lower extremity and gait functions, such as gait velocity and symmetry.
CKC position in isokinetic strength training is effective to improve functional ability in patients with chronic stroke.
Key Words: Closed kinetic chain; Isokinetic exercise; Knee; Open kinetic chain; Stroke.
Introduction
After stroke, the sensorimotor dysfunction is a prominent clinical features and is known to be one of the main factors in slowing the recovery of func- tions (Cramp et al, 2006; Lin, 2005). Especially, lower extremity muscle weakness and impaired proprio- ception can lead to markedly reduced functional abil- ities, such as normal gait function, in hemiplegic pa- tients (Lin, 2005; Patten et al, 2004). They may have
increased spatiotemporal gait asymmetry and de- creased gait velocity and energy efficiency (Hus et al, 2003; Patterson et al, 2010; Wist et al, 2016). In clinical practice, physical therapy was intended to in- crease muscle strength and enhance proprioceptive function (Bloem et al, 2000; Wist et al, 2016).
Progressive resistive training (PRT) has been known as an effective intervention for muscle strengthening in various musculoskeletal and neuro- muscular diseases (Jan et al, 2009; Wist et al, 2016).
Corresponding author: Jung-suk Roh [email protected]
This research was funded by the Hanseo University research grant (2018).
PRT is generally classified into open kinetic chain (OKC) exercise and closed kinetic chain (CKC) ex- ercise (Stensdotter et al, 2003). OKC exercise are sin- gle joint movements that are performed in non-weight bearing positions with a free distal extremity. In con- trast, CKC exercise are multi-joint movements per- formed in weight bearing or simulated weight bearing postures with a fixed distal extremity (Stensdotter et al, 2003). OKC exercise is a more frequently applied treatment option, because it implies the absence of weight loading, and therefore, is associated with re- duced exercise tolerance and risk of falls (Irish et al, 2010). Nevertheless, CKC exercise is known to better improve the muscle coordination pattern and func- tional status compared to OKC exercise, because of the recruitment of more muscle groups and require- ment of additional skeletal stabilization (Mansfield et al, 2010; Protas et al, 2005; Stensdotter et al, 2003).
In addition, CKC exercise may provide more sensory feedback through multiple joint proprioceptive re- actions (Bloem et al, 2000; Irish et al, 2010).
The isokinetic muscle strengthening represents a potentially interesting physical therapy intervention for patients with stroke. Because of the real-time visual and auditory feedback provided by different devices and the easy monitoring of subjects’ perform- ance, it can increase the adherence to the physical therapy intervention (Hammami et al, 2012).
Previously, maximal isokinetic strength training in OKC position of the knee musculature has been found to significantly improve gait velocity without increas- ing muscle tone in patients with stroke (Engardt et al, 1995; Sharp and Brouwer, 1997). These authors concluded that the use of isokinetic exercises in hem- iparetic patients was beneficial not only for muscle strengthening, but also for functional ability improvement. However, Kim et al (2001) pointed out the lack of a control group in previous studies that reported on improvement of functional ability through isokinetic exercise. Rather, previous research on iso- kinetic strength exercise in OKC position performed during 6 weeks in hemiplegic patients showed that
although the muscle strength improved, no significant effect on gait function was detected (Kim et al, 2001).
It was suggested that isokinetic strength training may need to be performed in conjunction with prac- tical tasks to be of functional benefit.
Many previous studies have compared the effec- tiveness of the OKC and CKC exercise, and the ef- fects of muscle strengthening exercise using the iso- kinetic equipment in stroke patient was also con- firmed (Irish et al, 2010; Sharp and Brouwer, 1997;
Stensdotter et al, 2003). However, although there are two types (OKC and CKC) of isokinetic equipment, most previous studies have used OKC attachment to the isokinetic equipment for isokinetic strengthening exercises in patients with stroke, while CKC attach- ment was rarely used (Killington et al, 2010; Kim et al, 2001). When isokinetic strength training is per- formed in the CKC position to improve function after stroke, we expect it will be more effective in im- proving function not only by providing muscle strengthening, but also by allowing muscular control and sensory stimulation of the lower extremity. It is necessary to study the effects of CKC exercise using the isokinetic equipment. Therefore, the purpose of this study was to compare the effects of OKC ver- sus CKC exercise of the knee joint using the iso- kinetic equipment on the lower extremity sensor- imotor function and gait ability in patients with chronic stroke.
Methods
Study design
This study was carried out prospectively and the convenient sampling method was used to select the samples. Community dwelling stroke survivors were recruited on a volunteer basis through the re- habilitation center of a university hospital. All sub- jects were randomly divided equally into 2 groups:
The CKC isokinetic exercise group and OKC iso- kinetic exercise group. A conventional rehabilitation
Characteristics CKCa group (n1=15) OKCb group (n2=15) F/χ2
Age (years) 54.2±12.4c 53.0±8.7 .761
Gender (Male/Female) 8/7 9/6 1.000
Hemiplegic side (Right/Left) 8/7 7/8 .676
Type of stroke (infarct/hemorrhage) 7/8 6/9 .754
Disease duration (months) 59.8±36.6 57.0±37.9 .838
Height (㎝) 167.2±8.2 169.0±5.7 .492
Body weight (㎏) 64.5±8.0 64.7±4.3 .933
K-MBId 83.5±4.5 81.1±5.5 .824
aclosed kinetic chain, bopen kinetic chain, cmean±standard deviation, dKorea-modified Barthel index.
