이식된 자가골의 종류와 형태에 따른 임플란트 변연골 흡수량에 관한 후향적 연구
김태이
1·김예미
2·김지연
2·김명래
1,2·김선종
1,21
이화여자대학교 임상치의학대학원 임플란트학과,
2
이화여자대학교 의학전문대학원 치과학교실 구강악안면외과
Abstract(J Korean Assoc Oral Maxillofac Surg 2011;37:483-9)
The retrospective study of marginal bone loss around dental implants according to different autogenous bone grafts
Tae-Yi Kim
1, Ye-Mi Kim
2, Ji-Youn Kim
2, Myung-Rae Kim
1,2, Sun-Jong Kim
1,21
Department of Implantology, Graduate School of Clinical Dentistry, Ewha Womans University,
2
Department of Oral and Maxillofacial Surgery, School of Medicine, Ewha Womans University, Seoul, Korea
Introduction: This study examined the cumulative resorption of implants placed in a severely atrophic mandible and analyzed the radiologic bone resorption in the marginal bone, after an autogenous bone graft including both block and particulates that had been harvested from the ramus and iliac crest.
Materials and Methods: A retrospective study was performed on patients who had bone grafts for augmentation followed by implant installation in the mandible area from 2003 to 2008. Twelve patients (6 men and 6 women) who received 34 implants in the augmented sites were evaluated.
Cumulative radiologic resorption around the implants was measured immediately, 3 months, 6 months and 12 months after implant installation surgery.
Results: The installed implant in grafted bone showed 0.84 mm marginal bone resorption after 3 months and 50% total cumulative resorption after 1 year. The mean marginal bone resorption around the implant installed in the grafted bone was 0.44 mm after 3 months, 0.52 mm after 1 year, after which it stabilized. The implant survival rate was 97% (failed implant was 1/34). Marginal bone resorption of the installed implant in the autogenous onlay block bone grafts was 0.98 mm after 3 months, which was significantly higher than that of a particulated bone graft (0.74 mm) (P<0.05).
Conclusion: An autogenous graft including block type and particulate type is a predictable procedure for the use of dental implants in a severely atrophic mandible. Implant placement in augmented areas show a relatively high survival and minimal bone loss, as revealed by a radiologic evaluation.
Key words: Dental implants, Bone graft, Bone resorption
[paper submitted 2011. 7. 11 / revised 2011. 8. 26 / accepted 2011. 10. 12]
임플란트식립에제한을받기때문에치조골증대술등의 고급임플란트 술식이요구된다1,2
.
치조골증대술은 골이 식결손부가크지 않은경우동종골이나이종골재료만으 로이식을하는경우도있으나,
자가골은골형성능,
골전도 능,
골유도능등골이식재가갖춰야할기본적인조건들을 모두만족시키며면역거부반응을일으키지않고생체적합 력이높아빠른치유를보여주는등의장점을가지고있기 때문에 골이식재의최선의기준으로받아들여진다.
그러 나,
골흡수속도가빠르기때문에임플란트를유지하기위 한신생골의양이부족할수도있으며부위에따라채취량 이제한적일수있고,
공여부에이차적인수술부위를만들 어야하는단점이있다3.
이식을 위한 자가골편은 구강 내와구강 외에서 채취 할 수 있다4-7
.
구강외에서 가능한채취부위로는두개골I. 서 론
임플란트의장기적이고안정적인예후를 위해서는충분 한골량과양호한골질의확보가필수적이다
.
중등도이상 의치주염,
종양절제,
구강악안면영역의외상등에의한치 아의발거,
또는 조기치아 발거후장기간무치악상태의 유지등의원인으로치조골이 과도하게 위축된경우에는 김 선 종158-050 서울시 양천구 목동 911-1
이화여자대학교 의학전문대학원 구강악안면외과학교실 Sun-Jong Kim
Department of Oral and Maxillofacial Surgery, School of Medicine, Ewha Womans University 911-1, Mok-dong, Yangcheon-gu, Seoul 158-050, Korea TEL: +82-2-2650-5041 FAX: +82-2-2650-5764 E-mail: [email protected]
학교의학전문대학원부속목동병원치과진료부에내원하 여임플란트식립을목적으로하악 구치부에자가골이식 술을시행받은환자들중에서
,
보철치료가완료되고3
개월 이상 추적조사가가능했던12
명(
남자6
명,
여자6
명)
을대 상으로하였다.
