서 론
대장용종은 대장의 내강 쪽으로 점막의 표면에서 돌출된 융기물 을 통틀어 말하는 것으로 대장내시경 검사 건수가 증가하면서 진단 율이 높아지고 이에 대한 관심도 증가하고 있다. 대장용종은 대장암 으로 발달할 수 있기 때문에1) 발견 시 제거하는 것이 중요하다. 대장 암은 식단이 서구화되고 신체활동이 저하되면서 오는 비만도 증가 에 따라 발생률이 증가하고 있다.2) 대장암은 서구에서 발생률이 가
장 높지만 중진국 및 개발도상국에서도 발생률이 증가하는 추세이 다.3) 국내에서도 발생률과 사망률이 함께 증가하는 질환으로 연령에 비례하여 발생률이 증가하고 있다.4)
대장암의 위험요인으로 복부비만, 대장암 가족력, 염증성 장질환, 신체활동부족, 흡연, 음주 등이 있으며 2007년 World Cancer Re- search Fund (WCRF)와 American Institute for Cancer Research는 복부 비만을 신뢰할 근거가 있는(confident evidence) 대장암의 위험인자로 평가하였다.5) 복부비만은 대사증후군의 주된 위험인자로 유전–환 Received March 6, 2017 Revised June 4, 2017 Accepted June 23, 2017
Corresponding author Ah-ra Koh Tel: +82-31-210-0114, Fax: +82-31-210-0140 E-mail: [email protected]
ORCID: http://orcid.org/0000-0001-8146-8286
Copyright © 2018 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Original Article
https://doi.org/10.21215/kjfp.2018.8.1.15 eISSN 2233-9116
Korean J Fam Pract. 2018;8(1):15-20
Korean Journal of Family Practice
KJFP
건강검진 수진자에서 대장용종과 대사증후군 지표, 혈중요산농도와의 상관관계
고아라*, 김춘환, 방준호, 정광욱, 유희권
동수원병원 가정의학과
The Correlation between Colon Polyps and Metabolic Syndrome Parameters, Serum Uric Acid Level in Health Screen Examinees
Ah-ra Koh*, Chun-hwan Kim, Jun-ho Bang, Kwang-wook Jung, Hee-kwon Yu Department of Family Medicine, Dongsuwon General Hospital, Suwon, Korea
Background: Adenomatous polyps of the colon are precancerous lesions. Whether hyperuricemia represents an independent risk factor for colon cancer is controversial. Studies have indicated a relationship between colon cancer and metabolic syndrome. The aim of this study was to determine whether metabolic syndrome parameters and hyperuricemia are risk factors for colon polyps and whether uric acid level is a predictive factor.
Methods: We retrospectively reviewed the medical records of patients with colon polyps who visited the General Hospital Health Promotion Center in Suwon and underwent colonoscopic examination between January 2011 and December 2014. A total of 1,435 asymptomatic adults were included.
We analyzed the odds ratios and 95% confidence intervals for colon polyps by using a multivariable logistic regression analysis. All the analyses were conducted using IMB SPSS 22.0.
Results: In the 1,435 patients, the prevalence of colon polyps was 21.3% (n=305). t-test revealed that the prevalence of colon polyps was higher in the patients with high triglyceride level, body mass index, and abdominal circumference. However, in the multiple regression analysis, the risk of colon polyps was not significantly associated with metabolic syndrome parameters and serum uric acid level.
Conclusion: The occurrence of colon polyps was not associated with metabolic syndrome parameters and serum uric acid level in the health screening examinees in this study.
