INTRODUCTION
The incidence of bloodstream infections with fungi (espe- cially Candida species) has increased substantially during recent decades (1). One study revealed that the incidence of candidemia increased from 1.25 episodes per 10,000 patient days per year in 1999 to 3.06 episodes per 10,000 patient days per year in 2003 (2). In the United States, Candida spe- cies are the fourth highest cause of nosocomial bloodstream infection (3). Moreover, the overall mortality of patients with a blood culture positive for Candida species ranges from 31%
to 81% (4-11).
Although antifungal agents have recently been developed and are widely used, the incidence of candidemia and its asso- ciated mortality are increasing, especially in patients with severe underlying diseases (12). This trend is associated with an increase in the number of patients who receive immuno- suppressive agents after antineoplastic or antirejection chemo- therapy (13, 14). The known risk factors for candidemia are
immunosuppression, neutropenia, hemodialysis, long-term use of a central venous catheter, previous broad-spectrum anti- biotic use, and Candida colonization (1, 13). As these risk factors are common among intensive-care unit (ICU) pati- ents, ICUs are high-risk environments for candidemia.
There are few recent studies on the epidemiology of can- didemia in medical ICUs (MICUs). Therefore, we undertook a case-control study of MICU patients to evaluate their clin- ical characteristics, including the incidence of candidemia, the predominant infectious organisms present, mortality, and risk factors for candidemia in an MICU.
MATERIALS AND METHODS Study design and patients
We performed a retrospective 1:3 matched case-control study. The study was conducted at the Seoul National Univer-
671
Seon-Sook Han1, Jae-Joon Yim2, Chul-Gyu Yoo2, Young Whan Kim2, Sung Koo Han2, Young-Soo Shim2, and Sang-Min Lee2
Department of Internal Medicine1, Kangwon National University School of Medicine, Chuncheon: Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine and Lung Institute2, Seoul National University College of Medicine, Seoul, Korea
Address for Correspondence Sang-Min Lee, M.D.
Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul National University Hospital, 101 Daehang-no, Jongno-gu, Seoul 110-744, Korea.
Tel : +82.2-2072-0833, Fax : +82.2-762-9662 E-mail : [email protected]
Clinical Characteristics and Risk Factors for Nosocomial Candidemia in Medical Intensive Care Units: Experience in a Single Hospital in Korea for 6.6 Years
The aim of this study was to determine candidemia incidence among patients in a medical intensive-care unit (MICU) and the associated mortality rate and to identify risk factors associated with candidemia. We retrospectively performed a 1:3 matched case-control study of MICU patients with candidemia. Controls were matched for sex, age, and Acute Physiology and Chronic Health Evaluation (APACHE) II score.
Candidemia incidence was 9.1 per 1,000 admissions. The most common pathogen was Candida albicans. Crude mortality was 96% among candidemia patients and 52% among controls (P<0.001). Mortality differed significantly between the groups according to Kaplan-Meier survival analysis (P=0.024). Multivariate analysis identi- fied the following independent risk factors for candidemia: central venous catheter- ization (odds ratio [OR] = 3.2, 95% confidence interval [CI]=1.2-9.0), previous steroid therapy (OR=4.7, 95% CI=1.8-12.1), blood transfusion during the same admission period (OR=6.3, 95% CI=2.4-16.7), and hepatic failure upon MICU admission (OR=6.9, 95% CI=1.7-28.4). In conclusion, we identify an additional independent risk factor for candidemia, the presence of hepatic failure on MICU admission. Therefore, increased awareness of risk factors, including hepatic failure, is necessary for the man- agement of candidemia.