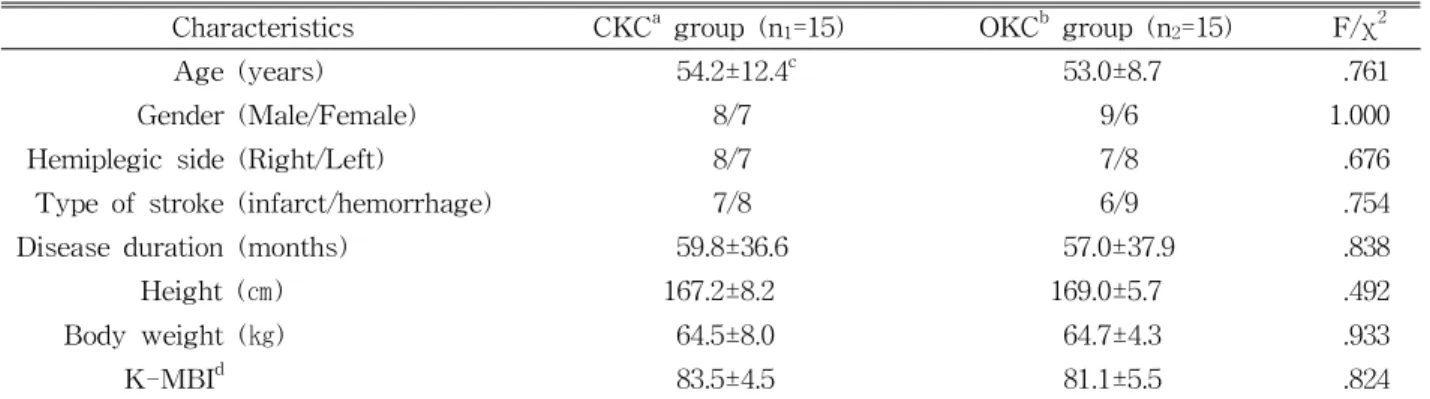
Table 1. Demographics and clinical characteristics of the participants (N=30)
program was applied to all subjects and maximal concentric isokinetic exercise was additionally applied to the hemiparetic knee in CKC or OKC position.
Subjects
Thirty community-dwelling individuals who had experienced a stroke and had residual unilateral weakness were included. The inclusion criteria were as follows: (1) a history of a single stroke at least 6 months before participating in the study, (2) ability to walk independently for a minimum of 10 meters without assistive device, (3) an activity tolerance of 45 minutes with resting time, and (4) non- participation in any formal training program or sim- ilar interventions. Participants were excluded if they had (1) visual impairment and comprehensive apha- sia, (2) an unstable medical condition (i.e., uncon- trolled hypertension, arrhythmia, congestive heart failure, or unstable cardiovascular status), (3) a sig- nificant musculoskeletal problem (i.e., fracture, un- stable joint conditions). Each subject received an ex- planation of the study’s purpose and methods prior to participation and provided informed consent according to the ethical principles of the Declaration of Helsinki.
Interventions
Isokinetic exercise of the hemiparetic knee was performed using the Biodex System 3 PRO dyna- mometer (Biodex Medical Systems, Inc., Shirley, NY,
USA). The non-paretic lower limb was not trained.
Verbal encouragement and visual feedback on a monitor were provided during training sessions to motivate maximal effort (McNair et al, 1996). All participants received a total of 45 minutes of CKC or OKC isokinetic exercise per session, 3 times per week for 6 weeks. Each training session included a warm-up of 5 minutes using a stationary bicycle and 10 minutes of passive stretching to cool-down of the knee extensors and flexors after the isokinetic exercise.
The OKC isokinetic exercise was conducted using the OKC knee attachment. Each subject was seated in a comfortable upright position with a 110˚ hip flexion and 90˚ knee flexion. The trunk, pelvis, and thigh were fixed to the dynamometer chair with Velcro straps to minimize body movement and then the knee attachment was fixed 1 ㎝ above the me- dial malleolus. The OKC isokinetic exercise consisted of 15 sets of maximal knee extension and flexion performed at 3 angular velocities, including low speed (at 90˚/sec, 5 repetitions, 5 sets), moderate speed (at 120˚/sec, 8 repetitions, 5 sets), and high speed (at 150˚/sec, 10 repetitions, 5 sets), separated by 10 seconds of rest after every set and 2 minutes of rest before each angular velocity change (Büyükvural et al, 2015) (Figure 1).
The CKC isokinetic exercise was conducted using a “leg press” knee attachment. Participants were positioned in the seat of the isokinetic dynamometer
A B
Figure 1. Isokinetic exercise (A: open kinetic chain, B: closed kinetic chain).
with 90˚ hip flexion and 45˚ knee flexion. Similar to the OKC position, the participant’s trunk, pelvis, and thigh were fixed to the dynamometer chair with Velcro straps to minimize body movement. Then, to stabilize the subject’s foot and footplate, a padded Velcro brand hook and loop fastener foot strap was threaded through the middle strap guides and secured over the forefoot. The heel strap was then threaded through the appropriate heel strap slots and secured tightly against the patient’s heel. The footplate could be used in a fixed position of 5-10˚ plantarflexion.
The CKC isokinetic exercise consisted of 15 sets of maximal knee extension and flexion performed at 3 angular velocities, including low speed (at 90˚/sec, 5 repetitions, 5 sets), moderate speed (at 120˚/sec, 8 repetitions, 5 sets), and high speed (at 150˚/sec, 10 repetitions, 5 sets) separated by 10 seconds of rest after every set and 2 minutes of rest before each an- gular velocity change (Figure 1).
Outcome measures
Measurements of the knee and ankle isokinetic strength, knee joint position sense, and gait perform- ance were assessed 2 to 3 days before and 2 to 3 days after the intervention.
