Abstract : Background : Sitagliptin, which inhibits dipeptidyl polypeptidase-4 and stimulate the secretion of insulin, is primarily used as a combination therapy with other oral hypoglycemic drugs. Sitagliptin is known to have lower incidence in hypoglycemia compared to other oral hypoglycemic drugs. However, several studies suggest that combination therapy including sitagliptin, can cause hypoglycemia. The aim of this study is to analyze the effectiveness and the frequency of hypoglycemia in Korean patients with type 2 diabetes treated with sitagliptin and sulfonylurea.
Methods : From August 2008 to April 2010, we retrospectively reviewed the electronic medical
회원학술보고
제 2형 당뇨 환자에서 Sitagliptin과 Sulfonylurea계 약물 병용 시 혈당 조절 효과와 저혈당 발현에 관한 연구
강민경
a, 정선회
a, 김향숙
a, 오정미
b, 최경희
c�서울대학교병원 약제부
a, 서울대학교 약학대학
b, 순천대학교 약학대학
cEffectiveness and Incidence of Hypoglycemia in the Combination of Sitagliptin and Sulfonylurea, in Patients with
Type 2 Diabetes Mellitus
Min Kyong Kang
a, Sun-Hoi Jung
a, Hyang Sook Kim
a, Jung Mi Oh
b, and Kyung Hee Choi
c�Department of Pharmacy, Seoul National University Hospital, 101 Daehak-ro, Jongno-gu, Seoul, 110-744, Korea
aCollege of Pharmacy, Seoul National University, 1 Gwanak-ro, Gwanak-gu, Seoul, 151-742, Korea
bCollege of Pharmacy, Sunchon National University, 255 Jungangno, Suncheon, Jeonnam, 540-950, Korea
c투고일자 2014.5.26; 심사완료일자 2014.6.16; 게재확정일자 2014.6.23
�교신저자 최경희 TEL 061-750-3763 E-mail: [email protected]
연구 배경 및 목적
당뇨는 대표적인 만성 질환 중 하나로 최근 들어 유병 율이 급격히 증가하는 추세로, 사회적으로도 중요한 의 미를 지니는 질병이다. 국민건강보험공단 자료에서 제 시하고 있는 의료비 증가 내용을 살펴보면, 2010년도 내분비, 영양 및 대사 질환에 관한 기관 부담금으로 추 산되는 금액은 약 1550억원으로 이는 2003년의 660 억원에 비해 2배 이상 증가한 것이다.
1)더구나 당뇨 진 행에 따른 합병증 발생을 고려할 때 질병에 의한 실질 적인 부담금은 상기 금액을 상회할 것으로 예상할 수 있다. 이러한 이유로 새로운 당뇨병 치료제의 등장은 사회적으로도 주목을 받고 있다. 이 중 2006년 개발된 sitagliptin은, dipeptidyl polypeptidase-4 (DPP-4) 억제제에 속하는 새로운 기전의 경구 당뇨약제로 장에 서 분비되는 인크레틴의 일종인 glucagon-like pep- tide-1(GLP-1)의 활성을 연장시켜 인슐린의 합성과 분비를 촉진시키고, 글루카곤의 분비는 감소시켜 혈당
을 조절한다. Drab S.R. 등의 연구에 따르면 이와 같 이 GLP-1 분해 효소 DPP-4를 억제하여 간접적으로 혈당 강하 효과를 나타내는 sitagliptin은 위약군과 비 교하였을 때 저혈당 위험성이 유의하게 증가하지 않으 며, 체중 증가 부작용 발현은 감소하는 장점을 가진다 는 결과가 있으며 이러한 장점 등에 따라 사용량이 증 가하고 있다.
2)Sitagliptin의 투여 시 주의할 점은 크레 아티닌 청소율이 50 mL/min 이상인 환자의 경우 체 중에 관계없이 1일 1회 복용을 추천하나, 50 mL/min 미만인 경우 용량 조절이 필요하다는 점이다.
3)Sitagliptin은 주로 metformin과 함께 투여가 이루어 지나, sulfonylurea계 약물과도 빈번하게 병용되고 있 다.
4)2007년 발표된 K. Hermansen 등의 연구에서는 glimepiride 단독 또는 glimepiride와 metformin 두 약물을 병용하는 환자에게 sitagliptin을 추가 투여하 고, 24주 후 HbA1C 값의 변화를 확인한 결과, sitagliptin을 병용하지 않은 군은 HbA1C 값이 0.28%
증가한 것에 비해 추가로 sitagliptin을 병용한 군에서 records of type 2 diabetes patients who were prescribed sulfonylurea and sitagliptin over a period of 6 months at Seoul National University Hospital. We excluded patients who had been using insulin as well as those, who had ESRD or kidney transplantation.