Keywords: Colonic Polyps; Metabolic Syndrome; Uric Acid
Ah-ra Koh, et al. Correlation between Colon Polyps, Metabolic Syndrome Parameters, Serum Uric Acid
Korean Journal of Family Practice
KJFP
경 상호작용이 대사증후군과 대장암의 공통된 질병 발생기전으로 제시되고 있다.6,7) 대사증후군은 복부비만, 고중성지방혈증, 저밀도 지질단백콜레스테롤혈증, 고혈압, 고혈당의 5가지 구성요소 중 3가 지 이상을 가지는 경우로 정의된다.8)
요산은 퓨린(purine)대사의 최종산물로 인체는 요산을 직접 대사 시킬 수 없기 때문에 장 혹은 신장을 통한 배설이 필요하다. 일반적 으로 혈중요산농도는 연령, 혈압, 체질량지수(body mass index, BMI), 체내용적변화 및 음주 등 다양한 인자들에 이해 영향을 받는다.9) 많 은 연구에서 대사증후군과 심혈관질환의 위험인자들이 혈청요산 농도와 밀접한 관련성을 갖는다고 밝혀졌다.10) 이에 더해 혈청요산 농도가 높을 때 대장암을 비롯한 종양성 질환을 악화시킬 수 있는 가능성도 제시되고 있다.11)
대장용종의 위험인자로 흡연, 음주, 비만, 신체활동저하, 고지방 식, 대사증후군 등이 제시되고 있지만 우리나라에서 이 위험요소들 이 대장용종 발생의 위험요인이라는 근거를 뒷받침할 만한 연구 실 적이 적고 결과들이 일치하지 않는다.12-14) 대사증후군과 혈중요산농 도를 상승시키는 위험인자가 비슷하며 일부 연구에서 연관성이 있 다고 보고되기도 하나 아직 연구결과가 부족한 실정으로 대사증후 군 지표와 혈중요산농도와 대장용종 발생률과의 관계를 확인하며 혈중요산농도와 대장용종간의 상관관계에 대해 알아보고자 한다.
방 법
1. 연구 대상
본 연구는 2011년 1월부터 2014년 12월까지 경기도 수원시 소재 종 합병원 건강증진센터에서 대장내시경을 받은 무증상 성인 3,149명 중에서 허리둘레를 포함한 신체계측을 시행하지 않고 전대장을 관 찰하지 못한 수검자 1,710명과 과거 대장암으로 진단받았거나 조직 병리검사상 대장암으로 확진된 4명의 수검자들을 제외한 1,435명을 대상으로 연구하였다. 이 연구는 이미 수집된 자료를 이용한 후향적 연구로 참여자의 승낙과 동의를 받지 않았다.
2. 연구 방법
본 연구는 대상자들의 대장내시경 전처치는 수검자가 검사 전일 저녁부터 세척용액을 마셔서 시행하였다. 대장용종은 long flexible colonofibroscope를 이용하였고 회맹부까지 전대장을 관찰하였으며, 생검을 진행하여 조직병리학적으로 확인하였다. 조직병리검사결과 에서 선종성 용종과 과형성용종을 대장용종군, 정상과 단순 염증 성 용종을 비용종군으로 분류하였다.
수검자들의 신체계측 중 키, 몸무게는 자동신체계측기를 이용하
여 측정하였다. BMI는 체중을 신장의 제곱으로 나누어 구하고 허리 둘레는 직립자세에서 최하위 늑골하부와 골반 장골능사이의 가장 가는 부위를 cm단위로 측정하였다. 혈압 측정은 내원 후 10분 이상 의 휴식시간 이후에 측정하였으며 혈액검사는 12시간 이상의 금식 후에 채취한 정맥혈을 이용하였으며 생화학검사들의 정상치는 본 원 검사실의 참고치를 기준으로 판단하였다.
참고치는 총콜레스테롤(0–220 mg/dL), 고밀도지단백콜레스테롤 (30–80 mg/dL), 저밀도지단백콜레스테롤(60–150 mg/dL), 중성지방 (30–200 mg/dL), 공복혈당(74–110 mg/dL), 혈중요산농도(2.5–7 mg/dL) 였다.