Isokinetic muscle strength test
Maximal concentric contraction of the knee and
ankle muscles was measured by the Biodex System 3 PRO. This equipment has shown good-to-excellent test-retest reliability of the muscle strength meas- urements (Flansbjer et al, 2005). Prior to the test, all participants performed a 5-minute warm-up using a stationary cycle and test procedures using sub-max- imal practice trials to familiarize with the equipment.
After a 10-minute rest time, to measure the knee isokinetic muscle strength, the subject was seated with the lateral femoral epicondyle of the knee joint axis aligned with the mechanical axis of the dynamometer. Then, the knee attachment was fixed 1 ㎝ above the medial malleolus. Each participant was required to fold the arms across the chest, and their trunk, pelvis, and thigh were fixed to the dy- namometer chair with a Velcro strap in order to prevent compensation by the upper limbs, minimize body movement, and ensure optimal movement of the knee joint of the paretic limb during the test (Pincivero et al, 2003). Further, to promote maximal concentric contraction, visual feedback from a com- puter monitor and verbal instruction of push and pull as hard as possible were provided (McNair et al.
1996). Five maximum concentric contractions were performed at 60˚/sec, and the peak torque generated over 5 repetitions was recorded and normalized to the body weight (MacIntyre et al, 2010).
Then, maximal concentric contraction was meas- ured for the dorsiflexors and plantarflexors.
Participants were seated with the ankle joint axis aligned with the mechanical axis of the dynamometer. After performing a practice trial, par- ticipants were instructed to push and pull the at- tachment as hard and as fast as possible. Five max- imum concentric contractions were performed at 30˚
/sec, and the peak torque generated over 5 repeti- tions was recorded and normalized to the body weight (MacIntyre et al, 2010).
In addition, the hamstring/quadriceps (H/Q) ratio was calculated to determine the movement quality of the knee joint, as this index may be used as a po- tential biomarker to probe the therapeutic effective-
ness of muscle strengthening. The formula for calcu- lating H/Q ratio was as follows (Hong et al, 2012):
H/Q ratio (%) = (isokinetic peak torque of ham- string ÷ isokinetic peak torque of quadriceps) × 100
Knee position sense test
Biodex System 3 PRO was used to assess the position sense of the knee joint. Before the test, one practice trail was performed with eyes open to fa- miliarize the tester with the explanation and equipment. After 10 minutes of rest, the participants wore an eye patch and earplugs to prevent the input of visual and auditory information (Peixoto et al, 2011). To measure the position sense of the knee joint, the participant was placed on the equipment and the starting angle of the test was set at 90˚
knee flexion. The target joint angles were 30˚ and 60˚ knee flexion; participants were instructed in ad- vance to hold for 10 seconds and perceive the target joint angle position. During passive extension of the knee joint at an angular velocity of 2˚/sec, each participant was instructed to press a stop button when he or she recognized the target angle (Rombaut et al, 2010). The knee joint reposition er- ror was defined as the absolute difference between the reproduction angle and target angle. A total of 3 repetitions were performed and 10 seconds of rest were provided for each measurement. The mean value of the error angles was used for the analysis and was measured before the strength test to mini- mize the effect of muscle fatigue (Hiemstra et al, 2001). Sekir et al (2008) showed that the position sense measurement using isokinetic device has high intra-tester reliability (intraclass correlation co- efficient=.90-.94).
Gait performance test
Spatiotemporal gait parameters were measured us- ing the GAITRite mat (CIR Systems Inc., Clifton, NJ, USA). The GAITRite mat contains 6 sensor pads with 13,824 sensors encapsulated in a roll-up carpet with an active area of 3.66 m length and .61
m width. Data were sampled at 30 ㎐. Participants performed 3 trials of walking at a self-selected speed across a level 10 m walkway with a pressure sensi- tive mat in the middle (Patterson et al, 2010). Prior to data collection, participants performed one practice trial to familiarize themselves with the procedure.
Three trials were recorded for each participant and the average values were used for subsequent analysis. The following variables were obtained: gait velocity, step length, and swing time. Spatial (step length) and temporal (swing time) gait symmetry in- dices were calculated as shown below (Hendrickson et al, 2014):
Symmetry index = non-paretic limb value ÷ (paretic limb value + non-paretic limb value)
The gait symmetry index (SI) ranges from 0 to 1.
A gait SI of .5 indicates equal values of the paretic and non-paretic limbs (i.e., perfect symmetry). A SI
<.5 indicates that the paretic limb has a greater val- ue than the non-paretic limb, while SI >.5 indicates that the non-paretic limb has a greater value than the paretic limb for a particular variable (Hendrickson et al, 2014).
Statistical analysis
Data were statistically analyzed using PASW Statistics for Windows, ver. 18 (SPSS Inc., Chicago, IL, USA). Continuous variables, such as age, disease duration, height, body weight, Korean version of the Modified Barthel Index, isokinetic PT/BW, H/Q ratio, reposition error, and gait spatiotemporal parameters were presented as mean±standard deviation.
Demographic and clinical characteristics of subjects were compared between two groups by the in- dependent t-test (for continuous variables). The χ2 test was used to compare the categorical variables, such as gender, hemiplegic side, and type of stroke, between two groups. A paired t-test was used to analyze the training effects within group differences (pre and post intervention), and the independent t-test for differences between the groups. Statistical significance for α was set at .05.