Key Words : Fungemia; Candidiasis; Intensive-Care Units; Mortality; Risk Factors
Received : 21 April 2009 Accepted : 28 September 2009
ⓒ 2010 The Korean Academy of Medical Sciences.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
sity Hospital, a tertiary care center in Korea. Seoul National University Hospital has 5 ICUs: a medical ICU, a surgical ICU (for patients who underwent abdominal and orthopedic surgery), an emergency ICU (for patients who presented at the emergency room), a pediatric ICU (for patients <15 yr old), and a cardio-pulmonary ICU (for patients who underwent tho- racic surgery). We studied patients who were admitted to the MICU. The MICU has 22 beds and admits medical and neu- rological patients. All patients in the MICU were ≥15 yr old. The duration of the study was 6 yr and 7 months (1 Jan- uary 2000 to 31 July 2006).
Definitions
Nosocomial candidemia was defined as one or more blood cultures positive for Candida species at least 48 hr after admis- sion. Blood cultures were tested routinely if a patient’s tem- perature was greater than 38℃. The onset of candidemia was defined as the date on which the first positive blood culture was detected. In-hospital mortality was defined as death during the same period of hospitalization.
Hemodynamic instability was defined as systolic blood pressure (BP) <90 mmHg, diastolic BP <60 mmHg, mean arterial BP <70 mmHg, or administration of a vasopressor on admission to the ICU. Patients were considered as having neutropenia if their absolute neutrophil count was <500 cells/
mm3on admission to the ICU. Acute renal failure was defined as a 0.5 mg/dL increase in serum creatinine level on admission to the ICU. Hepatic failure was defined as aspartate amino- transferase (AST) level >200 IU/L, alanine aminotransferase (ALT) level >200 IU/L, albumin level <3.0 g/dL, and pro- thrombin INR >2.0 on admission to the ICU. Central venous catheters (including internal jugular venous catheters, Hick- man catheters, Swan-Ganz catheters, or femoral catheters), nasogastric tubes, and Foley catheters were considered risk factors for candidemia if they were used for more than 3 days before the onset of candidemia. Previous total parenteral nutri- tion (TPN), transfusion with any blood product, including red blood cells, platelets and fresh, frozen plasma, gastroin- testinal (GI) bleeding, and steroid therapy were regarded as risk factors for candidemia when they occurred within 2 weeks of the onset of candidemia (15). Steroid therapy was defined as administration of ≥10 mg/day of prednisolone (or the equivalent dose of an alternative corticosteroid) or adminis- tration of <10 mg/day of prednisolone or its equivalent for more than 7 days. The use of immunosuppressive agents was defined as the administration of chemotherapeutic or anti- rheumatic agents within 2 weeks of the onset of candidemia (15). An immunocompromised state was defined as the pres- ence of a malignancy or the use of immunosuppressive agents during the same admission. Candida colonization was defined as a Candida species-positive culture of a sputum, urine, or fecal sample collected at any time before the onset of candi- demia.
Matching procedure
Control patients were selected from patients who did not have candidemia and were admitted to the MICU at about the same time as the candidemia patients. Control patients had no evidence of bacterial or fungal growth in blood cultures at any time during their hospitalization in the MICU. Con- trol patients were selected according to the following match- ing criteria: sex, age (±5 yr), and an Acute Physiology and Chronic Health Evaluation (APACHE) II score (16) of at least 5 on the day of admission to the MICU.
Statistical analysis
Continuous variables are expressed as the mean±standard deviation or as the median and interquartile range. Patient characteristics were compared between groups using the Mann- Whitney test for continuous variables and the chi-square test for categorical variables. To identify risk factors independent- ly associated with candidemia, variables that were significant according to a univariate analysis were subjected to binary logistic regression analysis. A P value <0.05 was considered significant. Kaplan-Meier survival curves were compared using the log-rank test. All statistical analyses were performed using SPSS software, version 12.0 (SPSS Inc., Chicago, IL, USA).
RESULTS Analysis of patients with candidemia
During the study period, 52 of 5,383 MICU admissions were identified as having fungemia. Three patients were infect- ed with species other than Candida (1 patient was positive for Aspergillus species and 2 patients were positive for Trichosporon beigelli). Therefore, we analyzed data from 49 patients.
