허혈성 심장 질환의 진단에서 지난 수십 년간 침습적 관상동 맥 조영술이 표준 검사법으로 자리 잡아 왔으며, 운동부하 심전 도검사(treadmill test), 심근 관류 단일 광자 방출 전산화 단층 촬영술(single photon emission computed tomography, 이하 SPECT), 부하 심장 초음파 등이 비침습적인 진단 방법으로 역할을 하고 있다. 최근 급속한 CT 기술의 발달과 이를 이용 한 진단 방법이 새롭게 대두하고 있다. 따라서 저자들은 허혈 성 심장질환에서 최근 각광을 받는 다절편 CT(multi-detector CT, 이하MDCT) 를 이용한 심장 영상의 임상 적용 및 한계점 그리고 앞으로 발전 방향에 대해 기술하고자 한다.
관상동맥 CT 혈관조영술의 일반적 고찰
심장 영상을 얻는 데 있어 가장 어려운 점은 다른 장기와 달 리 심장이 빠르게 박동하며 움직인다는 것이다. 따라서 관상동 맥 CT 혈관조영술은 시간 해상능의 한계로 말미암아 심장 박 동수가 75-80회 이상이면 빠른 심장 박동에 의한 인공물 (artifact)이 발생할 수 있으며, 관상동맥에 심한 석회화가 있 는 경우 협착이 과장되어 그 정도를 정확히 평가하기가 어렵 다는 단점이 있다. 빠른 심장 박동 이외에도 검사도중 심박동
수가 심하게 변하는 경우에도 영상의 질이 떨어진다(1). 일반 적으로 R-R 간격의 편차가 심한 부정맥이 있거나 인공 심박 동기가 있는 환자, 숨 참기 어려운 중환자에서는 만족할 만한 영상을 얻기 어렵다(2-8). 따라서 검사 전에 이러한 환자를 선별하여 검사 시행 여부를 결정하는 것이 필요하다. 다음으 로, 방사선 피폭과 조영제 사용량을 신중히 고려하여 결정하여 야 한다. 16-절편과 64-절편 MDCT는 기존의 침습적 혈관 조영술의 방사선 피폭량이 3-5 mSv임에 반해 피폭량이 약 6-10 mSv로 방사선 피폭으로 말미암은 위험성이 상대적으로 높으며 SPECT나 양전자 방출 전산화 단층 촬영술(positron emission tomography, 이하 PET)과 같은 방사선 동위원소를 이용한 비침습적 심장 영상검사와 비교하면 피폭량이 낮거나 비슷하지만, 아직은 선별(screening) 검사로 사용하는 것은 적 절하지 않다고 알려졌다(9). 또한, 조영제의 사용량이 16-절 편 MDCT에서는 120-150 mL, 64-절편 MDCT에서는 60- 80 mL로 감소하였다고는 하나 신기능이 나쁜 환자에서는 주 의가 필요하다.
관상동맥 CT 혈관조영술을 이용한 심질환 평가
관상동맥 우회술의 수술 후 평가
관상동맥 우회술후 이식 혈관은 관상동맥과 비교하여 내경 이 크고 심장의 움직임에 따른 영향이 상대적으로 작아서, 관 상동맥 영상을 얻을 때 문제가 되는 심박수, 호흡에 의한 변화, 후향적 영상 재구성시의 심장 주기 선택에 따른 영향을 비교 적 덜 받는다(10). 따라서 관상동맥우회로 수술 후 침습적 관
관상동맥 전산화단층촬영 혈관조영술: 새로운 진단기법으로서 임상에서의 적응증 및 역할을 중심으로1
김동훈・최상일2・전은주2・장성아3・최의근3・장혁재3・최동주3・이 활4・박재형4
허혈성 심질환의 진단을 위해 다양한 침습적, 비침습적인 영상방법들이 사용되어왔다. 아직 몇 가지 제한점에도, 최근 급속도로 발전하고 있는 관상동맥 전산화 단층촬영 혈관조영술(이 하 관상동맥 CT혈관조영술)은 관상동맥 질환이 의심되는 환자에서 이용빈도가 대폭 증가하 고 있다. 하지만, 아직까지 관상동맥 CT혈관조영술의 뛰어난 진단성적에도, 실제 관상동맥 질 환이 의심되는 환자에서 여러 가지 다른 비침습적 진단기법과 비교하여 관상동맥 CT혈관조 영술의 역할 및 적응증이 충분히 확립되어 있지 않으며, 아직도 이에 대한 많은 연구가 진행 중이다. 이에 기존에 발표된 자료들과 저자들의 경험을 바탕으로 관상동맥 질환이 의심되거나 확진된 환자에서 관상동맥 CT혈관조영술의 새로운 진단기법으로서의 역할 및 적응증을 제시 하고자 한다.
1조선대학교 의과대학 영상의학과교실
2분당서울대학교병원 진단방사선과학교실
3분당서울대학교병원 심장센터
4서울대학교병원 진단방사선과학교실
이 논문은 2006년 62차 대한영상의학회 학술대회“Best Scientific Exhibition Award”“금상”수상작으로 학회의 요청으로 준비되었음.
이 논문은 2006년 11월 22일 접수하여 2007년 3월 7일에 채택되었음.
상동맥 조영술을 대신하여 이식혈관의 개통성(patency)을 평 가하는 목적으로 널리 사용되고 있다. 많은 연구를 통해 관상 동맥 CT 혈관조영술이 침습적 혈관 조영술 대비 95% 이상의 민감도와 특이도가 있음이 알려졌다(11-13). 그러나 수술 시 사용되는 금속편이 이식 혈관에 너무 근접하여 있는 경우 인 공물에 의해 이식부위의 혈관을 평가하기 어려울 수 있다. 관 상동맥 CT 혈관조영술은 관상동맥 우회술을 받은 환자에서 다 시 개심술이 필요하거나 최소 침습수술(minimal invasive surgery)을 계획하는 경우에 상행대동맥의 석회화, 이식혈관 또는 목표혈관의 위치확인과 절개부위의 선택 등 수술계획을 세우는 데 큰 도움을 준다(14, 15).