3. 통계 분석
수집된 자료들의 통계분석은 IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA)을 이용하여 일반적인 특성 및 총콜레스테롤, 고 밀도지단백콜레스테롤, 저밀도지단백콜레스테롤, 중성지방, 수축기 혈압, 이완기혈압, 공복혈당, BMI, 허리둘레, 혈중요산농도에 따른 대 장용종의 유병률 차이는 pearson chi-suqare test, independent t-test로 검정하였다. 한편 관련 변수들의 대장용종에 대한 위험비를 산출하 기 위해 혼란변수인 성별, 연령을 보정한 상태에서 다중로지스틱회
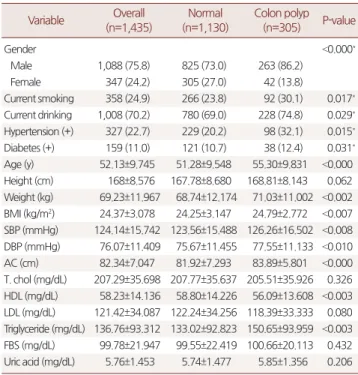
Table 1. Baseline characteristics of the study subjects Variable Overall
(n=1,435)
Normal (n=1,130)
Colon polyp (n=305) P-value
Gender <0.000*
Male 1,088 (75.8) 825 (73.0) 263 (86.2)
Female 347 (24.2) 305 (27.0) 42 (13.8)
Current smoking 358 (24.9) 266 (23.8) 92 (30.1) 0.017* Current drinking 1,008 (70.2) 780 (69.0) 228 (74.8) 0.029* Hypertension (+) 327 (22.7) 229 (20.2) 98 (32.1) 0.015* Diabetes (+) 159 (11.0) 121 (10.7) 38 (12.4) 0.031* Age (y) 52.13±9.745 51.28±9.548 55.30±9.831 <0.000 Height (cm) 168±8.576 167.78±8.680 168.81±8.143 0.062 Weight (kg) 69.23±11.967 68.74±12.174 71.03±11.002 <0.002 BMI (kg/m2) 24.37±3.078 24.25±3.147 24.79±2.772 <0.007 SBP (mmHg) 124.14±15.742 123.56±15.488 126.26±16.502 <0.008 DBP (mmHg) 76.07±11.409 75.67±11.455 77.55±11.133 <0.010 AC (cm) 82.34±7.047 81.92±7.293 83.89±5.801 <0.000 T. chol (mg/dL) 207.29±35.698 207.77±35.637 205.51±35.926 0.326 HDL (mg/dL) 58.23±14.136 58.80±14.226 56.09±13.608 <0.003 LDL (mg/dL) 121.42±34.087 122.24±34.256 118.39±33.333 0.080 Triglyceride (mg/dL) 136.76±93.312 133.02±92.823 150.65±93.959 <0.003 FBS (mg/dL) 99.78±21.947 99.55±22.419 100.66±20.113 0.432 Uric acid (mg/dL) 5.76±1.453 5.74±1.477 5.85±1.356 0.206 Values are presented as number (%) or mean±standard deviation.
BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pres- sure; T. chol, total cholesterol; HDL, high density lipoprotein cholesterol; LDL, low density lipoprotein cholesterol; FBS, fasting blood sugar.
P-value was calculated by independent t-test.
*P-value was calculated by χ2-test.
고아라 외. 대장용종과 대사증후군 지표, 혈중요산농도와의 상관관계 Korean Journal of Family Practice
KJFP
귀분석(multiple logistic resgression)을 이용하여 교차비(odds ratio)와 95% 신뢰구간을 정량화하여 분석하였다. 모든 통계자료는 P-value가 0.05 미만일 때 통계적으로 유의하다고 정의하였다.
결 과
1. 대상자의 일반적 특성 및 대장용종의 유병률
검진대상자 1,435명 중에서 대장용종군은 305명이었고 비용종군 은 1,130명으로 유병률은 21.3%였다. 검진대상자의 평균 나이는 52.1 세이며 남성이 1,088명으로 75.8%를 차지했다. 평균 혈중요산농도는 5.76 mg/dL였다. 대장용종군과 비용종군은 성별, 평균 연령, 고밀도 지단백콜레스테롤, 중성지방, 몸무게, BMI, 수축기혈압, 이완기혈압, 허리둘레에서 평균값의 유의한 차이를 보이는 것으로 나타났다 (P<0.05) (Table 1).