환자들의구강내16
부위에서식립된34
개 의임플란트를대상으로하였으며이중1
개의임플란트가 보철치료전제거되어,
보철치료까지추적조사된임플란 트는33
개였다.
골이식직후와임플란트식립직후및보철 치료후에최소한2
장이상의추적방사선사진이있는환 자를대상으로하였다.
기준측정길이가되는골이식시점 외에추가골이식된부위는연구대상에서제외하였으며,
골이식술후감염및판막열개등이발생하여1
주이상치 료목적의부가적항생제투약과외과적소파술등의추가 술식을시행한부위도연구대상에서제외하였다.
관찰기간은보철수복후평균
32±28
개월이었고평균나이는56±
11
세였다.(Table 1)
임플란트의식립시기에따라분류한결과골이식과임플란트의동시식립한임플란트
15
개,
골이 식술후6
개월지난후에식립한임플란트9
개, 1
년후식립 한임플란트9
개, 2
년내에식립되었던임플란트1
개로분 류되었다.(Table 2)
1)
사용된자가골공여부와골이식재의형태자가골의공여부위에따라구강내 공여부위인 하악지 에서 채취하여 골이식한 부위에 식립한 임플란트
19
개 와구강 외공여부위인장골에서채취하여골이식한부위 에 식립한 임플란트15
개,
두가지로 분류할 수 있다.
또 한 골이식재의 형태에 따라 블록골형태로 온레이 골이 식을 시행한부위에 식립한임플란트14
개와 입자 형태(calvarium),
경골(tibia),
장골(iliac crest),
늑골(rib)
등이있다
.
이중장골이악골재건에가장자주사용되나술후에 일시적인보행의불편,
입원,
술 후합병증등으로사용에 제한이있을수있으며,
치과임플란트와동반하는골이식 술식의경우많은양의골량을필요로하는경우는많지않 기때문에구강내에서채취하는경우가더욱일반적이다.
하지만,
장골은 다량의피질골및해면골이식이가능하기 때문에,
골이식을필요로하는위축된치조골의양과범위 가클경우장골이식은매우유용한공여부가된다8-11.
구강 내공여부위는상악결절부,
상악동전벽,
관골,
하악상행 지,
하악골체부,
하악골오훼돌기,
하악및상악골융기등 이다.
공여부와수혜부가인접해있어서외과적접근이용 이하고수술시간 및마취시간이단축되며 피부에흉터를 남기지않고구강외채취에비해환자가느끼는불편감은 훨씬적다는장점이있다.
하지만,
구강외공여부위에비 해채취량이제한적이라는단점이있다12,13.
이러한이식골 이수혜부에잘유지,
안착할수있도록하기위해서는흡수 성및비흡수성차단막,
티타늄메쉬등이입자형골이식등 에사용될수있으며,
블록형으로골이식을하는경우에는 고정나사나혹은임플란트로직접수혜부에고정시키는방법들이시행될수있다5,14-16
.
Papageorge
등17은자가골이식으로재건된9
명의하악골결손부환자에서결손부재건에사용된자가골이임플란트 보철물의제작을위해성공적으로사용될수있다고보고
하였으며
, Keller
등18은자가골을이식한31
명의재건환자들을
12
년간조사하여이식골에식립한임프란트가95.5%
생존한것과보철물이
100%
성공한것을보고하였다.
본연구의목적은하악구치부에자가골이식을시행하 고
,
이식골의치유후에식립한임플란트의파노라마방사 선사진을추적조사하여임플란트변연골의흡수량을측 정함으로써자가골의종류와형태에따른임플란트의안정 성과변연골의흡수량을비교분석하고자하였다.