관상동맥 및 심기능 평가 관상동맥 협착 평가
많은 연구에서 관상동맥 CT 혈관조영술은 관상동맥의 협착 을 평가에 하는데 있어 민감도와 음성 예측도가 90% 이상으 로 매우 높았다. 16-절편 MDCT를 이용한 연구 결과 높은 심 박동수를 가진 환자나 1.5 mm 이하의 작은 관상동맥, 기술적 인 한계 때문에 평가가 불가능하였던 증례를 포함하여 다시 분 석해 보면 실제 정확도는 약 80-85%에 불과하다(16-20).
최근 도입된 64-절편 MDCT를 이용한 연구에서는 높은 심박
동수를 가진 환자와 1.5 mm 이하의 작은 관상동맥을 분석대 상에 포함하고도 90% 이상의 민감도, 특이도와 음성 예측도 를 보고하고 있다(21-23). 현재의 기술적인 조건을 고려한다 면 95% 이상의 높은 음성 예측도를 이용하여, 관상동맥질환 의 중등도(intermediate) 위험군 환자, 다른 비 침습적 검사에 서 애매한(equivocal) 결과를 보이는 경우, 또는 저(low) 위험 군 환자에서 다른 이유로 침습적 관상동맥 조영술이 필요한 경 우 등을 우선으로, 관상동맥 CT 혈관조영술의 적응증으로 하 는 것이 가장 바람직하다고 생각된다.
관상동맥 위험반 평가
오래전부터 조영제를 사용하지 않고 소용량의 방사선만으로 관상동맥의 석회화 정도를 정량화하여, 이를 선별검사로 이용 하고자 하였다. 많은 연구에서 관상동맥의 석회화 점수가 비석 회화된 위험반(vulnerable plaque)을 포함한 관상동맥 반 (plaque)의 총량과 비교적 상관성이 높고 앞으로 발생할 심장 질환을 예측하는 데에도 도움이 된다고 알려져 있다. 하지만 인종, 나이에 따라 관상동맥 석회화 점수의 해석이 다르다는 문제가 있으며, 특히 급성 관동맥 증후군의 주원인인 위험반을 발견하기 어렵다는 심각한 문제점이 있다. 그럼에도, 현재까지 연구결과를 바탕으로 관상동맥의 석회화 정도의 평가는 중년
A B
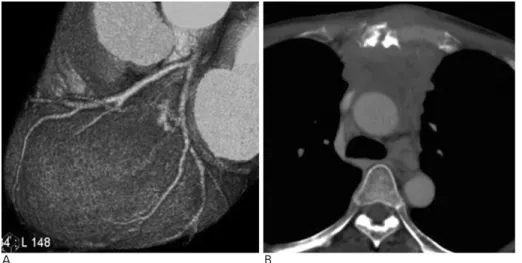
Fig. 1. A 61-year-old man with contin- uous radiating chest pain to the back.
Treadmill test (TMT), Holter, and echocardiograpy showed no abnormal findings.
A. Volume-rendered image shows nor- mal coronary arteries.
B. Axial CT scan shows localized thick- ening of anterior pericardium (arrow).
Pericarditis was confirmed clinically.
A B
Fig. 2. A 37-year-old man with atypical chest pain.
A. Volume-rendered image demon- strates normal coronary arteries.
B. End-systolic image on 4 chamber view shows dilatation of left ventricle.
Ejection fraction measured by cardiac MDCT was 25.6% and dilated car- diomyopathy was clinically proved.
의 관상동맥 고(high) 위험군 환자에서 추천되고 있으며, 관상 동맥 CT 혈관조영술의 판독에도 도움을 줄 수 있다고 알려졌 다.
관상동맥 CT 혈관조영술의 가장 큰 장점은 허혈성 심장 질 환을 진단하는데 있어 관상동맥의 협착 정도뿐만 아니라 급성 관상동맥 증후군을 유발하는 죽상경화반 (atherosclerotic plaque)의 특성을 비침습적으로 영상화할 수 있어서 이를 조 기에 발견하고 쉽게 추적관찰 할 수 있다는 점이다. 관상동맥 CT 혈관조영술과 혈관 내 초음파(intravascular ultrasound)와 비교한 연구 결과, 위험반은 저음영 원주상의 병변으로 50 HU(Hounsfield Unit) 내외로 낮은 수치로 보이며, 급성 심근 경색에서 혈전은 20 HU, 섬유화반(fibrous plaque)은 90 HU, 석회화가 동반된 위험반은 130 HU 이상으로 측정된다(24).
그러나 아직 관상동맥 CT 혈관조영술은 공간 해상능의 한계 로 말미암아, 근위부 분절(proximal segment)에만 국한되어 진단할 수 있으며 위험반의 특성과 면적의 분석, 재형성 (remodeling)의 평가 소견은 혈관 내 초음파와 비교적 일치하 지만 협착 정도의 평가에는 두 검사 간에 어느 정도 차이를 보
인다(25-28).
심장 기능 평가
관상동맥 CT 혈관조영술은 추가적인 검사를 하지 않고도 심 장 용적 및 기능에 대한 정보를 제공한다. 이면성 심초음파와 다르게 용적의 측정에서, 연속적인 영상 단면의 심실을 모두 측정하기 때문에 매우 정확하며 재현성이 높다. 그러나 이를 위한 별도의 소프트웨어가 필요하며, 추가로 많은 영상을 재구 성해야 하므로 많은 시간과 인력이 소모된다. 심실 수축기능 연구에서 심장 자기공명 영상에서 얻어진 수치를 표준으로 하 여 비교하였을 때, 관상동맥 CT 혈관조영술이 심초음파나 SPECT보다 정확하며, 우심실 용적과 기능도 정확히 측정할 수 있다(29-31). 그러나 시간 해상능의 한계로 말미암아, 정 확히 심실의 이완기말 최대용적과 수축기말 최소용적을 얻지 못해 심실 구혈율이 작게 측정될 수 있으며 이완기능을 측정 할 수 없다. 이런 단점과 방사선 피폭을 고려해보면 심장 기능 의 평가를 위하여 일차적으로 MDCT를 사용하는 것은 바람직 하지 않다.