Parameters CKCa group (n1=15) OKCb group (n2=15)
Pre Post Changes Pre Post Changes
Knee PTc/BWd
(Nm/㎏)
Extensor 78.74±46.57e105.30±50.92** 26.29±10.67 71.54±35.80 103.86±46.23** 32.32±13.85 Flexor 22.13±13.85 34.14±18.11** 12.01±9.67 21.87±19.97 38.83±26.94** 16.96±10.84 Ankle
PT/BW (Nm/㎏)
Dorsiflexor 14.85±8.09 19.42±11.42 4.57±5.41 15.28±11.67 17.33±11.94 2.05±5.29 Plantarflexor 25.14±15.60 35.12±17.70** 9.98±5.63‡ 24.78±22.33 25.68±22.97 .90±4.91 H/Qf ratio (%) 28.47±14.45 37.65±10.97** 9.16±10.71 25.66±21.16 42.20±26.37** 16.55±22.30 Knee Position error (˚) 10.28±6.27 7.46±4.60** -2.82±2.57† 13.54±9.48 12.91±8.64 -.63±2.38
aclosed kinetic chain,bopen kinetic chain, cpeak torque, dbody weight, emean±standard deviation, fhamstring/quadriceps,
*p<.05 and **p<.01 indicate a significant difference between pre and post intervention within the group, †p<.05 and
‡p<.01 indicate a significant difference between the change values two groups.
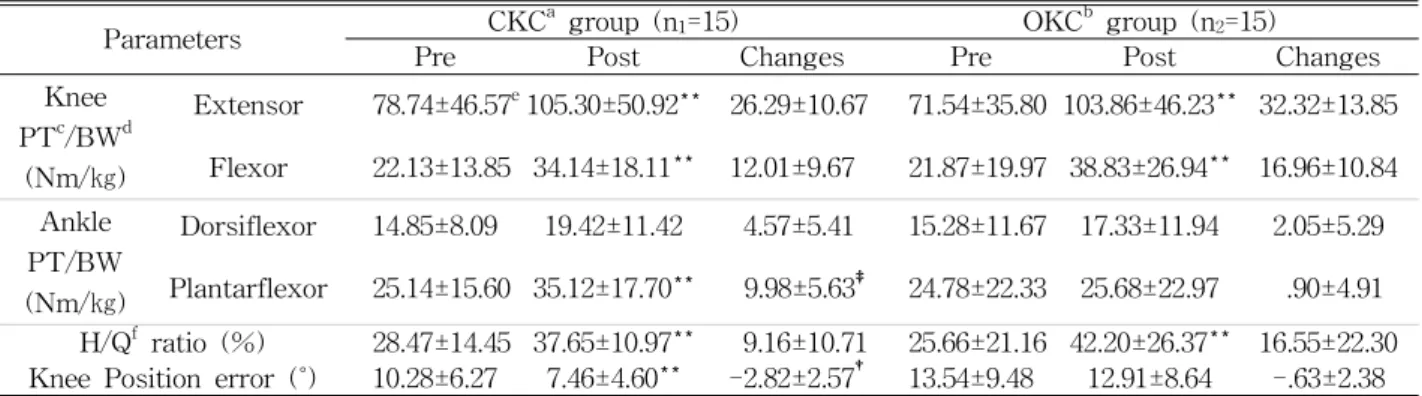
Table 2. Comparison of the isokinetic strength and position sense of the paretic lower extremity pre and post
intervention (N=30)
Results
There were 15 patients (8 males, 7 females) with a mean age of 54.2±12.4 years in the CKC group and 15 patients (9 males, 6 females) with the mean age of 53.0±8.7 years in the OKC group.
Demographic and clinical features of the participants are listed in Table 1. No significant difference in baseline characteristics and physical parameters were found between the groups (p>.05).
After 6 weeks of isokinetic exercise, the PT/BW of the knee muscles significantly increased in both groups compared to pre-intervention PT/BW (p<.01).
However, no statistically significant difference was found between the 2 groups in training effects (p>.05). The mean change in the knee extensor PT/BW were 26.29 Nm/㎏ in the CKC group and 32.32 Nm/kg in the OKC group, while those for the knee flexor PT/BW were 12.01 Nm/㎏ in the CKC group and 16.96 Nm/㎏ in the OKC group. The PT/BW of the ankle plantarflexor PT/BW sig- nificantly increased in the CKC group compared to that in the OKC group (p<.01). The mean change values in the ankle plantarflexor PT/BW were 9.98 Nm/㎏ in the CKC group and .90 Nm/㎏ in the OKC group. However, the PT/BW of the ankle dorsiflexor was not significantly different between two groups (p>.05) (Table 2).
The H/Q ratio was not significantly different be- tween the groups (p>.05). However, it significantly increased in both groups compared to pre-inter- vention H/Qratio (p<.01). The mean change values in the H/Q ratio were 9.16 % in the CKC group and 16.55 % in the OKC group. The reposition error was significantly decreased in the CKC group compared to the OKC group after intervention (p<.05). The mean change values of the knee joint reposition error were -2.82˚ in the CKC group and -.63˚ in the OKC group (Table 2).