The incidence of candidemia in the MICU was 9.1 per 1,000 admissions. The mean age of the patients was 57.6± 14.1 yr. There were more men than women in the sample (28:21). Among the candidemia patients, there was no sig- nificant difference in APACHE II score between the day of admission to the ICU and the day of onset of candidemia (23.8
±7.7 vs. 23.3±6.4, respectively; P=0.473).
Albicans was the predominant Candida species (32 cases, 65%); non-albicans Candida species accounted for 35% of infections (13 patients [27%]were infected with C. tropicalis, 3 patients [6%]were infected with C. parapsilosis, and 1 pati- ent [2%]was infected with C. glabrata). Thirty-five patients (71%) were treated with an antifungal agent: amphotericin B was administered to 25 patients and fluconazole was admin- istered to 10 patients. Eight of the 35 patients were treated with an antifungal agent before candidemia was diagnosed.
The median duration of antifungal treatment was 11 days (range, 1-45 days). Bacteremia was present before diagnosis of
candidemia in 20 patients (41%). Various causative organisms of bacteremia were detected: Clostridium perfringens, Escherichia coli, Enterobacter cloacae, Enterococcus faecium, Klebsiella pneumo- niae, Staphylococcus aureus, Pseudomonas aeruginosa, and Staphy- lococcus epidermidis. The median duration of antibiotic use before the onset of candidemia was 16 days (range, 1-92 days). All patients were treated with antibiotics before the onset of can- didemia.
Comparison of candidemia patients with matched control patients
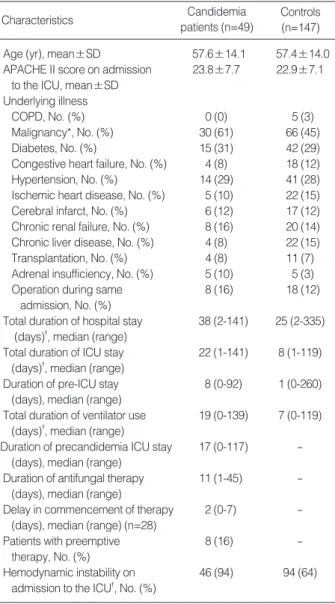
There were no significant differences in demographic char- acteristics or underlying diseases between the candidemia patients and the controls, except for the presence of malig- nancy (Table 1). Malignancy was more prevalent in patients with candidemia than in the control patients (P=0.048). This difference was not associated with solid malignancies (12 can- didemia patients [25%]vs. 35 control patients [24%]; P=
0.923) but with hematological malignancies (18 candidemia patients [37%]vs. 31 control patients [21%]; P=0.028). The dialysis method used for patients with chronic renal failure did not differ between the 2 groups. Patients with candidemia had longer stays in hospital and in the MICU compared with the control group, but there was no difference in their pre- ICU hospital stays (Table 1). Patients with candidemia were mechanically ventilated for a longer period during their total MICU stay than the controls (P=0.001) and had a longer MICU stay than the controls (P=0.001). At the time of MICU admission, patients with candidemia were more hemo- dynamically unstable than the controls (P<0.001).
Univariate analysis identified 8 variables that differed sig- nificantly between the candidemia patients and the controls (Table 2). These were central venous catheterization, candida colonization, an immunocompromised state, previous steroid therapy, transfusion, TPN, hepatic failure, and neutropenia on MICU admission. Multivariate analysis of these 8 vari-
*P<0.05 for candidemia patients vs. controls according to the chi-square test. �P≤0.05 for candidemia patients vs. controls according to the Mann- Whitney test.
APACHE, Acute Physiology and Chronic Health Evaluation; COPD, chron- ic obstructive pulmonary disease; ICU, intensive-care unit; duration of pre-ICU stay, general ward stay before ICU admission; duration of pre- candidemia ICU stay, days from ICU admission to candidemia; delay in start of therapy, days from diagnosis of candidemia to commence- ment of antifungal therapy; patients with preemptive therapy, patients treated with antifungal therapy before candidemia was diagnosed.