A B C
Fig. 3. A 43-year-old man with atypical chest pain.
A. Volume-rendered image shows normal coronary arteries.
B, C. Two chamber multiplanar reformatted (MPR) views in end-diastole (B) and end-systolic (C) phases represent apical hypertro- phy of left ventricle (hypertrophic cardiomyopathy).
A B
Fig. 4. A 61-year-old woman with con- tinuous chest pain during one year.
A. Volume-rendered image shows no abnormality in coronary arteries.
B. Axial CT scan shows bulky mass in anterior mediastinum with destructed sternum. Thymic carcinoma was proved by biopsy.
심근 관류 및 생존능 평가
중등도 이상의 관상동맥 협착에도 안정 시에는 보상성 혈관 확장에 의해 관류량이 유지되어 있으므로, 관상동맥 CT 혈관 조영술을 이용하여 관상동맥 협착부위 이하의 관류감소를 평 가함으로써 의미 있는 동맥 협착을 찾는 것은 매우 어렵다. 하 지만, 급성 심근경색환자에서 관상동맥의 완전 폐색이나 미세 혈관 폐색(microvascular obstruction)이 발생하면, 조영제 주 입 후 심근의 조영증강이 정상심근에 비하여 감소하여 나타난 다. 한 연구에 의하면 정상 심근, 급성과 만성 심근 경색에서 심근의 조영증강 정도는 각각 73±14 HU, 26±26 HU, -13
±37 HU으로 구별이 쉽다고 보고하였다(32).
조영제 주입 후 5-10분 후에 추가로 지연 영상을 얻게 되 면 심근 경색 부위에 지연기 조영증강(delay enhancement)이 발생하며 자기공명 영상에 의한 심근 경색 부위 평가와 비교 하여 잘 일치한다고 알려졌다(33-36). 하지만, 심근 관류 및 생존능을 평가하려면 추가적인 검사를 시행하여야 하므로, 이
때문에 방사선 피폭이 증가한다는 단점이 있어서 앞으로 이 검 사들의 유용성에 대한 임상 연구가 필요하다.
판막 질환 평가
현재까지 판막질환을 평가하고자) 관상동맥 CT 혈관조영술 이 일차적으로 추천되고 있지는 않으나, 최근에 관상동맥 CT 혈관조영술의 유용성이 보고되고 있다. 특히 대동맥 협심증 (aortic angina)이라고 불리는 대동맥 협착과 같은 대동맥 판 막 질환에서 판막의 형태와 협착 정도 등을 평가하는데에서 관 상동맥 CT 혈관조영술은 심초음파와 같은 결과를 보이며, 대 동맥 기시부(aortic root)와 상행대동맥의 직경 평가에 매우 용 이 하므로 사용이 점차 증가하고 있다.
A B C
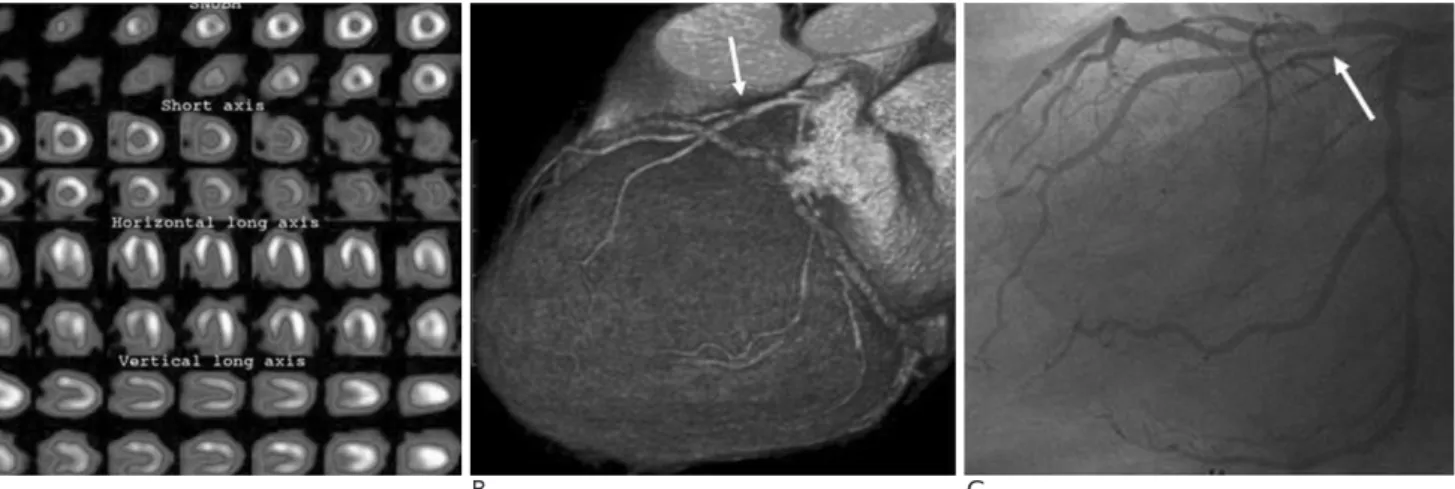
Fig. 6. A 55-year-old man with dyspnea on exertion.
A. SPECT shows no significant perfusion defect. 3D volume-rendering image (B) and selective coronary angiography (C) shows high grade discrete stenosis (75%) of proximal LAD (arrow).
A B C
Fig. 5. A 72-year-old woman with dyspnea during two months. A. SPECT (single positron emission CT) shows normal finding.
B. Axial CT scan shows severe discrete stenosis (80%) at left main coronary artery (arrow).
C. Selective coronary angiography also shows severe stenosis at left main coronary artery (arrow) and is very well correlated with CT coronary angiography (arrow in B).