II. 연구 대상 및 방법
1. 연구 대상
본연구는
2003
년1
월부터2008
년12
월까지이화여자대Table 1. Patients’ description
Description Period/number
Post-operative follow-up (mon) Number of patients
Age of patients (yr) Number of target areas Number of implants
32±28 (4-60) 12 (male: 6, female: 6)
56±11 16 34
Tae-Yi Kim et al: The retrospective study of marginal bone loss around dental implants according to different autogenous bone grafts. J Korean Assoc Oral Maxillofac Surg 2011
Table 2. Number of implants placed after autogenous bone graft according to time of implant installation
Period between graft and installation (mon) Number 0 (immediate installation)
Up to 3 Up to 6 Up to 12 Up to 24
15 0 9 9 1
Tae-Yi Kim et al: The retrospective study of marginal bone loss around dental implants according to different autogenous bone grafts. J Korean Assoc Oral Maxillofac Surg 2011
Table 3. Number of implants according to donors and graft methods
Ramus Iliac Total
Block Particulated Total
6 13 19
8 7 15
14 20 34 Tae-Yi Kim et al: The retrospective study of marginal bone loss around dental implants according to different autogenous bone grafts. J Korean Assoc Oral Maxillofac Surg 2011
사용하여견고하게밀착고정하였다
.
증강된이식골을긴장없이봉합하기위해전기소작기
와 수술도의사면을이용하여골막의 감장절개
(releasing
incision)
를 시행하였다.
봉합은 단속봉합(interrupted)
및 수직누상봉합(vertical mattress),
수평누상봉합(horizontal mattress),
그리고남은자연치에고정봉합(tie suture)
을시 행하여창상을유지시켰다.
가철성의치는술후2
주간사 용하지않도록권유하였고봉합사는7-10
일후에제거하였 다.
임플란트는이식술후최소5
개월,
최대11
개월에식립 하였다.
(2)
자가하악지온레이골이식술Midazolam (Bukwang Pharm., Seoul, Korea)
및1 : 8
만epinephrine
이포함된2% lidocaine (Yuhan Co., Seoul,
Korea)
을 이용한진정국소마취 하에시행되었다.
공여부절개는견치원심에서각화점막내에형성하고
,
전층판막 을피판 전방부에서거상하고이공을확인한후후방부를 거상하였다.
생리적식염수주수하에micro-oscillating saw (Stryker Co., Portage, MI, USA)
를이용하여블록골을절단 하였고,
골절도를이용하여분리시켰다.
자가장골을이용한블록골 이식술과동일하게수혜부는 여러부위의피질골을천공하여출혈을유도하여이식골과 의 결합을증진시키도록하였다
.
또한2
개 이상의골고정 나사로블록골이식재를고정하였다.
골절삭용버(burr)
로 날카로운 면을가다듬고수여부와 이식골편과의빈 간극에자가골을
chip bone
으로만들어서Bio-Oss
등과혼합하여채워넣었다
.
일차봉합을위하여감장절개가협측판막 을따라수행되었다.
임플란트는공여부가하악지이식술 인경우이식후최소4.5
개월,
최대14
개월후에식립하였 으며,
고정용골나사를한꺼번에제거하지않고앞에서부 로자가골을만들어이종골(Bio-Oss, Geistlich, Wolhusen,
Switzerland)
과1 : 1
로혼합하여골유도재생술(guided bone
regeneration, GBR)
을시행한부위에식립한20
개두가지로분류되었다
.(Table 3)
2)
식립된임플란트종류식립된임플란트종류는 표면처리된나사모양의 완전
매립형
(submerge)
구조의 골 유착형 골내 임플란트로서Replace system (Nobel Biocare AB, Göteborg, Sweden) 12
개, USII system (Osstem, Seoul, Korea) 8
개, MKⅢ system (Nobel Biocare AB) 14
개를각각식립하였다.(Table 4)
3)
골이식수술방법(1)
자가장골온레이골이식술전신마취하에서장골능접근법으로자가장골편을절취 하였다
.