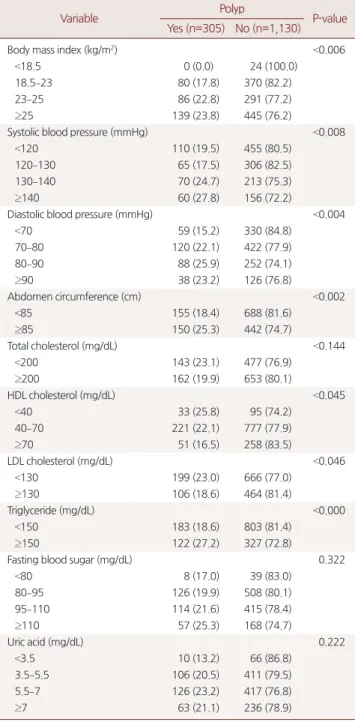
2. 대사증후군관련 지표별, 혈중요산농도에 따른 유병률 검진대상자의 대사증후군 관련 지표별, 혈중요산농도에 따른 유 Table 2. The prevalence rate of colon polyps for variables
Variable Polyp
P-value Yes (n=305) No (n=1,130)
Body mass index (kg/m2) <0.006
<18.5 0 (0.0) 24 (100.0)
18.5–23 80 (17.8) 370 (82.2)
23–25 86 (22.8) 291 (77.2)
≥25 139 (23.8) 445 (76.2)
Systolic blood pressure (mmHg) <0.008
<120 110 (19.5) 455 (80.5)
120–130 65 (17.5) 306 (82.5)
130–140 70 (24.7) 213 (75.3)
≥140 60 (27.8) 156 (72.2)
Diastolic blood pressure (mmHg) <0.004
<70 59 (15.2) 330 (84.8)
70–80 120 (22.1) 422 (77.9)
80–90 88 (25.9) 252 (74.1)
≥90 38 (23.2) 126 (76.8)
Abdomen circumference (cm) <0.002
<85 155 (18.4) 688 (81.6)
≥85 150 (25.3) 442 (74.7)
Total cholesterol (mg/dL) <0.144
<200 143 (23.1) 477 (76.9)
≥200 162 (19.9) 653 (80.1)
HDL cholesterol (mg/dL) <0.045
<40 33 (25.8) 95 (74.2)
40–70 221 (22.1) 777 (77.9)
≥70 51 (16.5) 258 (83.5)
LDL cholesterol (mg/dL) <0.046
<130 199 (23.0) 666 (77.0)
≥130 106 (18.6) 464 (81.4)
Triglyceride (mg/dL) <0.000
<150 183 (18.6) 803 (81.4)
≥150 122 (27.2) 327 (72.8)
Fasting blood sugar (mg/dL) 0.322
<80 8 (17.0) 39 (83.0)
80–95 126 (19.9) 508 (80.1)
95–110 114 (21.6) 415 (78.4)
≥110 57 (25.3) 168 (74.7)
Uric acid (mg/dL) 0.222
<3.5 10 (13.2) 66 (86.8)
3.5–5.5 106 (20.5) 411 (79.5)
5.5–7 126 (23.2) 417 (76.8)
≥7 63 (21.1) 236 (78.9)
Values are presented as number (%).
HDL, high density lipoprotein; LDL, low density lipoprotein.
P-value was calculated by pearson χ2-test for categorical variable.
Table 3. Multiple logistic regression analysis of variables according to the risk of colon polyps
Variable Odds
ratio
95% confidence interval P-value Systolic blood pressure (mmHg)
<120 1 Referent
120–130 0.675 0.464–0.983 <0.040
130–140 0.933 0.606–1.436 0.751
≥140 1.044 0.619–1.761 0.872
Diastolic blood pressure (mmHg)
<70 1 Referent
70–80 1.326 0.910–1.933 0.142
80–90 1.493 0.933–2.392 0.095
≥90 1.120 0.602–2.085 0.720
Abdomen circumference (cm)
<85 1 Referent
≥85 1.173 0.816–1.687 0.389
Total cholesterol (mg/dL)
<200 1 Referent
≥200 0.976 0.686–1.388 0.892
HDL cholesterol (mg/dL)
<40 1 Referent
40–70 0.958 0.614–1.495 0.850
≥70 0.865 0.498–1.502 0.607
LDL cholesterol (mg/dL)
<130 1 Referent
≥130 0.714 0.498–1.023 0.067
Triglyceride (mg/dL)
<150 1 Referent
≥150 1.362 0.998–1.860 0.052
Fasting blood sugar (mg/dL)
<80 1 Referent
80–95 1.136 0.497–2.600 0.762
95–110 1.020 0.443–2.349 0.964
≥110 0.918 0.383–2.202 0.848
HDL, high density lipoprotein; LDL, low density lipoprotein.