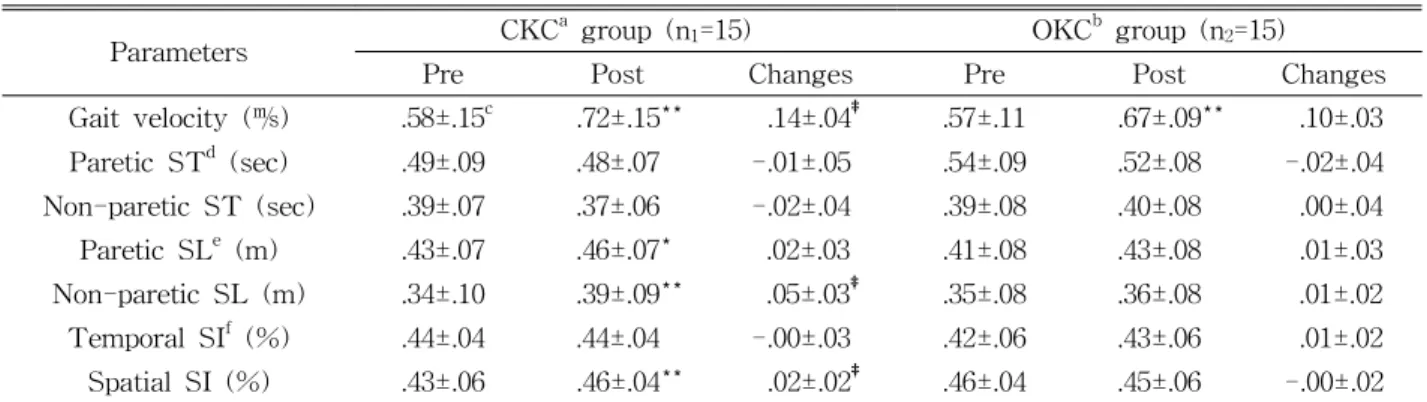
Gait velocity significantly increased in both groups after intervention (p<.01). Inparticular, statistical analysis of the mean changes showed significant im- provements in the CKC group compared to the OKC group (p<.01). The mean change values in the gait velocity were .14 ㎧ in the CKC group and .10 ㎧ in the OKC group. The spatial gait SI was significantly improved in the CKC group compared to the OKC group (p<.01). However, the temporal gait SI was not significantly different between the groups (p<.05) (Table 3)
Discussion
Patients with stroke experience muscle weakness and impaired proprioceptive function in the lower ex-
Parameters CKCa group (n1=15) OKCb group (n2=15)
Pre Post Changes Pre Post Changes
Gait velocity (㎧) .58±.15c .72±.15** .14±.04‡ .57±.11 .67±.09** .10±.03
Paretic STd (sec) .49±.09 .48±.07 -.01±.05 .54±.09 .52±.08 -.02±.04
Non-paretic ST (sec) .39±.07 .37±.06 -.02±.04 .39±.08 .40±.08 .00±.04
Paretic SLe (m) .43±.07 .46±.07* .02±.03 .41±.08 .43±.08 .01±.03
Non-paretic SL (m) .34±.10 .39±.09** .05±.03‡ .35±.08 .36±.08 .01±.02
Temporal SIf (%) .44±.04 .44±.04 -.00±.03 .42±.06 .43±.06 .01±.02
Spatial SI (%) .43±.06 .46±.04** .02±.02‡ .46±.04 .45±.06 -.00±.02
aclosed kinetic chain, bopen kinetic chain, cmean±standard deviation, dstep time, estep length, fsymmetry index.
*p<.05 and **p<.01 indicate a significant difference between pre and post intervention within the group, †p<.05 and
‡p<.01 indicate a significant difference between the change values two groups.
Table 3. Comparison of the spatiotemporal gait parameters pre and post intervention (N=30)
tremity (Cramp et al, 2006; Lin, 2005; Patten et al, 2004). Many researchers have concluded that the knee muscle strength and proprioceptive function are closely related to gait function (Hsu et al, 2003;
Sharp and Brouwer 1997). Therefore, intervention programs emphasizing muscle strengthening and en- hancing proprioceptive function are indicated for hemiplegic stroke patients without injury. In the cur- rent study, we aimed to analyze the effect of iso- kinetic PRT performed in CKC or OKC positions on the lower extremity sensorimotor function and gait performance in patients with chronic stroke. For this purpose, isokinetic equipment was used to perform PRT of the hemiparetic knee joint in CKC or OKC positions for 6 weeks. As a result, the OKC iso- kinetic exercise showed a significant improvement in the gait velocity, as well as in the muscle strength- ening and H/Q ratio of the knee compared with pre-intervention. On the contrary, the CKC isokinetic exercise significantly improved muscle strengthening in the ankle plantarflexor, as well as muscle strength and H/Q ratio of the knee. In addition, it was con- firmed that the reposition error of the knee joint de- creased, while the gait velocity and spatial gait sym- metry improved more significantly in the CKC group.
In general, isokinetic devices are known to be safe for evaluation and strength training without the risk of injury or increased muscle tone in persons with stroke (Engart et al, 1995; Flansbjer et al, 2005; Kim
et al, 2001; Sharp and Brouwer, 1997). They are very effective in inducing maximal concentric con- traction of target muscles; in addition, they produce a faster rate of strength gain and reduce muscle tenderness better than isotonic exercise (Coudeyre et al, 2016; Pontes et al, 2018). In the present study, both methods of isokinetic PRT were found very ef- fective in improving the strength of target muscles.
The OKC isokinetic exercise is very useful to re- peatedly and constantly elicit maximal concentric contractions of the knee extensors and flexors.
However, the effect of OKC isokinetic exercise was restricted to the target muscle, while CKC isokinetic exercise had a positive effect on the improvement of the ankle strength adjacent to the target muscle.
These results may be related to the fact that the CKC isokinetic exercise effectively induces the con- traction of more muscles around the target muscle by multi-joint movements (Augustsson et al, 1998;
Jan et al, 2009; Stendotter et al, 2003). In other words, the CKC isokinetic exercise used the ankle muscles as well as the knee muscles, while the OKC isokinetic exercise mostly used the isolated knee ex- tensor and flexors.