또한수혜부의여러곳에피질골을천공하여혈행 이좋도록하였다.
채취한자가골편의예리한모서리를제 거하고수용부와최대한접촉할수있도록형태를조정하여수혜부에밀착한후지름
1.2 mm,
길이8-12 mm
의티타늄골고정나사
(Jeil Medical Co., Seoul, Korea)
를2
개이상Table 4. Number of implant systems used in this study
Implant system Number of
implants Internal
connection External connection Total
Replace (Nobel Biocare AB, Sweden) USII (Osstem, Korea)
MKIII (Nobel Biocare AB, Sweden)
12 8 14 34 Tae-Yi Kim et al: The retrospective study of marginal bone loss around dental implants according to different autogenous bone grafts. J Korean Assoc Oral Maxillofac Surg 2011
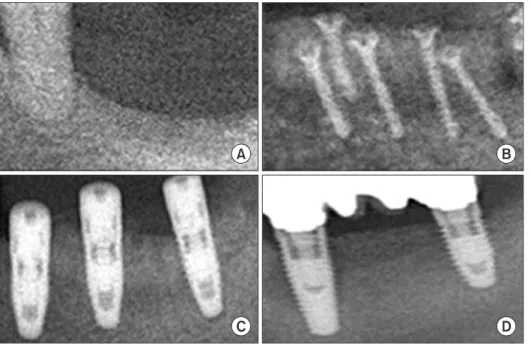
Fig. 1. Autogenous block bone graft, implant installation and functional loading. These figures were collected from different patients who underwent ramal bone graft and implant installation surgery. A. Pre-operative radiography. B.
Immediate post-operative radio graphy after autogenous block bone graft operation. C. Immediate post-opera- tive radio graphy after implant fixtures installation operation. D. Follow-up radiography after functional loading.
Tae-Yi Kim et al: The retrospective study of marginal bone loss around dental implants according to different autogenous bone grafts. J Korean Assoc Oral Maxillofac Surg 2011
터하나씩고정용나사를제거하면서임플란트를식립하였 다
.(Fig. 1)
(3)
자가입자골을이용한골증강술(GBR with particulated autogenous bone)
장골혹은 하악지로부터 자가골을 채취하여 입자형태 로분쇄한후
Bio-Oss
와1 : 1
로혼합하였다.
외형의유지를위해티타늄메쉬
,
비흡수성 차단막(Gore-Tex, WL Gore,
Flagstaff, AZ, USA),
또는흡수성차단막(Biogide, Geistlich,
Wolhusen, Switzerland)
을사용하여이식골의외형유지와골증대를유도하였다
.(Figs. 2, 3) 2. 연구 방법
자가골이식술후치유기간을거친이식골에임플란트를 지연식립하였거나혼합형골이식과동시에식립한임플란 트에서식립 직후의파노라마방사선사진과보철치료직
후를포함한추적기간동안의방사선사진에서
Myriad 8.0
(Informative Graphics Co., Scottsdale, AZ, USA)
계측시스템
(2D/3D viewer)
을 이용하여기준점이되는임플란트Fig. 2. Simultaneous implant installation with autogenous particulated bone and xenogenic bone graft. These figures were collected from different patients who underwent particulated autogenous bone and xenogenic bone graft and implant installation surgery. A. Pre-operative radiography. These previous implants were removed at bone graft surgery because of those mobility and pain. B. Immediate post- operative radiography after mixed particulated bone graft and implant installation. C. Follow-up post-operative radiography after functional loading.
Tae-Yi Kim et al: The retrospective study of marginal bone loss around dental implants according to different autogenous bone grafts. J Korean Assoc Oral Maxillofac Surg 2011
Fig. 3. Delayed implant installation after guided bone regeneration technique with autogenous particulated bone. A. Immediate post- operative radiography after autogenous particulated bone graft. B. Immediate post-operative radiography after 7-month delayed implant installation. C. Follow-up radiography after implant functional loading.