P-value <0.05 multiple logistic regression analysis adjusted age and sex.
Ah-ra Koh, et al. Correlation between Colon Polyps, Metabolic Syndrome Parameters, Serum Uric Acid
Korean Journal of Family Practice
KJFP
병률을 분석한 결과 고밀도지단백콜레스테롤, 저밀도지단백콜레 스테롤, 중성지방, BMI, 수축기혈압, 이완기혈압, 허리둘레에서 각 그 룹간의 유병률 차이에서 유의한 값을 보였다(P<0.05). 혈중요산농도 에 따른 차이는 나타나지 않았다(P=0.222) (Table 2).
3. 다변량분석에 의한 대사증후군 관련 지표별 대장용종 유병률의 교차비
관련 변수를 보정하지 않은 상태에서의 각 독립변수들의 대장용 종에 대한 위험비는 총콜레스테롤이 200 mg/dL 미만인 군에 비해 200 mg/dL 이상인 군에서, 고밀도지단백콜레스테롤이 40 mg/dL 미 만인 군에 비해 40 mg/dL 이상에서 70 mg/dL 미만인 군에서와 70 mg/dL 이상인 군에서, 저밀도지단백콜레스테롤이 130 mg/dL 미만 인 군에 비해 130 mg/dL 이상인 군에서 각각 감소하였으나 모두 통 계적으로 유의하지 않았다(P>0.05). 중성지방은 150 mg/dL 미만인 군에 비해 150 mg/dL 이상인 군에서 이완기혈압은 70 mmHg 미만인 군에 비해 70 mmHg 이상에서 80 mmHg 미만인 군과 80 mmHg 이 상에서 90 mmHg 미만인 군과 90 mmHg 이상인 군에서, 허리둘레는 85 cm 미만인 군에 비해 85 cm 이상인 군에서 위험비가 증가하였으 나 통계적으로 유의하지 않았다(P>0.0.5). 공복혈당은 80 mg/dL 미만 인 군에 비해 80 mg/dL 이상에서 95 mg/dL 미만인 군과 95 mg/dL 이 상에서 110 mg/dL 미만인 군에서는 증가하였으나 110 mg/dL 이상인 군에서 감소하였고 통계적으로 유의하지 않았다(P>0.05). 수축기혈 압은 120 mmHg 미만인 군에 비해 120 mmHg 이상에서 130 mmHg 미만인 군과 130 mmHg 이상에서 140 mmHg 미만인 군에서 감소하 였으나 140 mmHg 이상인 군에서 증가하였고 통계적으로 유의하지 않았다(P>0.05). BMI는 reference군인 18.5 kg/m² 미만인 군에 해당하 는 0명이어서 위험비값을 산출할 수 없었다(Table 3).
4. 혈중요산농도에 따른 대장용종발생의 위험비
혼란변수를 보정하지 않은 model 1에서는 혈중요산농도가 3.5
mg/dL 미만인 군에 비해 3.5 mg/dL 이상에서 5.5 mg/dL 미만인 군과 5.5 mg/dL 이상에서 7 mg/dL 미만인 군과 7 mg/dL 이상인 군에서 위 험비가 증가하였으나 통계적으로 유의하지 않았다(P>0.05). 혼란변 수를 보정한 model 3에서 혈중요산농도가 3.5 mg/dL 미만인 군에 비 해 7 mg/dL 이상인 군에서 위험비가 감소하였으나 통계적으로 유의 하지 않았다(P>0.05) (Table 4).