관상동맥 질환에서의
관상동맥 CT 혈관조영술의 임상적용
기존의 관상동맥질환의 비침습적 진단법은 의미 있는 혈관 협착이 있는 경우에 생기는 심장의 병태생리학적 변화에 근거 하여 진단이 이루어져 왔다. 하지만, 관상동맥 CT 혈관조영술 은 다른 비침습적 진단법과는 달리 관상동맥 내강의 의미 있 는 협착이 생기기 이전 단계에서의 혈관벽의 변화, 즉 동맥 경 화와 위험반을 평가할 수 있다는 장점이 있다.
비전형적 흉통
현재 관상동맥 CT 혈관조영술이 임상에서 가장 많이 사용 되는 것은 95% 이상의 높은 음성 예측도를 이용하여 경도 또 는 중등도의 관상동맥 질환의 위험성이 있는 비전형적 흉통 환 자에서 관상동맥질환을 배제하고자 사용되는 경우이다(Fig.
1-4). CT검사는 심장뿐만 아니라 폐, 종격동, 흉벽 등 심장 이외에서 기인하는 흉통을 진단하는 데 유용하므로 한 번의 검 Fig. 7. A 41-year-old man with acute chest pain. ECG showed
block of left bundle branch, ST elevation in V1 to V4 lead, and hyperacute T wave. Clinically, STEMI (ST elevated myocar- dial infarction) was suspected. However, axial CT scan shows intramural hematoma with overt aortic dissection (arrows).
A B
Fig. 8. A 40-year-old man with acute chest pain. ECG and cardiac enzymes were within normal limits. Axial CT scan (A) and short axis view (B) show bulky thrombi within proximal LAD.
Final diagnosis is NSTEMI (non-STE- MI) at proximal LAD due to thrombot- ic occlusion.
A B C
Fig. 9. A 53-year-old man with acute atypical chest pain. ECG and cardiac enzymes were within normal limits. Axial CT scans show thrombotic occlusion at proximal LCX (arrow in A) with subendocardial perfusion defect (arrow in B). Short axis viewon end-systolic phase represents akinesia at mid to basal lateral wall (C).
사로 많은 정보를 얻을 수 있다(37-39).
부하 검사에서 애매한 결과를 보이는 고 위험군의 환자
관상동맥 CT 혈관조영술은 비교적 낮은 양성 예측률로 인 하여 아직은 일차적 또는 독자적인 검사기법으로 확립되어 있 지 않다. 하지만, 운동 부하 심전도 검사나 SPECT와 같은 부 하검사에서 애매한 결과를 보이는 안정형 협심증 환자 또는 고
혈압이나 2형 당뇨를 앓은 고 위험군의 환자에서 관상동맥 CT 혈관조영술을 시행함으로써 불필요한 고식적 관상동맥 조영술 을 감소시킬 수도 있다(Fig. 5, 6) (40-43).
관상동맥 폐색의 중재적 시술 전 평가
관상동맥의 만성 완전 폐색(chronic total occlusion)을 보이 는 환자에서 중재적 시술 실패의 주요 원인은 폐색 길이
A B
Fig. 10. A 54-year-old man with chest pain on exertion.
A. Short axis MPR image shows chronic total occlusion due to mainly fibrous plaque at mid-RCA (arrow).
B. Vessel analysis using dedicated soft- ware represents relatively short seg- mental occlusion (1.06 cm) at mid- RCA and no evidence of calcified plaque. Revascularization by percuta- neous coronary intervention was suc- cessfully done.
A B
Fig. 12. A 44-year-old man with atypi- cal chest pain. Myocardial bridging of LAD that is distinct artery within my- ocardium is seen in short axis MPR view on systole (arrow in A) and dias- tole (arrow in B).
A B
Fig. 11. A 58-year-old man with chest pain on exertion.
A. Volume rendered image shows dif- fuse chronic total occlusion (3.51 cm) from proximal LAD with multifocal dense calcified plaques.
B. Selective coronary angiography also shows total occlusion at proximal LAD. Percutaneous coronary inter- vention was failed and coronary artery bypass graft was done.
(occlusion length)가 길거나 심한 석회화(severe calcification) 가 있는 경우로, 관상동맥 CT 혈관조영술은 관상동맥의 3차원 적인 폐색 길이와 석회화 정도의 평가에서 고식적 혈관조영술 에 비하여 더 많은 정보를 제공하여 주므로 시술 전 대상환자 선정 및 치료계획을 세우는데 유용하다(Fig. 7, 8) (44).
급성 관동맥 증후군
64절편 MDCT의 도입으로 심전도 동기하에 흉부 CT 검사 가 가능해짐에 따라 급성 흉통의 3대 중요한 원인인 대동맥 박 리, 폐색전증과 급성 관동맥 증후군을 한 번에 평가할 수 있다 (소위“triple rule-out”) (Fig. 9), 따라서 원인이 명확하지 않 은 급성 흉통을 주소로 내원한 환자를 이른 시일 내에 감별 진 단함으로써 효율적인 치료가 가능하게 되었다(Fig. 10, 11) (45, 46). 급성 관동맥 증후군에서 관상동맥 CT 혈관조영술을 시행함으로써 치료방침을 결정하는데 도움이 되었다는 연구도 있으며 이러한 용도로 MDCT의 이용은 앞으로 추가적인 연구 결과를 기다려 볼 필요가 있다(47).
관상동맥 우회술의 수술 전 평가
관상동맥 우회로 수술 전의 환자 평가에서 관상동맥 CT 혈 관조영술은 고식적 관상동맥 조영술과 비교하여 문합부위의 선 정(target anastomotic site)을 위한 석회화된 위험반의 발견, 문합부위의 직경 평가와 심근 교(myocardial bridging) 유무를 평가하는 데 있어 매우 유용하다(Fig. 12). 또한, 심막 외 지 방조직 속에 깊이 위치한 관상동맥 혈관을 3차원적으로 평가 할 수 있어 수술 계획 수립에 도움을 준다(Fig. 13) (48, 49).