Characteristics Candidemia
patients (n=49)
Controls (n=147) Age (yr), mean±SD 57.6±14.1 57.4±14.0 APACHE II score on admission 23.8±7.7 22.9±7.1
to the ICU, mean±SD Underlying illness
COPD, No. (%) 0 (0) 5 (3)
Malignancy*, No. (%) 30 (61) 66 (45)
Diabetes, No. (%) 15 (31) 42 (29)
Congestive heart failure, No. (%) 4 (8) 18 (12)
Hypertension, No. (%) 14 (29) 41 (28)
Ischemic heart disease, No. (%) 5 (10) 22 (15)
Cerebral infarct, No. (%) 6 (12) 17 (12)
Chronic renal failure, No. (%) 8 (16) 20 (14) Chronic liver disease, No. (%) 4 (8) 22 (15)
Transplantation, No. (%) 4 (8) 11 (7)
Adrenal insufficiency, No. (%) 5 (10) 5 (3)
Operation during same 8 (16) 18 (12)
admission, No. (%)
Total duration of hospital stay 38 (2-141) 25 (2-335) (days)�, median (range)
Total duration of ICU stay 22 (1-141) 8 (1-119) (days)�, median (range)
Duration of pre-ICU stay 8 (0-92) 1 (0-260) (days), median (range)
Total duration of ventilator use 19 (0-139) 7 (0-119) (days)�, median (range)
Duration of precandidemia ICU stay 17 (0-117) - (days), median (range)
Duration of antifungal therapy 11 (1-45) - (days), median (range)
Delay in commencement of therapy 2 (0-7) - (days), median (range) (n=28)
Patients with preemptive 8 (16) -
therapy, No. (%)
Hemodynamic instability on 46 (94) 94 (64) admission to the ICU�, No. (%)
Table 1. Baseline characteristics of patients with candidemia and controls in an MICU
Variables
Candidemia patients
(n=49)
Controls
(n=147) OR 95% CI P *
Central venous catheter 42 (86) 67 (46) 6.1 2.7-14.0 <0.001 Nasogastric tube 42 (86) 138 (94) 0.4 0.1-1.1 NS Foley catheter 46 (94) 145 (82) 0.2 0.1-1.3 NS Candida colonization 14 (29) 23 (17) 2.2 1.1-4.6 0.045 Immunocompromised state 36 (75) 73 (50) 2.8 1.4-5.7 0.004 Previous steroid therapy 35 (71) 49 (33) 5.0 2.5-10.2 <0.001 Previous GI bleeding 8 (16) 17 (12) 1.5 0.6-3.7 NS Previous transfusion 40 (82) 50 (34) 8.6 3.9-19.2 <0.001 Previous TPN 11 (23) 7 (5) 5.8 2.1-15.9 <0.001 Hepatic failure on 9 (18) 6 (4) 5.3 1.8-15.7 0.001
admission to the ICU
ARF on admission 24 (49) 51 (35) 1.8 0.9-3.5 NS to the ICU
Neutropenia on 12 (25) 11 (8) 4.0 1.6-9.8 <0.001 admission to the ICU
Table 2. Results of univariate analysis for candidemia risk factors
Values are expressed as the number (%) of patients.
*Determined using the chi-squared test.
OR, odds ratio; CI, confidence interval; central venous catheter, internal jugular venous catheter, Hickman catheter, Swan-Ganz catheter, or fe- moral catheter; immunocompromised state, malignancy (hematologic or solid) or use of immunosuppressive agent; GI, gastrointestinal; TPN, total parenteral nutrition; ARF, acute renal failure; Neutropenia, absolute neutrophil count <500/μL.
ables using logistic regression revealed that central venous catheterization, previous steroid therapy, transfusion during the same admission, and hepatic failure on MICU admission were independent risk factors for candidemia (Table 3).