After interventions, with both CKC and OKC group showing improvement in gait velocity com- pared to baseline status. Previous studies similar re- sults reported that isokinetic peak torque of the af- fected knee and ankle muscles predicted the gait ve-
locity in patients with stroke (Flansbjer et al, 2005;
Hsu et al, 2003; Olney et al, 1991). In addition, iso- kinetic strength training program of the hemiparetic knee and ankle muscles resulted in significant im- provement in muscle strength and gait velocity (Büyükvural et al, 2015; Killington et al, 2010;
Patterson et al, 2010). In our study, the increased strength of the knee muscles of the subjects after the intervention had a direct effect on the improvement of the gait velocity (Hyun et al, 2015).
Noteworthy, the comparison between the groups showed that the gait velocity was significantly high- er in the CKC group than in the OKC group. The minimum clinically important difference value for gait velocity was set at .10-.20 ㎧ (Bohannon and Glenney, 2014). In this study, the gait velocity of the OKC group improved by .10 ㎧ and that of the CKC group improved by .14 ㎧. Therefore, the CKC iso- kinetic exercise was more clinically meaningful in improving gait velocity. The reason for this result could be the fact that CKC isokinetic exercise im- proved the strength of the ankle muscles as well as of the knee muscles. The ankle plantarflexor contrib- utes to propelling the body forward by creating strong ground reaction forces in the late stance to early pre-swing phase of the gait cycle with com- fortable speed (Allen et al, 2011; Neptune et al, 2001;
Olney er al, 1991). Perhaps the reason for the sig- nificant improvement of the plantarflexors seems to be the result of a statistically higher gait velocity in the CKC group.
Hemiplegic patients typically had a limitation of weight shifting toward the paretic side due to muscle weakness and impaired proprioception of the lower limb, resulting in an asymmetric gait pattern (Hsu et al, 2003; Lin, 2005; Patterson, 2010). The subjects who participated in this study had a temporal SI of .43 and a spatial SI of .45. This means that the step time and step length of the non-paretic lower limb were shortened during gait. Perhaps the instability of the paretic lower limb was the main reason during the stance phase (Hendrickson et al, 2014). In this
study, an improvement of spatial gait symmetry was noted in the CKC group compared to the OKC group. Although the CKC isokinetic exercise has not progressed at the weight bearing position, the knee extension and flexion with the distal extremity firmly fixed was similar to the actual gait pattern. Lee et al (2013) reported that the CKC exercise showed sig- nificant changes in contact area and peak contact pressure of the hind foot compared to the OKC exercise. These results would imply that CKC ex- ercise is beneficial for weight bearing ability of the affected leg. The pushing of the CKC isokinetic ex- ercise was accompanied by the hip extension, knee extension, and ankle plantarflexion, and pulling was accompanied by the hip flexion, knee flexion, and ankle dorsiflexion (Stensdotter et al, 2003). This re- petitive motion of the lower extremity was similar to the actual gait pattern and daily routines compared with OKC exercise. As the CKC approach is based on the functional movement such as normal gait pattern performed during the exercise, this might be more easily accepted by patients during exercise (Krawczyk et al, 2014).
Moreover, a greater improvement in reposition sense of the knee joint was found in the CKC ex- ercise group. Previous study has reported similar findings, an 8 week leg press exercise (i.e., CKC) improved reposition sense by 2.8°, however, leg curl exercise (i.e., OKC) improved reposition sense by .6˚
in patients with knee osteoarthritis (Jan et al, 2009).
The CKC exercise has been shown to enhance pro- prioceptive performance by stimulation of mechanor- eceptors in the intra-articular and firing muscle spindles in patients with the knee disorders (Hurd et al, 2006; Jan et al, 2009; Shields et al, 2005). As a result, the functional movement of the CKC exercise and the improvement of the knee joint position sense contributed to the stability of the stance phase of the affected leg. Maybe this point was the reason for the longer step length of the unaffected lower limb and improved spatial gait symmetry (An and Jo, 2017).
Finally, both OKC and CKC isokinetic exercises
were effective in improving the H/Q ratio. The H/Q ratio is a parameter used to describe the muscular control of the knee joint (Aagaard et al, 1998).
Decreased H/Q ratio has been suggested to be asso- ciated with increased risk of the knee joint pain and ligament injury (Aagaard et al, 1998; Hewett et al, 2008). Our result showed that the H/Q ratio was significantly increased in both groups compared to baseline measurement values. Basically, it seems that both interventions were able to improve the balance of muscular strength between the agonist and antag- onist muscles of the knee. Further, this result sug- gested that both interventions can be used to prevent the knee from secondary damages due to improved muscular control of the knee joint.
The present study has some limitations that re- quire consideration when interpreting the results.
First, the follow-up measurements were not per- formed; accordingly, the carryover effect of the 2 types of isokinetic exercise could not be determined.
Second, the intervention applied in this study was expected to have a sufficient influence on the hip muscles. Nonetheless, the lack of measuring the iso- kinetic strength of the hip muscles also limits the interpretation of the results. Finally, this study in- cluded a small sample, and therefore its statistical results are difficult to generalize. Therefore, future studies should prove the long-term effects of the 2 types isokinetic exercises on the lower extremities sensorimotor function, including on the hip joint and on functional ability.
Conclusion
This study was conducted to determine the effect of isokinetic exercise on the hemiparetic knee at the CKC and OKC position in patients with chronic stroke. As a result, both interventions were effective in improving the strength of the knee muscles. In addition, the CKC isokinetic exercise improved strength of the ankle plantarflexors and knee joint
position sense and positive effected gait velocity and spatial gait symmetry. Therefore, in order to improve the functional ability though isokinetic exercise in patients with stroke, functional and task-oriented muscle strengthening (i.e., CKC position) may be more effective than simple muscle strengthening task (i.e., OKC position). In addition, it may be necessary to develop various interventions that can be per- formed in CKC position.