Results : A total of 232 Korean patients were enrolled in this study. The effectiveness in the reduction of blood glucose was statistically significant (P<0.05). In the sulfonylurea maintenance group (n=206), 10 patients experienced hypoglycemia, however two of them were not related to the medicine. In the sulfonylurea reduction group (n=26), one patient who had problems of alco- hol abuse, experienced hypoglycemia. Therefore, he recovered from hypoglycemia after quitting drinking.
Conclusions : In this study, the combination therapy of sitagliptin and sulfonylurea significantly improved glycemic control. Yet, hypoglycemia occurred in some patients after adding sitagliptin.
[Key words] Type 2 DM, Sulfonylurea, Sitagliptin, Hypoglycemia
는 HbA1C 값이 0.45% 감소했다는 결과가 보고되었으 며, sitagliptin 병용군에서 저혈당 발생 빈도가 더 높 다는 연구 결과(1.8% vs. 12.2%) 또한 보고되었다.
5)2008년도에는 혈당 조절이 잘 이루어지지 않고 있는 metformin, glimepiride, insulin 병용 투여 환자에 게 sitagliptin을 추가하였을 때 저혈당이 발생한 사례 또한 보고되었는데, 이때 환자는 sitagliptin을 중단하 였으나 이후 재투여하자 다시 저혈당이 발생하였다.
6)2010년 현재 제조사 측에서는 sitagliptin 허가 사항에 저혈당이 발생할 수 있는 인슐린 분비 촉진 약물이나 인슐린 병용 시, 병용과 동시에 기존 제제의 용량을 감 량하도록 지시하는 내용을 추가하고 병용 약물에 따른 저혈당 발생에 대해 주의해야 할 필요가 있음을 알리고 있다.
7)그러나, 이와 같은 내용에도 불구하고 국내에서는 아 직까지 sulfonylurea계 약물 전반에 걸쳐 sitagliptin 과의 병용 시 발생할 수 있는 부작용 등에 대해서는 구 체적인 연구가 이루어지지 않은 상황으로 이런 현황을 근거로 할 때, sulfonylurea계 약물과 sitagliptin 병 용 시 국내 환자에게 나타나는 영향을 분석하는 것이 필요할 것으로 보인다.
본 연구에서는 국내 환자를 대상으로 sulfonylurea 계 약물 단독 또는 sulfonylurea계 약물과 met- formin을 복용하는 환자를 대상으로 sitagliptin을 추 가하였을 때 sulfonylurea계 약물 별 혈당 조절 효과 를 각각 분석하고, 병용 시 저혈당 발현 빈도 및 sul- fonylurea계 약물 감량 여부가 저혈당 발생에 미치는 영향을 분석하고자 한다.
연구방법 1. 대상 환자
본 연구는 2008년 8월부터 2010년 4월까지의 기간 중 서울대학교병원에서 sulfonylurea계열 약제와 sitagliptin의 병용 투여를 시작한 제 2형 당뇨 환자를 대상으로 하였다. 이 때 sitagliptin 병용 기간이 6개월 이하인 환자, sitagliptin의 약동학적 특성상 감량 투여 가 요구되는 말기신부전증(end stage renal disease, ESRD) 환자와 신이식 환자는 제외하였고, 혈당에 직접
적인 영향을 주는 insulin 주사 제제 병용 환자 역시 대 상군에서 제외하였다. 또한, 의무기록 미비로 인해 효과 와 부작용 발생 여부를 확인할 수 없는 환자도 그 대상 에서 제외하였다.
그러나 sulfonylurea계 및 sitagliptin외 병용 빈도가 높은 경구 혈당 강하제인 metformin의 경우, sitagliptin 과 병용 시 저혈당 발생빈도의 증가 및 약물 동력학적인 특성에 영향을 주지 않는다는 문헌을 근거로, sulfony- lurea계 약제와의 병용 기간이 3개월 이상으로 met- formin의 효과가 안정적인 환자는 대상 환자군에 포함 하였다.
12),16)2. 자료 수집
전자 의무기록을 통해 대상군에 속하는 환자 특성에 대해 다음의 자료를 후향적으로 수집하였다.
�성별
�병용 투여 시작시의 연령
�임의 혈당 측정치 (Random glucose, mg/dL)
�Sitagliptin 시작 용량
�복용 중인 sulfonylurea계 약물의 종류와 용량
�Sitagliptin 병용 전 metformin 복용 여부
Clinical outcome 항목으로는 sitagliptin 병용 후 6 개월, 1년이 경과된 시점에서 다음의 자료를 후향적으 로 수집하였다.