Tae-Yi Kim et al: The retrospective study of marginal bone loss around dental implants according to different autogenous bone grafts. J Korean Assoc Oral Maxillofac Surg 2011
Fig. 4. Formula for calculation of bone level and height. Average real length was calculated from (A+B/2 ×magnificent rate).
Tae-Yi Kim et al: The retrospective study of marginal bone loss around dental implants according to different autogenous bone grafts. J Korean Assoc Oral Maxillofac Surg 2011
다
.(Table 5, Fig. 5)
2. 공여부와 이식골 형태에 따른 누적 흡수량
공여부에따라변연골흡수량을비교한결과하악지로부 터이식된골에식립된임플란트변연골초기
3
개월의평균 흡수량이0.9 mm
였고장골은0.48 mm
이었다.
이중,
하악 지에서블록골형태로채취되어이식한부위에식립된임 플란트1
예에서과도한골흡수의결과를관찰할수있었다.
공여부에따른흡수 정도는하악지로부터의 이식시에더 많이높았으나통계적인유의성은없었다(P>0.05).(Table 6)
골형태에따른골흡수량은입자형골에서3
개월의평균흡수량이
0.74 mm,
블록골형태에서0.98 mm
로입자형골이블록골형태골보다약간적은골흡수를보였으며통계적 유의성이있었다
( P<0.05). 6
개월및1
년후의누적평균흡 수량에서도같은경향을보여주었으나통계적유의성은없 었다(P>0.05).(Table 7)
IV. 고 찰
골이식에어떤종류의 이식골을사용할 것인지는필요 한이식골의양과 형태에절대적으로달려있으며많은양 의이식이필요한부위에서는골재생능력이뛰어난자가 골이식이훨씬유리하다
.
자가골은더빠른골치유,
형성 과개조및높은적합성을가지고있어서생활골로의변환 이빠르고,
용도에따라충분한입자의크기를다양한형태 로채취할수있는장점이있다. Dragoo
와Sullivan
19은자가 골이 치조골결손부에서가장재생 능력이높은 이식재라 고보고하였으며, Marx
등20은자가골이신생혈관의증식,
살아있는골생성세포의함유,
성장인자방출등의이점을 가지고있어골이식재중골재생부분에있어선호되는재 의길이를측정하고알고있는실제임플란트길이와의보정계산을한뒤에대상임플란트의변연골을근
,
원심면에 서2
회측정하고평균치를구하고보정상수에의해변연골 의흡수량변화를실측치로표시하였다.(Fig. 4)
분석결과 를토대로식립한전체임플란트의식립후변연골의변화 를각각3
개월, 6
개월, 1
년동안의누적골흡수량(cumulated
bone resorption)
으로 비교하였고이식골의공여부에따른흡수량의비교와이식재의형태에따른흡수량을비교하였다
.
각군의흡수량의차이의통계적유의성을검정하기위 해SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA)
을사용하 여t-test
를시행하였다. P
값이0.05
미만일경우통계적으로 유의하다고판단하였다.
III. 결 과
1. 변연골의 누적 흡수량
측정된전체임플란트의변연골흡수는식립후
3
개월에 누적평균이0.84 mm
였으며6
개월에1.28 mm, 1
년동안에1.80 mm
였다.
각구간별흡수량의변화는처음3
개월에서가장높았고점차로흡수율이 감소하는 경향을보여주었 Table 5. Cumulative marginal bone resorption after implant placement in/with the grafted bone
Period after implantation (mon) Resorption (mm) 3
6 12
0.84 1.28 1.80
Tae-Yi Kim et al: The retrospective study of marginal bone loss around dental implants according to different autogenous bone grafts. J Korean Assoc Oral Maxillofac Surg 2011
Table 6. Cumulative resorption according to donor site (mm)
3 mon 6 mon 12 mon
Ramus
Iliac 0.91
0.48 1.48
0.78 2.04
1.28 Tae-Yi Kim et al: The retrospective study of marginal bone loss around dental implants according to different autogenous bone grafts. J Korean Assoc Oral Maxillofac Surg 2011
Table 7. Cumulative resorption according to type of the grafted bone (mm)
3 mon1 6 mon 12 mon
Block bone Particulated bone
0.98 0.74
1.37 1.20
1.91 1.67
1statistically significant at 3 months (P<0.05).