고 찰
대장암은 서구에서 많이 발생하는 암으로 전체 암발생 중 11.5%
를 차지한다고 알려져 있다. 대장암의 대부분은 대장선종에서 발생 하고 선종에서 암성 변화를 일으키는데는 약 5년에서 10년이 걸린 다.15) 한국에서 무증상의 건강검진 수진자에게 진단되는 대장용종 과 대장암의 비율은 18.3%가 대장용종으로 대장암은 0.3%로 알려져 있다.15) 50세 이상의 수진자를 대상으로 분석할 경우 대장용종은 26.3%, 대장암은 0.5%로 획기적으로 증가한다.15) 대사증후군과 대장 암의 공통위험요인으로 복부비만, 신체활동 저하가 알려지면서 다 수의 연구들에서 대사증후군이 동반된 경우 대장암의 위험이 증가 한다고 보고하고 있다.16,17) 본 연구에서 대사증후군 지표별 대장용 종 발생률에 대해 분석한 결과 고밀도지단백콜레스테롤이 낮을수 록 유병률이 높았으며(P=0.045), 중성지방이 높을수록 유병률이 높 았고(P=0.000) BMI가 증가할수록 유병률이 높았으며(P=0.006) 허리 둘레가 증가할수록 유병률이 높았다(P=0.002) (Table 2). 대사증후군 지표 중 중성지방, 허리둘레가 높을수록 대장용종 유병률이 높게 분석되었다. 그러나 다변량회귀분석에서는 통계적으로 유의하지 않 았다(Table 3).
최근 혈청요산농도가 대사증후군의 각각 구성요소와 밀접한 관 련이 밝혀지면서 일부에서는 고요산혈증을 대사증후군의 한 부분 으로 보는 견해도 있다.18,19) 일본인을 대상으로 한 연구에서 혈청요 산농도가 높은 군이 대사증후군의 위험도가 높으며 연령, 성별, 총
Table 4. OR and 95% CI for colon polyps according to uric acid value
Model 1 Model 2 Model 3
OR (95% CI) P-value OR (95% CI) P-value OR (95% CI) P-value
Uric acid (mg/dL)
<3.5 1 1 1
3.5–5.5 1.702 (0.847–3.423) 0.136 1.244 (0.601–2.573) 0.556 1.149 (0.503–2.624) 0.741
5.5–7 1.994 (0.996–3.993) 0.051 1.034 (0.489–2.189) 0.930 1.027 (0.447–2.361) 0.950
≥7 1.762 (0.857–3.623) 0.124 0.860 (0.392–1.884) 0.706 0.943 (0.395–2.251) 0.894
Model 1, not-adjusted. Model 2, adjusted age, sex. Model 3, adjusted age, sex, current smoking, current drinking, hypertension (+), diabetes (+), fasting blood sugar, systolic blood pressure, diastolic blood pressure, abdomen circumference, total cholesterol, high density lipoprotein, low density lipoprotein, triglyceride.
OR, odds ratio; CI, confidence interval.
P-value was calculated by multiple logistic regression analysis.
고아라 외. 대장용종과 대사증후군 지표, 혈중요산농도와의 상관관계 Korean Journal of Family Practice
KJFP
콜레스테롤, 흡연력을 보정한 후에도 의미가 있었다.20) 혈중요산농도 는 인슐린 저항성을 증가시키는데21) 인슐린 저항성이 증가하여 나타 나는 고인슐린혈증은 대장암의 위험요인으로 알려져 있다.22) 본 연 구에서 대장용종은 대장암의 전암병변으로 혈중요산농도와 대장 용종의 상관관계에 대해 연구한 바 대장용종군과 비용종군간의 혈 중요산농도 차이가 유의한 값을 갖지 않았으며(P=0.206) (Table 1) 혈 중요산농도에 따른 대장용종 유병률에 대해서도 유의한 값을 보이 지 않았다(P=0.222) (Table 2). 앞서 밝힌 일본인을 대상으로 한 연구20) 에서와 다른 결과를 보인 이유로는 일본에서 시행한 연구는 10년에 걸쳐 8,144명의 대사증후군 환자 중 인슐린 정보가 축적된 6,339명을 대상으로 혈중요산농도와 대사증후군과의 상관관계를 알아보았으 나 본 연구는 역학적 인자를 도출해내기에는 다소 부족한 연구 대 상자 수와 대장용종군도 305명으로 결과 변수 차이가 희석되었을 가능성이 높을 것으로 생각된다.