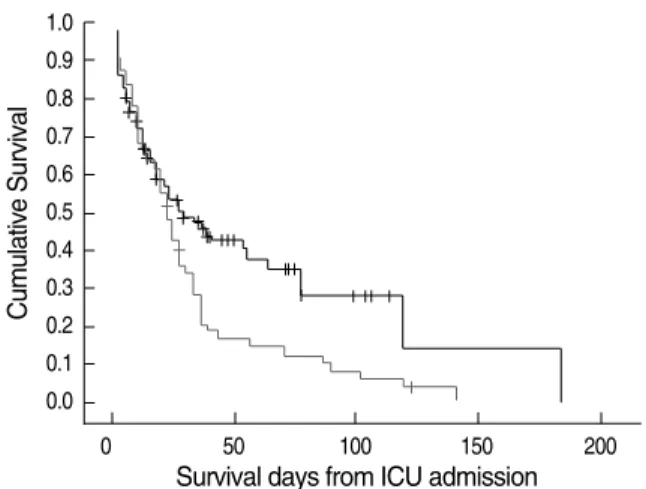
In-hospital mortality was 96% (47 of 49 patients) for pati- ents with candidemia and 52% (77 of 147 patients) for con- trol patients with odds ratio (OR) 21.4 (95% confidence inter- val [CI]5.0-91.2). The significance of this difference in mor- tality rate was confirmed using Kaplan-Meier survival curves (P=0.024; Fig. 1).
DISCUSSION
We performed a 1:3 matched case-control study to deter- mine the incidence of candidemia in MICU patients and the mortality rate among these patients and to identify factors asso- ciated with candidemia. We matched cases and controls on admission using variables known to be strongly correlated with nosocomial infections and the risk of death (e.g., severe ill- ness and age). There were no differences between cases and con- trols in underlying illnesses, except for malignancy. The dura- tion of the pre-ICU hospital stay did not differ significantly between groups.
In our study, the incidence of candidemia (9.1 patients per 1,000 admissions) and the crude mortality rate (96%) of can- didemia patients were greater than those of previous studies, in which the incidence of candidemia was 0.3-2.5 episodes per 1,000 admissions (4, 7, 12, 17) and the crude mortality rate was 31-61% (4-9). Lee et al. (18) reported that the incidence of candidemia in a Korean ICU was 0.3-1.5 episodes per 1,000 patient days and that the crude mortality was 48.3%. This discrepancy may have arisen because we included patients with severe disease and only enrolled MICU patients with a pre- existing risk factor for candidemia. Our study involved more patients with malignancy (61%) than previous studies (10- 41%) (4, 5, 9, 18), which may also have contributed to the relatively high incidence of candidemia in our study.
Attributable mortality in our study was 44% (96% minus 52%), which is similar to the results of previous studies (34- 49%). However, crude mortality was higher in our study than in previous studies (96% vs. 40-61%, respectively) (5, 9, 12,
18, 19). Of 8 patients who received preemptive antifungal therapy, only 1 survived. There are several potential explana- tions for the difference in crude mortality between our study and previous studies. First, criteria for enrollment in our study were stricter than those of other studies, which enrolled gen- eral ward patients whose mortality rate was lower than that of our patients (5, 9, 19). According to previous studies, an APACHE II score >20 during candidemia is associated with an elevated mortality rate (12) irrespective of intensive anti- fungal therapy (15). For this reason, we conducted an APACHE II score-matched case-control study. This matching procedure ensures that the control group is valid for comparison of mor- tality rate. Second, our study included more patients with malignancy (61%) than previous studies (10-41%) (4, 5, 9, 18). These factors may have been responsible for the high mortality rate in our study.
The Kaplan-Meier survival analysis showed that the differ- ence in mortality between the two groups was sustained (P=
0.024). In terms of underlying illness, the candidemia patients had more malignancies than the control patients (P=0.048).