Tae-Yi Kim et al: The retrospective study of marginal bone loss around dental implants according to different autogenous bone grafts. J Korean Assoc Oral Maxillofac Surg 2011
Fig. 5. Cumulative marginal bone resorption after implant placement in/with the grafted bone.
Tae-Yi Kim et al: The retrospective study of marginal bone loss around dental implants according to different autogenous bone grafts. J Korean Assoc Oral Maxillofac Surg 2011
하였다
.
또한Wallace
와Froum
25의연구에서도즉시식립법과지연식립법의생존율은각각
89.7%, 89.6%
로유의한차이는없다고보고하였다
.
본연구는블록골형태로온레이자가골이식을시행한 부위에임플란트를 식립하거나혹은입자형태의 자가골
과
Bio-Oss
를 섞어서 혼합골형태로 골재생술을시행한뒤
,
동시혹은지연식립과같은임플란트식립시기의분류 없이변연골변화만을연구하였다.
이연구에서도기존연 구결과와같이블록골이식술이입자형골이식술에비해 더높은변연골흡수를보임을확인할수있었으며,
이는통 계적으로도유의한결과를보였다.
그리고통계적으로유 의하지는않았지만,
기존연구들의결과와다르게공여부 가하악지인경우에서장골이식부보다높은 변연골흡수 를보였다.
이는하악지에서블록골형태로채취하여골이 식을시행한1
예에서상대적으로많은양의임플란트변연 골흡수를보였기때문으로생각된다.
공여부의종류뿐만 아니라,
골이식의방법또한변연골흡수에많은영향을미 친다는것을확인할수있었다.
또한이식골의종류및형태 외에도,
특정환자의구강내골결손상태및구강위생상 태,
그리고전신적인상태및시술자의술기의존도가결과 에영향을끼칠수도 있었을것으로생각된다.
향후좀더 많은연구대상을통한전향적연구가필요하리라생각된다.
V. 결 론
본연구는
2003
년1
월부터2008
년12
월까지이화여자대 학교의학전문대학원부속목동병원치과진료부에내원하 여하악구치부에온레이골,
분쇄골등으로자가골편골이 식을하고임플란트를식립한환자들중,
식립직후와보철 후파노라마방사선사진을포함하는추적조사된2
회이상 의방사선사진평가가가능한환자12
명의16
부위에식립 된34
개의임플란트를대상으로임플란트변연골흡수량을 측정하여다음과같은결과를얻었다.
1.
이식골에식립한임플란트는식립초기에이식골의공 여부나골의형태에관계없이변연골의흡수가초기3
개월에0.84 mm
로1
년누적흡수량의50%
를보였다. 2. 3
개월 후부터는골흡수량이6
개월까지0.44 mm, 1
년까지
0.52 mm
만큼더흡수된후안정화되었으며임플란트생존율은총
34
개중1
개가실패하여97%
였다.
3.
온레이골형태로 이식술을시행한 이식골에식립된임플란트의식립후초기
3
개월변연골흡수량은0.98
mm
를보였고분쇄골0.74 mm
보다 유의성있게높았다
( P<0.05).
References
1. Brånemark PI, Lindström J, Hallén O, Breine U, Jeppson PH, 료라고보고하였다
.
자가골의 공여부에 따른 골흡수량의 정도에 대해서
Proussaefs
와Lozada
21는하악지와같은막내막성골이식재를사용하여블록골형태의자가골을이식했을때
6
개월후 방사선사진에서평균값약1 mm
의흡수,
즉증가된길이의17%
의흡수를보인다고발표하였다. Jeon
등22또한자가 골이식공여부에따른수직적치조능증강술후발생하는 골흡수량에관한연구를시행하였다.