관상동맥 스텐트 시술 후의 재협착 평가
관상동맥 스텐트 시술 후 이의 개통성과 재협착 유무를 평 가하는 것은 매우 중요하다. 그러나 현재까지 관상동맥 CT 혈 관조영술을 이용한 스텐트 내의 재협착 평가는 매우 어려운데, 이는 스텐트 재질에 따라 금속 성분이 많이 포함될수록 잘 발 생하게 되는 인공음영(beam hardening artifact)과 부족한 공 간 해상능 때문으로, 앞으로 좀 더 많은 연구와 기술의 발전이 필요하다. 현재까지 16-절편과 40-절편 MDCT를 이용한 연 구결과에 따르면 좌주 관상동맥(left main coronary artery)의 스텐트 평가에서 35% 이상의 재협착이 있는 경우 유용하며 (50), 또한 3 mm 이상의 직경과 지주(strut)의 두께가 140 μ m 이하이면 스텐트 내 재협착 유무의 평가가 가능하다는 보 고가 있다(Fig. 14) (51, 52).
관상동맥의 정상 변이 및 선천성 기형
대동맥과 폐동맥 사이를 관상동맥이 지나는 경우 운동이나 스트레스시 심근 허혈이나 급사가 생길 수 있다. 관상동맥 CT 혈관조영술은 관상동맥의 주행 경로 이외에도 대혈관과의 관 계를 입체적으로 확인할 수 있다는 장점이 있다(Fig. 15). 이 외에도 관상동맥루나 관상동맥류를 포함한 각종 정상 변이 및 선천성 기형 소견들에서 진단이 쉽다(Fig. 16) (53, 54). 고식 적인 관상동맥 혈관조영술에서 변이 또는 기형의 평가가 애매 한 경우에 확진을 위해 관상동맥 CT 혈관조영술을 유용하게 사용할 수 있다.
A B
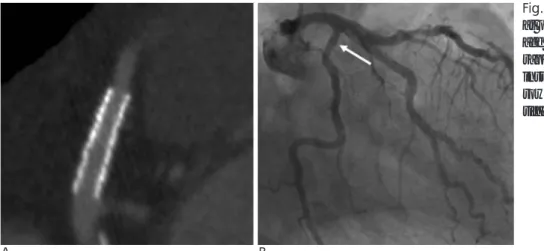
Fig. 14. A 61-year-old man with stent at proximal LCX. Short axis MPR im- age (A) and selective coronary angiog- raphy (B) show wide patency without instent restenosis at proximal LCX (ar- row) even though minor blooming ar- tifact.
Fig. 13. A 47-year-old man with typical chest pain. Short axis view shows coronary artery buried within profuse epicardial fat.
무증상의 관상동맥 위험군 환자의 선별검사
비록 아직은 무증상을 가진 환자에서 관상동맥 CT 혈관조 영술은 관상동맥 위험군 환자에서 선별검사로 추천되지는 않 지만, 앞으로 이의 유용성에 대한 연구가 필요하다. 하지만, 실 제 MDCT가 설치된 많은 병원에서 관상동맥 CT 혈관조영술
이 건강검진 목적으로 이용되고 있으며, 이의 남용에 대한 우 려의 목소리도 높다. 하지만, 당뇨병을 비롯하여 심장질환의 위 험도가 높은 무증상의 관상동맥 질환 위험군에서 관상동맥 CT 혈관조영술은 유용한 선별검사 방법으로서 사용될 수 있다(Fig.
17).
A B
Fig. 16. A 28-year-old man with con- genital coronary arteriovenous fistula.
A, B. 3D volume-rendering images shows coronary arteriovenous fistula arising from RCA and draining into main pulmonary trunk (arrows).
A B C
Fig. 17. A 44-year-old man with asymptom. 3D volume-rendering image (A) and magnified short axis view (B) show severe discrete stenosis (75 %) at mid-LAD (arrow) due to vulnerable plaque with positive arterial remodeling.
C. Selective coronary angiography shows high grade discrete stenosis of mid-LAD (arrow).
A B
Fig. 15. A 61-year-old man with con- genital anomaly of coronary artery.
Anomalous origin of right coronary artery from left coronary sinus and un- usual passing route between aortic root and pulmonary trunk are well demonstrated (arrow in A and B).
결 론
관상동맥 CT 혈관조영술은 향상된 공간분해능과 짧은 스캔 시간으로 비약적인 발전을 이루었으나, 아직도 여러 가지 해결 해야 하는 문제점이 있다. 그러나, 1초 이하의 짧은 스캔 시간 을 보이는 256-절편 MDCT와 같은 다음 세대의 CT는 문제 점들을 대부분 극복할 것으로 보여, 1-2년 이내에 관상동맥영 상을 포함한 심장 검사에 새로운 전기를 마련해 줄 것으로 기 대된다(55). 또한 심장 MRI와 마찬가지로 관상동맥 CT 혈관 조영술은 PET과 결합하여 허혈성 심질환에서 비침습적인
“one- stop”검사법으로서 발전할 가능성이 있다(56). 아직 허혈성 심질환이 의심되는 환자에 있어 기존의 비침습적인 진 단방법인 운동부하 심전도 검사, 심근 SPECT와 비교하여 관 상동맥 CT 혈관조영술은 일차적으로 사용되는 있지는 않으나 점차 그 역할이 증가할 것이므로 다양한 검사들의 역할에 대 한 점검이 필요하다. 즉, 일차적으로 관상동맥 CT 혈관조영술 을 시행하여 그 결과가 애매하거나 혈역학적 의미를 알기 어 려운 중등도의 협착이 있는 경우에 심근 SPECT를 시행할 수 있으며, 관상동맥 CT 혈관조영술로 평가가 어려운 석회화의 빈도가 높은 고령의 환자에서는 일차적으로 심근 SPECT를 시 행하는 것과 같은 역할 분담이 필요하다(57). 또한 운동부하 심전도 검사와 심근 SPECT는 심장의 기능적 이상을 평가하 는 반면, 관상동맥 CT 혈관조영술은 해부학적 이상을 잘 평가 하므로, 운동 부하 심전도와 관상동맥 CT 혈관조영술을 동시 에 일차적으로 시행하는 방법도 유용하다고 할 수 있다(Fig.