References
Aagaard P, Simonsen EB, Magnusson SP, et al. A new concept for isokinetic hamstring: Quadriceps muscle strength ratio. Am J Sports Med. 1998;
26(2):231-237. https://doi.org/10.1177/03635465980 260021201
Allen JL, Kautz SA, Neptune RR. Step length asym- metry is representative of compensatory mecha- nisms used in post-stroke hemiparetic walking.
Gait Posture. 2011;33(4):538-543. https://doi.org/
10.1016/j.gaitpost.2011.01.004
An CM, Jo SO. Effects of Talocrural Mobilization with Movement on Ankle Strength, Mobility, and Weight-Bearing Ability in Hemiplegic Patients with Chronic Stroke: A Randomized Controlled Trial. J Stroke Cerebrovasc Dis. 2017;26(1):169- 176. https://doi.org/10.1016/j.jstrokecerebrovasdis.
2016.09.005
Augustsson J, Esko A, Thomeé R, et al. Weight train- ing of the thigh muscles using closed vs. open kinetic chain exercises: A comparison of perform- ance enhancement. J Orthop Sports Phys Ther.
1998;27(1):3-8. https://doi.org/10.2519/jospt.1998.27.1.3 Bloem BR, Allum JH, Carpenter MG, et al. Is lower leg proprioception essential for triggering human automatic postural responses? Exp Brain Res.
2000;130(3):375-391. https://doi.org/10.1007/s00221 9900259
Bohannon RW, Glenney SS. Minimal clinically im- portant difference for change in comfortable gait
speed of adults with pathology: A systematic review. J Eval Clin Pract. 2014;20(4):295-300.
https://doi.org/10.1111/jep.12158
Büyükvural Şen S, Özbudak Demir S, Ekiz T, et al.
Effects of the bilateral isokinetic strengthening training on functional parameters, gait, and the quality of life in patients with stroke. Int J Clin Exp Med. 2015;8(9):16871-16879.
Coudeyre E, Jegu AG, Giustanini M, et al. Isokinetic muscle strengthening for knee osteoarthritis: A systematic review of randomized controlled trials with meta-analysis. Ann Phys Rehabil Med.
2016;59(3):207-215. https://doi.org/10.1016/j.rehab.
2016.01.013
Cramp MC, Greenwood RJ, Gill M, et al. Low in- tensity strength training for ambulatory stroke patients. Disabil Rehabil. 2006;28(13-14):883-889.
https://doi.org/10.1080/09638280500535157
Engardt M, Knutsson E, Jonsson M, et al. Dynamic muscle strength training in stroke patients:
Effects on knee extension torque, electromyo- graphic activity, and motor function. Arch Phys Med Rehabil. 1995;76(5):419-425.
Flansbjer UB, Holmbäck AM, Downham D, et al.
What change in isokinetic knee muscle strength can be detected in men and women with hemi- paresis after stroke? Clin Rehabil. 2005;19(5):
514-522. https://doi.org/10.1191/0269215505cr854oa Hammami N, Coroian FO, Julia M, et al. Isokinetic
muscle strengthening after acquired cerebral damage: A literature review. Ann Phys Rehabil Med. 2012;55(4):279-291. https://doi.org/10.1016/
j.rehab.2012.03.003
Hendrickson J, Patterson KK, Inness EL, et al.
Relationship between asymmetry of quiet stand- ing balance control and walking post-stroke.
Gait Posture. 2014;39(1):177-181. https://doi.org/
10.1016/j.gaitpost.2013.06.022
Hewett TE, Myer GD, Zazulak BT. Hamstrings to quadriceps peak torque ratios diverge between sexes with increasing isokinetic angular velocity.
J Sci Med Sport. 2008;11(5):452-459. https://do-
i.org/10.1016/j.jsams.2007.04.009
Hiemstra LA, Lo IK, Fowler PJ. Effect of fatigue on knee proprioception: Implications for dynamic stabilization. J Orthop Sports Phys Ther. 2001;
31(10):598-605. https://doi.org/10.2519/jospt.2001.
31.10.598
Hong WH, Chen HC, Shen IH, et al. Knee muscle strength at varying angular velocities and asso- ciations with gross motor function in ambulatory children with cerebral palsy. Res Dev Disabil.
2012;33(6):2308-2316. https://doi.org/10.1016/j.ridd.
2012.07.010
Hsu AL, Tang PF, Jan MH. Analysis of impairments influencing gait velocity and asymmetry of hem- iplegic patients after mild to moderate stroke.
Arch Phys Med Rehabil. 2003;84(8):1185-1193.
https://doi.org/10.1016/S0003-9993(03)00030-3 Hurd WJ, Chmielewski TL, Snyder-Mackler L.
Perturbation-enhanced neuromuscular training alters muscle activity in female athletes. Knee Surg Sports Traumatol Arthrosc. 2006;14(1):
60-69. https://doi.org/10.1007/s00167-005-0624-y Hyun CW, Han EY, Im SH et al. Hemiparetic knee
extensor strength and balance function are pre- dictors of ambulatory function in subacute stroke patients. Ann Rehabil Med. 2015;39(4):
577-585. https://doi.org/10.5535/arm.2015.39.4.577 Irish SE, Millward AJ, Wride J, et al. The effect of
closed-kinetic chain exercises and open-kinetic chain exercise on the muscle activity of vastus medialis oblique and vastus lateralis. J Strength Cond Res. 2010;24(5):1256-1262. https://do- i.org/10.1519/JSC.0b013e3181cf749f
Jan MH, Lin CH, Lin YF, et al. Effects of weight-bearing versus nonweight-bearing ex- ercise on function, walking speed, and position sense in participants with knee osteoarthritis: A randomized controlled trial. Arch Phys Med Rehabil. 2009;90(6):897-904. https://doi.org/10.1016/
j.apmr.2008.11.018
Krawczyk M, Szczerbik E, Syczewska M. The com- parison of two physiotherapeutic approaches for
gait improvement in sub-acute stroke patients.