�Sulfonylurea계 약물의 용량 변화
�HbA1C 변화량
�저혈당 발생 빈도
이 때 저혈당 발생의 판단 기준은 입원 환자의 경우
Whipple’ s triad criteria로 선정하였고,
8)외래 환자의
경우 의료진의 판단에 따른 의무기록상의“저혈당”기
록으로 선정하였다. Whipple’ s triad criteria에서 정
의하는 저혈당은 환자가 증상을 겪었을 때의 혈중 당
농도가 50 mg/dL 이하로, 의무기록에 피로감, 권태
감, 오심, 손떨림, 어지러움 등의 중추신경계 증상이 기
록되어 있거나 당 섭취 후 저혈당 증상이 회복되는 경
우를 의미한다.
3. 자료 분석
수집한 자료는, 먼저 병용한 sulfonylurea제를 성분 별로 분류하였고, 이후 sitagliptin 병용 전 HbA1C (>7.5%, ≤7.5%) 및 환자연령(>65세, ≤65세)으로 나 누어 각각 분석하였다.
17)각 그룹별 분석항목은 저혈당 의 발생 빈도, HbA1C 변화량, sulfonylurea계열 약물 의 감량 용량이었으며, 각 군간 혈당 조절 효과를 판정 하기 위해 student t-test를, 저혈당 발생 빈도 차이 를 판정하기 위해 Fisher’ s exact test를 사용하였고, 여기에는 모두 95% 신뢰구간을 적용하였다.
Sulfonylurea계 약물 세 군간의 혈당조절 효과는 ANOVA(one-way factorial)를 사용하여 분석하였다.
연구결과 1. 환자군 특성
연구 기간 동안 조건을 만족하는 환자는 총 232명으로 이들의 환자 정보를 수집하였다. 이 중 205명(88.4%) 의 환자는 3개월 이상 sulfonylurea계 약물 외 met- formin을 병용 투여하고 있었다. 이들 연구 대상 환자 의 평균 HbA1C는 8.23±0.85(%)였으며, 임의 혈당 측정치는 152.2±32.4(mg/dL)이었다. 환자가 복용 중 인 sulfonylurea계 약 물 은 glibenclamide, glimepiride, gliclazide 등 3가지로, 그 종류에 따라 분류했을 때 glibenclamide 복용 군이 다른 두 군 (glimepiride, gliclazide)에 비해 환자 수의 규모가 작 았으며, 각 제제당 metformin 병용 비율이 유의하게 나타나지 않았다. Sulfonylurea계 약물 별 복용 환자 의 평균 연령도 세 군간 통계적으로 유의하지 않았다.
또한 치료 전 초기 HbA1C(%)와 연령 및 임의 혈당 측 정치도 각 sulfonylurea계 약물 군간에 통계적으로 유 의한 차이가 나타나지 않았으나 sitagliptin의 용량은 gliclazide 사용 군에서의 투여 용량 차이로 인해 세 군 간 임상적인 유의성이 나타났다(p<0.05)(Table 1, Table 2).
2. Clinical Outcomes
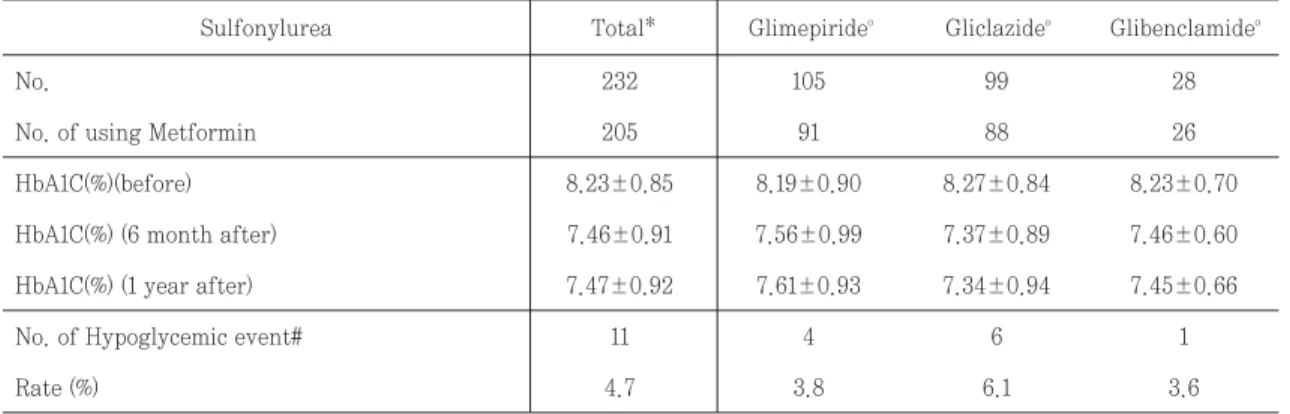
대상 군 환자의 HbA1C(%) 수치 변화를 sitagliptin 병 용 기간에 따라 분석했을 때 sitagliptin 병용 투여초기 측정값과 6개월 후 측정값(p<0.05), 병용 투여 초기 측 정값과 1년 후 측정치(p<0.05)에서 각각 통계적으로 유 의하게 감소하였다. 또한 대상 군의 6개월 후 평균 HbA1C는 7.5 % 이하로 산출되었다. 저혈당은 232명
Table 1. Baseline characteristics of patients
No* 232
No* of using Metformin 205
Age(Years) 62.3±10.2
Sex 56.0/44.0
Male 130(56%)
Female 102(44%)
HbA1C(%) 8.23±0.85
Random Glucose(mg/dL) 152.2±32.4
Sitagliptin dose 83.2±24.0
Total
* Number of patients
Table 2. Study population profile grouped by on- going sulfonylurea
No.* of using
Metformin 91 88 26 0.97
Age (Years) 62.3±10.1 62.1±10.9 63.1±8.4 0.90
Sex 0.16
Male Female
62(59%) 49(50%) 19(68%) 43(41%) 50(50%) 9(32%)
p- value Glibencla-
mide (n=28) Gliclazide
(n=99) Glimepi-
ride (n=105)
* Number of patients HbA1C