18) (58). 그러나 이에 앞서 정확한 임상적용과 신뢰할 수 있 는 결과를 얻으려면 검사의 장점, 단점과 한계점을 명확히 이 해하고 이에 대한 많은 연구가 선행되어야 한다. 결론적으로 관상동맥 CT 혈관조영술은 지속적인 기술 발전과 더불어 좀 더 정확한 형태적인 관찰뿐만 아니라 다양한 기능적인 검사를 상용화시킬 것이며, 그 임상적용은 비약적으로 증가 될 것으로 기대된다.
참 고 문 헌
1. Leschka S, Wildermuth S, Boehm T, Desbiolles L, Husmann L, Plass A, et al. Noninvasive coronary angiography with 64-section CT: effect of average heart rate and heart rate variability on image quality. Radiology 2006;241:378-385
2. Nieman K, Cademartiri F, Lemos PA, Raaijmakers R, Pattynama PM, de Feyter PJ. Reliable noninvasive coronary angiography with fast submillimeter multislice spiral computed tomography.
Circulation 2002;106:2051-2054
3. 김동훈, 최상일, 이경원, 강성권, 최성훈, 서준범 등. 다절편 전산화 단층촬영을 이용한 관상동맥영상: 1부 기술적 측면. 대한영상의학 회지 2004;51:401-408
4. 김동훈, 최상일, 이경원, 장혁재, 정우영, 채인호 등. 다절편 전산화 단층촬영을 이용한 관상동맥영상: 2부 임상적 측면. 대한영상의학 회지 2004;51:409-416
5. Ropers D, Baum U, Pohle K, Anders K, Ulzheimer S, Ohnesorge B, et al. Detection of coronary artery stenoses with thin-slice multi- detector row spiral computed tomography and multiplanar recon- struction. Circulation 2003;107:664-666
6. Schoenhagen P, Halliburton SS, Stillman AE, Kuzmiak SA, Nissen SE, Tuzcu EM, et al. Noninvasive imaging of coronary arteries:
current and future role of multi-detector computed tomography.
Radiology 2004;232:7-17
7. Schoepf UJ, Becker CR, Ohnesorge BM, Yucel EK. CT of coronary artery disease. Radiology 2004;232:18-37
8. Hoffmann MH, Shi H, Manzke R, Schmid FT, De Vries L, Grass M, et al. Noninvasive coronary angiography with 16-detector row CT: effect of heart rate. Radiology 2005;234:86-97
9. Donnelly PM, Higginson JD, Hanley PD. Multidetector CT coro- nary angiography: have we found the holy grail of non-invasive coronary imaging? Heart 2005;91:1385-1388
10. Willmann JK, Weishaupt D, Kobza R, Verdun FR, Seifert B, Marincek B, et al. Coronary artery bypass grafts: ECG-gated mul- ti?detector row CT angiography-influence of image reconstruction interval on graft visibility. Radiology 2004;232: 568-577
11. Song MH, Ito T, Watanabe T, Nakamura H. Multidetector comput- ed tomography versus coronary angiogram in evaluation of coro- nary artery bypass grafts. Ann Thorac Surg 2005;79:585-588 12. Schlosser T, Konorza T, Hunold P, Kuhl H, Schmermund A,
Barkhausen J. Noninvasive visualization of coronary artery bypass Fig. 18. Approach to diagnosis and management of coronary artery dis- ease (CAD) in symptomatic patients using coronary CTA, TMT and stress SPECT or PET. This diagram is modi- fied form from that of Berman DS et al (ref. 58).
grafts using 16-detector row computed tomography. J Am Coll Cardiol 2004;44:1224-1229
13. Martuscelli E, Romagnoli A, D’Eliseo A, Tomassini M, Razzini C, Sperandio M, et al. Evaluation of venous and arterial conduit pa- tency by 16-slice spiral computed tomography. Circulation 2004;110:3234-3238
14. Gilkeson RC, Markowitz AH, Ciancibello L. Multisection CT eval- uation of the reoperative cardiac surgery patient. Radiographics 2003;23:S3-S17
15. Aviram G, Sharony R, Kramer A, Nesher N, Loberman D, Ben-Gal Y, et al. Modification of surgical planning based on cardiac multi- detector computed tomography in reoperative heart surgery. Ann Thorac Surg 2005;79:589-595
16. Kuettner A, Beck T, Drosch T, Kettering K, Heuschmid M, Burgstahler C, et al. Diagnostic accuracy of noninvasive coronary imaging using 16-detector slice spiral computed tomography with 188 ms temporal resolution. J Am Coll Cardiol 2005;45:123-127 17. Kuettner A, Kopp AF, Schroeder S, Rieger T, Brunn J, Meisner C,
et al. Diagnostic accuracy of multidetector computed tomography coronary angiography in patients with angiographically proven coronary artery disease. J Am Coll Cardiol 2004;43:831-839 18. Mollet NR, Cademartiri F, Krestin GP, McFadden EP, Arampatzis
CA, Serruys PW, et al. Improved diagnostic accuracy with 16-row multi-slice computed tomography coronary angiography. J Am Coll Cardiol 2005;45:128-132
19. Martuscelli E, Romagnoli A, D’Eliseo A, Razzini C, Tomassini M, Sperandio M, et al. Accuracy of thin-slice computed tomography in the detection of coronary stenoses. Eur Heart J 2004;25:1043- 1048