Therefore, it could be inferred that the difference in the preva- lence of malignancy contributed to the difference in mortal- ity. However, survival analysis that excluded patients with a hematological malignancy showed a consistent result (P=
0.037 according to the log-rank test).
Many studies have been undertaken to evaluate risk fac- tors for the development of candidemia. However, most stud- ies were undertaken using specific patient populations or did not use case-control methodology (4, 10). Using a case-con- trol design, we identified several independent risk factors for candidemia in the MICU: central venous catheteriza- tion, previous steroid therapy, and previous transfusion.
This result is consistent with risk factors identified by other authors (5, 13, 20, 21).
We identified a new risk factor, viz., the presence of hepatic
*Determined using binary logistic regression analysis.
OR, odds ratio; CI, confidence interval.
Variables OR 95% CI P *
Central venous catheter 3.2 1.2-9.0 0.023
Previous steroid therapy 4.7 1.86-12.1 0.001
Previous transfusion 6.3 2.4-16.7 <0.001
Hepatic failure on 6.9 1.7-28.4 0.0075
admission to the ICU
Table 3. Results of multivariate logistic regression analysis for can- didemia risk factors
Fig. 1. Kaplan-Meier survival curves for candidemia patients and controls in an MICU. The solid line indicates the cumulative sur- vival of 49 patients with candidemia and the dashed line indi- cates the cumulative survival of 147 control patients (P=0.024).
Cumulative Survival
1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0.0
0 50 100 150 200
Survival days from ICU admission
failure on admission to the MICU. A previous study reported that fungal infection (predominantly candidiasis) is a common complication (32%) in patients with acute liver failure (22).
However, there are few reports on hepatic failure as an inde- pendent risk factor for candidemia. In our study, 9 patients in the candidemia group had hepatic failure on admission to the MICU. Using multivariate analysis, we identified hepat- ic failure on admission to the MICU as an independent risk factor for candidemia (OR, 7.6 ; 95% CI, 1.5-39.0). Hepat- ic failure may be a risk factor because patients with hepatic failure have increased susceptibility to infection because of abnormal immune function (23), increased colonization of the small bowel (24, 25), impaired phagocytic function (26, 27), or reduced complement levels (28).
Our study has several limitations. First, the incidence of candidemia in the MICU might have been underestimated.
Because this was a retrospective study, no special fungal blood cultures were performed. In our hospital, blood is cultured for 5 days using a Bact/Alert 3D instrument (BioMerieux, Inc., Durham, NC, USA) when a routine blood culture is request- ed. If no growth is identified after 5 days, the blood culture is terminated. However, if a fungal blood culture is request- ed, the blood is cultured for 3 weeks to identify any slow-grow- ing Candida species. Several authors have reported that they cultured blood for more than 5 days to identify specific slow- growing organisms. Therefore, it has been suggested that the appropriate duration for blood culture should be determined on an individual basis according to the clinical relevance of the culture (29, 30). A prospective study would have avoid- ed this methodological weakness.
Second, the control patients had no evidence of bacterial or fungal growth in their blood cultures. However, systemic bacterial or fungal infections may be present even if blood cul- tures are negative. In this study, 67 patients (46%) in the con- trol group used empirical antibiotics. Therefore, the control group may have included infected patients. However, circum- vention of this situation is clinically very difficult. Therefore, we performed a multivariate analysis that included antibiotic use as a variable.
In conclusion, bloodstream Candida infections in MICUs are associated with much higher crude mortality rates than would be expected for uninfected patients with the same dis- ease severity. We identify an additional independent risk fac- tor for candidemia, the presence of hepatic failure on MICU admission. Therefore, increased awareness of risk factors, in- cluding hepatic failure, is necessary for the management of candidemia.
ACKNOWLEDGEMENTS
We thank Professor Eui Chong Kim of the Department of Laboratory medicine for his approval and support for this work. We are grateful to the doctors and nurses of medical
intensive-units; the medical records officer of Seoul Nation- al University Hospital. All authors have no financial sup- port.