또한 혈중요산농도에 따른 대장용종 위험비를 산출하였으며 (Table 4)에서도 혼란변수를 보정하지 않은 Model 1은 혈중요산농도 가 3.5 mg/dL 미만인 군에 비해 3.5 mg/dL 이상에서 5.5 mg/dL 미만인 군과 5.5 mg/dL 이상에서 7 mg/dL 미만인 군과 7 mg/dL 이상인 군에 서 위험도는 증가하였지만 혈중요산농도가 높을수록 위험비가 상 승한 것은 아니며 통계적으로 유의하지 않았다(P>0.05). Model 2, 3에 서 혈중요산농도가 3.5 mg/dL 미만인 군에 비해 7 mg/dL 이상인 군 에서 위험비가 감소하는 값을 보였지만 이는 통계적으로 유의하지 않았다(P>0.05). 이 결과 혈중요산농도가 높을수록 대장용종 발생 위험이 높아지는 상관관계가 없는 것으로 나타났다(Table 3).
본 연구의 제한점으로는 첫째, 일개 종합병원 검진센터를 방문한 수검자를 대상으로한 연구이기 때문에 평소 건강에 관심이 있는 사 람들에 집중되어 있을 가능성이 높아 지역사회 전체를 대표할 수 없 다는 점과 둘째, 통풍에 대한 과거력, 약물 복용력, 운동 등 혈중요산 농도에 영향을 줄 수 있는 다른 혼란 요인은 배제하지 못한 점이다.
셋째, 건강검진 수진자 모집단 중 절반 이상에서 허리둘레 자료가 누 락되어 충분한 표본을 확보하지 못해 통계적 신뢰성이 떨어질 수 있 는 문제점이 있을 수 있다. 향후 연구에서 충분한 대상자를 확보하 여 연구된다면 좀 더 의미 있는 관계를 도출할 수 있을 것이라 생각 한다.
요 약
연구배경:
대장용종은 선암성 병변이며 대사증후군과 관련되어 있 다는 몇몇 연구 결과들이 보고되고 있다. 또한 대사증후군과 혈청요 산농도와의 독립적인 연관성이 있다는 연구들이 보고되고 있다. 이에 저자들은 위험인자로서 대사증후군 지표와 대장용종과의 상관 관계와 예상인자로서 혈중요산농도의 상관관계를 알아보기 위해 본 연구를 시행하였다.
방법:
2011년 1월부터 2014년 12월까지 경기도 수원시 소재 종합병 원 건강증진센터에서 대장내시경을 받은 무증상 성인 3,149명에서 허리둘레를 포함한 신체계측을 시행하지 않고 전대장을 관찰하지 못한 수검자 1,710명과 과거 대장암으로 진단받았거나 조직병리검 사상 대장암으로 확진된 4명의 수검자들을 제외한 1,435명을 대상 으로 후향적으로 분석하였다. 혈중요산농도와 대장용종의 위험비 와 95% 신뢰구간은 다변량로지스틱회귀분석을 이용하여 계산하였 다. 모든 분석은 IBM SPSS 22.0을 이용하여 시행하였다.결과:
검진대상자 1,435명 중에서 대장용종군은 305명이었고 비용 종군은 1,130명으로 유병률은 21.3%였다. 고밀도지단백콜레스테롤, 저밀도지단백콜레스테롤, 중성지방, 체질량지수, 수축기혈압, 이완 기 혈압, 허리둘레에서 각 그룹간의 유병률차이에서 유의한 값을 보 였으나(P<0.05) 로지스틱회귀분석결과 통계적으로 유의하지 않았 다. 혈중요산농도에 따른 유병률 차이가 나타나지 않았고(P=0.222) 혼란변수를 보정한 혈중요산농도에 따른 대장용종 위험비도 유의 하지 않았다(P>0.05).결론:
본 연구에서는 대장용종의 위험인자로 대사증후군 지표의 의미와 예상인자로서 혈중요산농도의 의미가 없는 것으로 확인되 었다.중심단어:
대장용종; 대사증후군 지표; 혈중요산농도 REFERENCES1. Winawer SJ, Zauber AG, Ho MN, O’Brien MJ, Gottlieb LS, Sternberg SS, et al. Prevention of colorectal cancer by colonoscopic polypectomy. The Na- tional Polyp Study Workgroup. N Engl J Med 1993; 329: 1977-81.
2. Borritz M, Rugulies R, Bjorner JB, Villadsen E, Mikkelsen OA, Kristensen TS. Burnout among employees in human service work: design and baseline findings of the PUMA study. Scand J Public Health 2006; 34: 49-58.
3. International Agency for Research Cancer. GLOBOCAN 2012: estimated cancer incidence, mortality and prevalence worldwide in 2012 [Internet].