20. Morgan-Hughes GJ, Roobottom CA, Owens PE, Marshall AJ.
Highly accurate coronary angiography with submillimetre, 16 slice computed tomography Heart 2005;91:308-313
21. Leschka S, Alkadhi H, Plass A, Desbiolles L, Grunenfelder J, Marincek B, et al. Accuracy of MSCT coronary angiography with 64-slice technology: first experience. Eur Heart J 2005;26:1482- 1487
22. Raff GL, Gallagher MJ, O’Neill WW, Goldstein JA. Diagnostic ac- curacy of noninvasive coronary angiography using 64-slice spiral computed tomography. J Am Coll Cardiol 2005;46:552-557 23. Mollet NR, Cademartiri F, van Mieghem CA, Runza G, McFadden
EP, Baks T, et al. High-resolution spiral computed tomography coronary angiography in patients referred for diagnostic conven- tional coronary angiography. Circulation 2005;112: 2318-2323 24. Leber AW, Knez A, Becker A, Becker C, von Ziegler F, Nikolaou
K, et al. Accuracy of multidetector spiral computed tomography in identifying and differentiating the composition of coronary athero- sclerotic plaques: a comparative study with intracoronary ultra- sound. J Am Coll Cardiol 2004;43:1241-1247
25. Leber AW, Knez A, von Ziegler F, Becker A, Nikolaou K, Paul S, et al. Quantification of obstructive and nonobstructive coronary le- sions by 64-slice computed tomography: a comparative study with quantitative coronary angiography and intravascular ultrasound. J Am Coll Cardiol 2005;46:147-154
26. Leber AW, Becker A, Knez A, von Ziegler F, Sirol M, Nikolaou K, et al. Accuracy of 64-slice computed tomography to classify and quantify plaque volumes in the proximal coronary system: a com- parative study using intravascular ultrasound. J Am Coll Cardiol 2006;47:672-677
27. Achenbach S, Ropers D, Hoffmann U, MacNeill B, Baum U, Pohle K, et al. Assessment of coronary remodeling in stenotic and non- stenotic coronary atherosclerotic lesions by multidetector spiral computed tomography. J Am Coll Cardiol 2004;43:842-847
28. Achenbach S, Moselewski F, Ropers D, Ferencik M, Hoffmann U, MacNeill B, et al. Detection of calcified and noncalcified coronary atherosclerotic plaque by contrast-enhanced, submillimeter multi- detector spiral computed tomography: a segment-based compari- son with intravascular ultrasound. Circulation 2004;109:14 -17 29. Yamamuro M, Tadamura E, Kubo S, Toyoda H, Nishina T, Ohba
M, et al. Cardiac functional analysis with multi-detector row CT and segmental reconstruction algorithm: comparison with echocardiography, SPECT, and MR imaging. Radiology 2005;234 :381-390
30. Juergens KU, Fischbach R. Left ventricular function studied with MDCT. Eur Radiol 2006;16:342-357
31. Lembcke A, Dohmen PM, Dewey M, Klessen C, Elgeti T, Hermann KA, et al. Multislice computed tomography for preoper- ative evaluation of right ventricular volumes and function: com- parison with magnetic resonance imaging. Ann Thorac Surg 2005;79:1344-1351
32. Nieman K, Cury RC, Ferencik M, Nomura CH, Abbara S, Hoffmann U, et al. Differentiation of recent and chronic myocar- dial infarction by cardiac computed tomography. Am J Cardiol 2006;98:303-308
33. Mahnken AH, Koos R, Katoh M, Wildberger JE, Spuentrup E, Buecker A, et al. Assessment of myocardial viability in reperfused acute myocardial infarction using 16-slice computed tomography in comparison to magnetic resonance imaging. J Am Coll Cardiol 2005;45:2042-2047
34. Lardo AC, Cordeiro MA, Silva C, Amado LC, George RT, Saliaris AP, et al. Contrast-enhanced multidetector computed tomography viability imaging after myocardial infarction: characterization of myocyte death, microvascular obstruction, and chronic scar.
Circulation 2006;113:394-404
35. Gerber BL, Belge B, Legros GJ, Lim P, Poncelet A, Pasquet A, et al.
Characterization of acute and chronic myocardial infarcts by mul- tidetector computed tomography: comparison with contrast-en- hanced magnetic resonance. Circulation 2006;113:823-833 36. Koyama Y, Matsuoka H, Mochizuki T, Higashino H, Kawakami H,
Nakata S, et al. Assessment of reperfused acute myocardial infarc- tion with two-phase contrast-enhanced helical CT: prediction of left ventricular function and wall thickness. Radiology 2005;235:
804-811
37. Herzog C, Britten M, Balzer, Mack MG, Zangos S, Ackermann H, et al. Multidetector-row cardiac CT: diagnostic value of calcium scoring and CT coronary angiography in patients with sympromat- ic, but atypical, chest pain. Eur Radiol 2004;14:169-177
38. Schmermund A, Erbel R. Non-invasive computed tomographic coronary angiography: the end of the beginning. Eur Heart J 2005;26:1451-1453
39. Garcia MJ. Noninvasive coronary angiography: hype or new para- digm? JAMA 2005; 293:2531-2533
40. Hoffmann U, Moselewski F, Cury RC, Ferencik M, Jang IK, Diaz LJ, et al. Predictive value of 16-slice multidetector spiral computed tomography to detect significant obstructive coronary artery dis- ease in patients at high risk for coronary artery disease: patient-ver- sus segment-based analysis. Circulation 2004;110:2638-2643 41. Mollet NR, Cademartiri F, Nieman K, Saia F, Lemos PA,
McFadden EP, et al. Multislice spiral CT coronary angiography in patients with stable angina pectoris. J Am Coll Cardiol 2004;43:
2265-2270
42. Schuijf JD, Bax JJ, Jukema JW, Lamb HJ, Vliegen HW, van der Wall EE, et al. Noninvasive evaluation of the coronary arteries with multislice computed tomography in hypertensive patients.