모든이식된자가골 은블록골형태로채취되어수혜부에1
개이상의금속나사 로고정하였다.
이식후1
일과술후8
개월의치근단방사선 사진계측에서,
구강내의골을이식한증례들에서는평균0.93 mm (3.71 mm
에서2.82 mm)
의흡수를보였고,
장골이 식한증례들에서는0.95 mm (5.91 mm
에서4.96 mm)
의흡 수를보였음을확인하고구강내의골을 이식재로사용하 는것이이식재의흡수가작아치료의예측가능성이높다 고언급하였다.
자가골의이식형태및방법에따라서도골흡수량및임 플란트의성공률이 달라질 수 있다
.
자가골을 이용한 온 레이골이식술은 예측성이떨어진다는 단점이있다.
자가 골온레이골이식이시행된부위에식립된임프란트의평 균생존율과성공률은정상적인골조직에식립된것에비해 낮은양상을 보인다고알려져 있다
. 2007
년, Aghaloo
와
Moy
23는 기존발표된 다수의문헌들을 체계적으로검 토및분류하여,
치조골이식형태및방법에따라임플란트 의생존율을비교하였다.
이논문에서입자형골이식을통한골재생술
(GBR)
후식립한임플란트는95.5%
의생존율을보였으며
,
블록골을이용한온레이및베니어골이식술(onlay/veneer grafting)
후식립한임플란트는90.4%
의생존 율을보였다고보고하였다.
하지만, GBR
에대한연구논문 들외의다른연구들에서는장기간의추적기간이없고,
모 든논문이각기다른수혜부조건과증례수를다루었기때 문에표준화된연구는상당히드물다는한계점에대해서도 언급하였다.
종류및형태뿐만아니라골이식을시행한부위에임플 란트를식립하는시기또한임플란트의생존율과성공률에 영향을미칠수있는요소중하나이다
.
임플란트는통상이 식재가치유된다음에이차적으로식립하게되지만,
골편 이식과함께 임플란트를즉시식립하여이식골편을고정 하는술식이임상에적용되는경우도있다.
골이식과동시 에임프란트를식립하는경우는지연식립에비해자가골의 흡수를약간방지할수있지만치조정골의흡수및나사선 노출위험성은피할수없다.
특히창상이벌어지면골이식 재의상당량이소실되고임플란트가실패할위험성이매우 높아질수있다.
이에대한Jensen
과Sindet-Pedersen
24의연 구에의하면,
자가골만을이식하여즉시식립법과지연식 립법으로식립된임플란트의장기간(5
년)
의성공률은각각85.5%
와83.9%
였으며,
통계적으로유의한차이는없다고Surg Oral Med Oral Pathol 1979;47:17-24.
15. Doblin JM, Salkin LM, Mellado JR, Freedman AL, Stein MD.
A histologic evaluation of localized ridge augmentation utilizing DFDBA in combination with e-PTFE membranes and stainless steel bone pins in humans. Int J Periodontics Restorative Dent 1996;16:120-9.
16. Misch CM, Misch CE, Resnik RR, Ismail YH. Reconstruction of maxillary alveolar defects with mandibular symphysis grafts for dental implants: a preliminary procedural report. Int J Oral Maxillofac Implants 1992;7:360-6.
17. Papageorge MB, Karabetou SM, Norris LH. Rehabilitation of patients with reconstructed mandibles using osseointegrated implants: clinical report. Int J Oral Maxillofac Implants 1999;14:
118-26.
18. Keller EE, Tolman D, Eckert S. Endosseous implant and auto- genous bone graft reconstruction of mandibular discontinuity: a 12-year longitudinal study of 31 patients. Int J Oral Maxillofac Implants 1998;13:767-80.
19. Dragoo MR, Sullivan HC. A clinical and histological evaluation of autogenous iliac bone grafts in humans. I. Wound healing 2 to 8 months. J Periodontol 1973;44:599-613.