Lyon: International Agency for Research cancer; 2012. [cited 2012 Apr 1].
Abailable from: http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx.
4. Jung KW, Won YJ, Kong HJ, Oh CM, Cho H, Lee DH, et al. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2012. Cancer Res Treat 2015; 47: 127-41.
5. Chan AT, Giovannucci EL. Primary prevention of colorectal cancer. Gastro- enterology 2010; 138: 2029-43.e10.
6. Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, et al. Diagnosis and management of the metabolic syndrome: an American
Ah-ra Koh, et al. Correlation between Colon Polyps, Metabolic Syndrome Parameters, Serum Uric Acid
Korean Journal of Family Practice
KJFP
Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 2005; 112: 2735-52.
7. Fearnhead NS, Wilding JL, Bodmer WF. Genetics of colorectal cancer: he- reditary aspects and overview of colorectal tumorigenesis. Br Med Bull 2002; 64: 27-43.
8. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cho- lesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evalu- ation, And Treatment of High Blood Cholesterol In Adults (Adult Treat- ment Panel III). JAMA 2001; 285: 2486-97.
9. Terkeltaub R. Update on gout: new therapeutic strategies and options. Nat Rev Rheumatol 2010; 6: 30-8.
10. Cigolini M, Targher G, Tonoli M, Manara F, Muggeo M, De Sandre G. Hy- peruricaemia: relationships to body fat distribution and other components of the insulin resistance syndrome in 38-year-old healthy men and women.
Int J Obes Relat Metab Disord 1995; 19: 92-6.
11. Wang YY, Lin SY, Lai WA, Liu PH, Sheu WH. Association between adeno- mas of rectosigmoid colon and metabolic syndrome features in a Chinese population. J Gastroenterol Hepatol 2005; 20: 1410-5.
12. Park SH. Internal medicine department of catholic university of Korea, co- lon polyps. Korean J Intern Med 2010; 79: S491-4.
13. Lee WC, Neugut AI, Garbowski GC, Forde KA, Treat MR, Waye JD, et al.
Cigarettes, alcohol, coffee, and caffeine as risk factors for colorectal adeno- matous polyps. Ann Epidemiol 1993; 3: 239-44.
14. Bird CL, Frankl HD, Lee ER, Haile RW. Obesity, weight gain, large weight
changes, and adenomatous polyps of the left colon and rectum. Am J Epide- miol 1998; 147: 670-80.
15. Kim MC, Kim DH, Jeong TH. Risk factors of colorectal polyps in Korean adults. J Korean Acad Fam Med 2002; 23: 890-6.
16. Seow A, Yuan JM, Koh WP, Lee HP, Yu MC. Diabetes mellitus and risk of colorectal cancer in the Singapore Chinese health study. J Natl Cancer Inst 2006; 98: 135-8.
17. Ishino K, Mutoh M, Totsuka Y, Nakagama H. Metabolic syndrome: a novel high-risk state for colorectal cancer. Cancer Lett 2013; 334: 56-61.
18. Yun JW, Mook KJ, Lee WY, Kim SW. Plasma uric acid concentrations repre- sent the degree of metabolic control and diabetic complications in type 2 diabetes. Korean J Med 2003; 64: 78-84.
19. Saggiani F, Pilati S, Targher G, Branzi P, Muggeo M, Bonora E. Serum uric acid and related factors in 500 hospitalized subjects. Metabolism 1996; 45:
1557-61.
20. Ishizaka N, Ishizaka Y, Toda E, Nagai R, Yamakado M. Association between serum uric acid, metabolic syndrome, and carotid atherosclerosis in Japa- nese individuals. Arterioscler Thromb Vasc Biol 2005; 25: 1038-44.
21. Desgrippes R, Beauchamp C, Henno S, Bouguen G, Siproudhis L, Bretagne JF. Prevalence and predictive factors of the need for surgery for advanced colorectal adenoma. Colorectal Dis 2013; 15: 683-8.
22. Nilsen TI, Vatten LJ. Prospective study of colorectal cancer risk and physical activity, diabetes, blood glucose and BMI: exploring the hyperinsulinaemia hypothesis. Br J Cancer 2001; 84: 417-22.