(mean%±SD) 8.19±0.90 8.27±0.85 8.23±0.70 0.81 Random
Glucose (mean, g/dL±SD)
146.6±28.1 158.4±35.8 153.7±34.1 0.14
Sitagliptin dose (mean mg±SD)
91.4±18.9 74.0±25.5 84.8±24.9 6.5x10-7
중 11명(4.7%)이 겪었는데 이들은 모두 sitagliptin 추가 후 초기 6개월 이내에 저혈당을 경험하였다(Table 3).
Sitagliptin 병용 전 HbA1C 측정값을 7.5%를 기준으 로 두 군으로 나누었을 때 각군 간의 HbA1C(%) 조절 효 과와 저혈당 발생 빈도는, sitagliptin 병용 전
HbA1C>7.5% 군에서만 HbA1C 수치 감소에서 통계적 으로 유의한 결과를 얻었다. 또한, 대상환자의 연령을 65세 기준으로 분류한 경우에는 두 군 모두 HbA1C 수 치 감소가 통계적으로 유의하게 나타났다. 그러나 초기 HbA1C(%) 수치 및 연령에 따른 저혈당 발생 빈도를 비 교한 분석에서는 유의성을 획득하지 않았다(Table 4).
Table 3. HbA1C(%) changes before vs. after sitagliptin addition in each sulfonylurea group
No. 232 105 99 28
No. of using Metformin 205 91 88 26
HbA1C(%)(before) 8.23±0.85 8.19±0.90 8.27±0.84 8.23±0.70
HbA1C(%) (6 month after) 7.46±0.91 7.56±0.99 7.37±0.89 7.46±0.60
HbA1C(%) (1 year after) 7.47±0.92 7.61±0.93 7.34±0.94 7.45±0.66
No. of Hypoglycemic event# 11 4 6 1
Rate (%) 4.7 3.8 6.1 3.6
Glimepirideo Gliclazideo Glibenclamideo Total*
Sulfonylurea
*p-value:Δbefore~6m<2.2x10-16/Δbefore~1y<2.2x10-16
op-value(Glimepiride):Δbefore~6m=2.3x10-9/Δbefore~1y=1.1x10-5
op-value(Gliclazide):Δbefore~6m<2.2x10-16/Δbefore~1y=1.1x10-15
op-value(Glibenclamide):Δbefore~6m=3.2x10-6/Δbefore~1y=0.0051
#p-value:0.82 No. number of patients
Table 4. HbA1C(%) changes before vs. after sitagliptin addition in each sub group
n 40 184 138 94
HbA1C(before) 7.15±0.32 8.47±0.74 8.22±0.84 8.25±0.87
HbA1C(6 month after) 6.92±0.61 7.57±0.93 7.51±1.01 7.39±0.74
HbA1C(1 year after) 7.01±0.62 7.58±0.94 7.54±0.98 7.39±0.83
No. of Hypoglycemic event$ 2 8 7 4
Rate (%) 5.0 4.3 5.1 4.3
HbA1C*
≤7.5 >7.5
Ageo
≤65 >65
*p-value (≤7.5) :Δbefore~6m=0.027/Δbefore~1y=0.32
*p-value (>7.5) :Δbefore~6m=<2.2x10-16/Δbefore~1y=<2.2x10-16
op-value (≤65) :Δbefore~6m=6.8x10-15/Δbefore~1y=3.1x10-11
op-value (>65) :Δbefore~6m=1.2x10-15/Δbefore~1y=3.0x10-10
$p-value o:HbA1C=0.69, Age=1.00
Sitagliptin 병용 시의 저혈당 발생 빈도를 확인하기 위해 먼저 병용 시점에서 sulfonylurea계 약물 감량 여 부를 조사하였다. 이때 전체 232명 중 5% 미만인 26명 (3.85%)만이 sitagliptin을 추가하면서 동시에 sulfony- lurea계 약물의 용량을 감량하였고 이들 중 1명에게서 저혈당이 발생하였다. 또한 sulfonylurea계 약물 용량 을 감량하지 않은 환자 206명의 경우 저혈당이 발생한 10명 중 다른 원인이 밝혀진 2명을 제외하고 8명은 이전 혈당 상승 상태 조절을 위한 sitagliptin 추가로 인해 저 혈당 발생이 유의하게 증가한 것으로 보인다(p<0.05).