20. Marx RE, Carlson ER, Eichstaedt RM, Schimmele SR, Strauss JE, Georgeff KR. Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;85:638-46.
21. Proussaefs P, Lozada J. The use of intraorally harvested autogenous block grafts for vertical alveolar ridge augmentation: a human study. Int J Periodontics Restorative Dent 2005;25:351-63.
22. Jeon HR, Kim JW, Kwon HB, Lee DH, Hong JR, Kim CS. The study on the bone resorption rate after vertical alveolar ridge augmentation. J Korean Assoc Oral Maxillofac Surg 2006;32:230- 4.
23. Aghaloo TL, Moy PK. Which hard tissue augmentation techniques are the most successful in furnishing bony support for implant placement? Int J Oral Maxillofac Implants 2007;22(Suppl):49-70.
24. Jensen J, Sindet-Pedersen S. Autogenous mandibular bone grafts and osseointegrated implants for reconstruction of the severely atrophied maxilla: a preliminary report. J Oral Maxillofac Surg 1991;49:1277-87.
25. Wallace SS, Froum SJ. Effect of maxillary sinus augmentation on the survival of endosseous dental implants. A systematic review.
Ann Periodontol 2003;8:328-43.
Ohman A. Reconstruction of the defective mandible. Scand J Plast Reconstr Surg 1975;9:116-28.
2. Block MS, Degen M. Horizontal ridge augmentation using human mineralized particulate bone: Preliminary results. J Oral Maxillofac Surg 2004;62(9 Suppl 2):67-72.
3. Enneking WF, Eady JL, Burchardt H. Autogenous cortical bone grafts in the reconstruction of segmental skeletal defects. J Bone Joint Surg Am 1980;62:1039-58.
4. Shirota T, Ohno K, Motohashi M, Michi K. Histologic and micro- radiologic comparison of block and particulate cancellous bone and marrow grafts in reconstructed mandibles being considered for dental implant placement. J Oral Maxillofac Surg 1996;54:15-20.
5. Buser D, Dula K, Hirt HP, Schenk RK. Lateral ridge augmentation using autografts and barrier membranes: a clinical study with 40 partially edentulous patients. J Oral Maxillofac Surg 1996;54:420- 32.
6. Triplett RG, Schow SR. Autologous bone grafts and endosseous implants: complementary techniques. J Oral Maxillofac Surg 1996;54:486-94.
7. Raghoebar GM, Batenburg RH, Vissink A, Reintsema H. Augmen- tation of localized defects of the anterior maxillary ridge with autogenous bone before insertion of implants. J Oral Maxillofac Surg 1996;54:1180-5.
8. Harsha BC, Turvey TA, Powers SK. Use of autogenous cranial bone grafts in maxillofacial surgery: a preliminary report. J Oral Maxillofac Surg1986;44:11-5.
9. Keller EE, Van Roekel NB, Desjardins RP, Tolman DE. Pro- sthetic-surgical reconstruction of the severely resorbed maxilla with iliac bone grafting and tissue-integrated prostheses. Int J Oral Maxillofac Implants 1987;2:155-65.
10. Listrom RD, Symington JM. Osseointegrated dental mplants in conjunction with bone grafts. Int J Oral Maxillofac Surg 1988;17:
116-8.
11. Schwartz-Arad D, Dori S. Intraoral autogenous onlay block bone grafting for implant dentistry. Refuat Hapeh Vehashinayim 2002;
19:35-9, 77.
12. Smith JD, Abramson M. Membranous vs endochondrial bone autografts. Arch Otolaryngol 1974;99:203-5.
13. Kusiak JF, Zins JE, Whitaker LA. The early revascularization of membranous bone. Plast Reconstr Surg 1985;76:510-6.
14. Marciani RD, Gonty AA, Synhorst JB 3rd, Page LR. Cancellous bone marrow grafts in irradiated dog and monkey mandibles. Oral