Acta Bioeng Biomech. 2014;16(1):11-18. https://
doi.org/10.5277/abb140102
Killington MJ, Mackintosh SF, Ayres MB. Isokinetic strength training of lower limb muscles follow- ing acquired brain injury. Brain Inj. 2010;
24(12):1399-1407. https://doi.org/10.3109/02699052.
2010.511589
Kim CM, Eng JJ, MacIntyre DL, Dawson AS.
Effects of isokinetic strength training on walk- ing in persons with stroke: a double-blind con- trolled pilot study. J Stroke Cerebrovasc Dis.
2001;10(6):265-273. https://doi.org/10.1053/jscd.2001.
123775
Lee NK, Kwon JW, Son SM, et al. Changes of plan- tar pressure distributions following open and closed kinetic chain exercise in patients with stroke. NeuroRehabilitation. 2013;32(2):385-390.
https://doi.org/10.3233/NRE-130859
Lin SI. Motor function and joint position sense in relation to gait performance in chronic stroke patients. Arch Phys Med Rehabil. 2005;86(2):
197-203. https://doi.org/10.1016/j.apmr.2004.05.009 Mansfield A, Peters AL, Liu BA, et al. Effect of a
perturbation-based balance training program on compensatory stepping and grasping reactions in older adults: A randomized controlled trial. Phys Ther. 2010;90(4):476-491. https://doi.org/10.2522/
ptj.20090070
McNair PJ, Depledge J, Brettkelly M, et al. Verbal encouragement: Effects on maximum effort vol- untary muscle action. Br J Sports Med. 1996;
30(3):243-245. https://doi.org/10.1136/bjsm.30.3.245 Neptune RR, Kautz SA, Zajac FE. Contributions of the individual ankle plantar flexors to support, for- ward progression and swing initiation during walking. J Biomech. 2001;34(11):1387-1398. https://
doi.org/10.1016/S0021-9290(01)00105-1
Olney SJ, Griffin MP, Monga TN, et al. Work and power in gait of stroke patients. Arch Phys Med Rehabil. 1991;72(5):309-314.
Patten C, Lexell J, Brown HE. Weakness and
strength training in persons with poststroke hemiplegia: Rationale, method, and efficacy. J Rehabil Res Dev. 2004;41(3A):293-312.
Patterson KK, Gage WH, Brooks D, et al. Evaluation of gait symmetry after stroke: A comparison of current methods and recommendations for standardization. Gait Posture. 2010;31(2):241-246.
https://doi.org/10.1016/j.gaitpost.2009.10.014 Peixoto JG, Dias JM, Dias RC, et al. Relationships
between measures of muscular performance, pro- prioceptive acuity, and aging in elderly women with knee osteoarthritis. Arch Gerontol Geriatr.
2011;53(2):253-257. https://doi.org/10.1016/j.archger.
2011.05.008
Pincivero DM, Coelho AJ, Campy RM, et al. Knee extensor torque and quadriceps femoris EMG during perceptually-guided isometric contractions.
J Electromyogr Kinesiol. 2003;13(2):159-167.
https://doi.org/10.1016/S1050-6411(02)00096-2 Pontes SS, de Carvalho ALR, Almeida KO, et al.
Effects of isokinetic muscle strengthening on muscle strength, mobility, and gait in post-stroke patients: A systematic review and meta-analysis.
Clin Rehabil. 2018;28:269215518815220. https://do- i.org/10.1177/0269215518815220
Protas EJ, Mitchell K, Williams A, et al. Gait and step training to reduce falls in Parkinson's disease. NeuroRehabilitation. 2005;20(3):183-190.
Rombaut L, De Paepe A, Malfait F, et al. Joint posi- tion sense and vibratory perception sense in pa- tients with Ehlers-Danlos syndrome type III (hypermobility type). Clin Rheumatol. 2010;29(3):
289-295. https://doi.org/10.1007/s10067-009-1320-y Sekir U, Yildiz Y, Hazneci B, et al. Reliability of a functional test battery evaluating functionality, proprioception, and strength in recreational ath- letes with functional ankle instability. Eur J Phys Rehabil Med. 2008;44(4):407-415.
Sharp SA, Brouwer BJ. Isokinetic strength training of the hemiparetic knee: Effects on function and spasticity. Arch Phys Med Rehabil. 1997;78(11):
1231-1236.
This article was received January 9, 2019, was re- viewed January 9, 2019, and was accepted March 25, 2019.
Shields RK, Madhavan S, Gregg E, et al.
Neuromuscular control of the knee during a re- sisted single-limb squat exercise. Am J Sports Med. 2005;33(10):1520-1526. https://doi.org/10.1177/
0363546504274150
Stensdotter AK, Hodges PW, Mellor R, et al.
Quadriceps activation in closed and in open ki- netic chain exercise. Med Sci Sports Exerc. 2003;
35(12):2043-2047. https://doi.org/10.1249/01.MSS.
0000099107.03704.AE
Wist S, Clivaz J, Sattelmayer M. Muscle strengthen- ing for hemiparesis after stroke: A meta-analysis.
Ann Phys Rehabil Med. 2016;59(2):114-124.
https://doi.org/10.1016/j.rehab.2016.02.001