환자 중 저혈당을 경험한 환자 총 11명 중 8명의 환자 가 저혈당 발생 후 sulfonylurea계 약물을 감량하는 처 방을 받았으며, 그 결과 8명 모두는 저혈당에서 회복되 었다. 나머지 3명의 환자 중 1명은 담도염으로 인해 사망 한 환자로 약제와의 관계성을 확신하기 어려웠으며, 다 른 1명의 환자는 저혈당의 원인이 itraconazole에 유발 된 식욕부진으로 진단된 경우로, itraconazole 중단을 통해 식욕 부진에서 회복하면서 저혈당에서도 회복된 사실을 확인할 수 있었다. 마지막으로 sulfonylurea계 열 약물의 초기 감량에도 불구하고 저혈당이 발생했던 1 명의 환자는 알코올 중독의 위험인자를 가지고 있던 환 자로 금주 이후 더 이상 저혈당은 발생하지 않았다.
Sitagliptin 병용을 시작하면서 sulfonylurea를 감량 한 군과 감량하지 않은 군을 대상으로 비교한 환자 기본 정보에서는 유의한 차이가 확인되지 않았다. 또한 sul- fonylurea계 약물을 감량한 군의 경우 병용 전 평균 복 용량의 44.6±13.1%를 감량하였으며, 이는 모두 상용량 이내에 포함되어 있었다(Table 5).
고찰
Sitagliptin은 그 기전상 직접적으로 insulin 분비에 관여하지 않으므로 단독 사용시 저혈당이 발생하지 않 는 제제로 알려져 왔다. 그러나 병용 요법에 따른 부작 용, 특히 insulin 분비를 촉진하는 제제와 병용 시 저혈 당이 발생한다는 보고가 이루어지면서 sulfonylurea 계 제제와 병용 시 이들의 용량을 감량할 것을 권고하 고 있다.
13),14),18)또한 가까운 일본 역시, 이와 관련한 감 량 가이드라인이 제시되고 있다.
10)그러므로 국내 환자 에 대한 실정을 파악하고 이에 대한 확인이 필요한 실 정이지만, 지금까지 sitagliptin 제제와 관련된 국내 연 구는 sitagliptin 제제 단독 사용시, 또는 metformin 과의 병용 사용에 관한 내용으로 sitagliptin과 sul- fonylurea 계열 약물 병용에 관한 연구는 부족한 상황 Table 5. HbA1C(%) changes before vs. after sitagliptin addition in each sulfonylurea group
Number of using Metformin(%) 22(84.6%) 183(88.8%) 1.00
Age(Years) 62.3±10.1 62.6±10.2 0.28
Sex(M/F%) 61.5/38.5 55.3/44.7 0.70
HbA1C(%) 8.10±0.62 8.25±0.88 0.41
Random Glucose(mg/dL) 150.5±32.1 152.5±32.6 0.80
Sulfonylurea Dose Reduction % 44.6±13.1 0
Sitagliptin dose 92.3±18.4 82.0±24.4 0.014
HbA1C(%) 6month delta -1.03±0.86 -0.74±0.89 0.13
HbA1C(%) 1year delta -0.86±0.74 -0.71±0.84 0.50
Total number of hypoglycemic event 1(0*) 10(8*) -
Decreased (N=26)
Undecreased
(N=206) p-value
* The number of hypoglycemia due to medication