Hypertension 2005;45:227-232
43. Schuijf JD, Bax JJ, Jukema JW, Lamb HJ, Vliegen HW, Salm LP, et al. Noninvasive angiography and assessment of left ventricular function using multislice computed tomography in patients with type 2 diabetes. Diabetes Care 2004;27:2905-2910
44. Mollet NR, Hoye A, Lemos PA, Cademartiri F, Sianos G, McFadden EP, et al. Value of preprocedure multislice computed tomographic coronary angiography to predict the outcome of per- cutaneous recanilization of chronic total occlusion. Am J Cardiol 2005;95:240-243
45. White CS, Kuo D, Kelemen M, Jain V, Musk A, Zaidi E, et al.
Chest pain evaluation in the emergency department: can MDCT provide a comprehensive evaluation? Am J Roentgenol 2005;185:
533-540
46. Ghersin E, Litmanovich D, Dragu R, Rispler S, Lessick J, Ofer A, et al. 16-MDCT coronary angiography versus invasive coronary an- giography in acute chest pain syndrome: a blinded prospective study. AJR Am J Roentgenol 2006;186:177-184
47. Dorgelo J, Willems TP, Geluk CA, Ooijen PM, Zijlstra F, Oudkerk M. Multidetector computed tomography-guided treatment strategy in patients with non-ST elevation acute coronary syndromes: a pi- lot study. Eur Radiol 2005;15:708-713
48. Herzog C, Dogan S, Diebold T, Khan MF, Ackermann H, Schaller S, et al. Multi-detector row CT versus coronary angiography: pre- operative evaluation before totally endoscopic coronary artery by- pass grafting. Radiology 2003;229:200-208
49. Falk V, Mourgues F, Adhami L, Jacobs S, Thiele H, Nitzsche S, et al. Cardio navigation: planning, simulation, and augmented reality in robotic assisted endoscopic bypass grafting. Ann Thorac Surg 2005;79:2040-2047
50. Gilard M, Cornily JC, Rioufol G, Finet G, Pennec PY, Mansourati J, et al. Noninvasive assessment of left main coronary stent paten- cy with 16-slice computed tomography. Am J Cardiol 2005;95:110- 112
51. Gaspar T, Halon DA, Lewis BS, Adawi S, Schliamser JE, Rubinshtein R, et al. Diagnosis of coronary in-stent restenosis with multidetector row spiral computed tomography. J Am Coll Cardiol 2005;46:1573-1579
52. Gilard M, Cornily JC, Pennec PY, Le Gal G, Nonent M, Mansourati J, et al. Assessment of coronary artery stents by 16 slice computed tomography. Heart 2006;92:58-61
53. Manghat NE, Morgan-Hughes GJ, Marshall AJ, Roobottom CA.
Multidetector row computed tomography: imaging congenital coronary artery anomalies in adults. Heart 2005;91:1515-1522 54. Kim SY, Seo JB, Do KH, Heo JN, Lee JS, Song JW, et al. Coronary
artery anomalies: classification and ECG-gated multi?detector row CT findings with angiographic correlation. Radiographics 2006;26:
317-334
55. Kondo C, Mori S, Endo M, Kusakabe K, Suzuki N, Hattori A, et al.
Real-time volumetric imaging of human heart without electrocar- diographic gating by 256-detector row computed tomography. J Comput Assist Tomogr 2005;29:694-498
56. Namdar M, Hany TF, Koepfli P, Siegrist PT, Burger C, Wyss CA, et al. Integrated PET/CT for the assessment of coronary artery dis- ease: a feasibility study. J Nucl Med 2005;46:930-935
57. Berman DS, Hachamovitch R, Shaw LJ, Friedman JD, Hayes SW, Thomson LE, et al. Roles of nuclear cardiology, cardiac computed tomography, and cardiac magnetic resonance: assessment of pa- tients with suspected coronary artery disease. J Nucl Med 2006;47:
74-82
58. Berman DS, Hachamovitch R, Shaw LJ, Friedman JD, Hayes SW, Thomson LE, et al. Roles of nuclear cardiology, cardiac computed tomography, and cardiac magnetic resonance: noninvasive risk stratification and a conceptual framework for the selection of non- invasive imaging tests in patients with known or suspected coro- nary artery disease. J Nucl Med 2006;47:1107-1118
J Korean Radiol Soc 2007;56:461-472
Address reprint requests to : Sang Il Choi, M.D., Department of Diagnostic Radiology, Seoul National University Bundang Hospital 300 Gumi-dong, Bundang-gu, Seongnam-si, Gyeonggi-do 463-707, Korea.
Tel. 82-31-787-7609 Fax. 82-31-787-4011 E-mail: drsic @ radiol.snu.ac.kr
Coronary CT Angiography: Focus on a New Algorithm as Diagnostic Tool in Routine Clinical Practice1
Dong Hun Kim, M.D., Sang Il Choi, M.D.2, Eun-Joo Chun, M.D.2, Sung-A Chang, M.D.3, Eeu-Keun Choi, M.D.3, Hyuk-Jae Chang, M.D.3, Dong-Ju Choi, M.D.3,
Whal Lee, M.D.4, Jae-Hyung Park, M.D.4
1Department of Radiology, Chosun University, College of Medicine
2Department of Diagnostic Radiology, Seoul National University Bundang Hospital
3Cardiovascular Center, Seoul National University Bundang Hospital
4Department of Diagnostic Radiology, Seoul National University Hospital
Various invasive and non-invasive imaging techniques have been used for the diagnosis of coronary artery disease. Despite several limitations, coronary CTA may soon emerge as the initial diagnostic modality of choice for patients with suspected coronary artery disease. However, in routine clinical practice, the role of coronary CTA is not clearly defined even though promising diagnostic accuracy has been demonstrated com- pared with that of the other non-invasive tests. Herein, we suggest a new paradigm for coronary CTA as an emerging diagnostic tool in routine clinical practice on the basis of our experience and published data.
Index words :Heart, CT
Computed tomography (CT), angiography Coronary vessels, CT