REFERENCES
1. Eggimann P, Garbino J, Pittet D. Epidemiology of Candida species infections in critically ill non-immunosuppressed patients. Lancet Infect Dis 2003; 3: 685-702.
2. Bassetti M, Righi E, Costa A, Fasce R, Molinari MP, Rosso R, Pallavicini FB, Viscoli C. Epidemiological trends in nosocomial candidemia in intensive care. BMC Infect Dis 2007; 6: 21.
3. Wisplinghoff H, Bischoff T, Tallent SM, Seifert H, Wenzel RP, Edmond MB. Nosocomial bloodstream infections in US hospitals:
analysis of 24,179 cases from a prospective nationwide surveillance study. Clin Infect Dis 2004; 39: 309-17.
4. Klingspor L, Tornqvist E, Johansson A, Petrini B, Forsum U, Hedin G. A prospective epidemiological survey of candidaemia in Sweden.
Scand J Infect Dis 2004; 36: 52-5.
5. Puzniak L, Teutsch S, Powderly W, Polish L. Has the epidemiology of nosocomial candidemia changed? Infect Control Hosp Epidemiol 2004; 25: 628-33.
6. Morgan J, Meltzer MI, Plikaytis BD, Sofair AN, Huie-White S, Wilcox S, Harrison LH, Seaberg EC, Hajjeh RA, Teutsch SM. Excess mortali- ty, hospital stay, and cost due to candidemia: a case control study using data from population-based candidemia surveillance. Infect Control Hosp Epidemiol 2005; 26: 540-7.
7. Alonso-Valle H, Acha O, Garcia-Palomo JD, Farinas-Alvarez C, Fer- nandez-Mazarrasa C, Farinas MC. Candidemia in a tertiary care hos- pital: epidemiology and factors influencing mortality. Eur J Clin Microbiol Infect Dis 2003; 22: 254-7.
8. Jamal WY, El-Din K, Rotimi VO, Chugh TD. An analysis of hospi- tal-acquired bacteremia in intensive care unit patients in a universi- ty hospital in Kuwait. J Hosp Infect 1999; 43: 49-56.
9. Gudlaugsson O, Gillespie S, Lee K, Vande Berg J, Hu J, Messer S, Herwaldt L, Pfaller M, Diekema D. Attributable mortality of noso- comial candidemia, revisited. Clin Infect Dis 2003; 37: 1172-7.
10. Nieto-Rodriguez JA, Kusne S, Manez R, Irish W, Linden P, Magnone M, Wing EJ, Fung JJ, Starzl TE. Factors associated with the devel- opment of candidemia and candidemia-related death among liver transplant recipients. Ann Surg 1996; 223: 70-6.
11. McNeil MM, Nash SL, Hajjeh RA, Phelan MA, Conn LA, Plikaytis BD, Warnock DW. Trends in mortality due to invasive mycotic dis- eases in the United States, 1980-1997. Clin Infect Dis 2001; 33: 641-7.
12. Nolla-Salas J, Stiges-Serra J, Leon-Gil C, Martinez-Gonzalez J, Leon- Regidor MA, Ibanez-Lucia P, Torres-Rodriguez JM. Candidemia in non-neutropenic critically ill patients: analysis of prognostic factors and assessment of systemic antifungal therapy. Intensive Care Med 1997; 23: 23-30.
13. Vincent JL, Anaissie E, Bruining H, Demajo W, el-Ebiary M, Haber J, Hiramatsu Y, Nitenberg G, Nystrom PO, Pittet D, Rogers T, Sand- ven P, Sganga G, Schaller MD, Solomkin J. Epidemiology, diagno- sis, and treatment of systemic Candida infection in surgical patients
under intensive care. Intensive Care Med 1998; 24: 206-16.
14. Herbrecht R. Managing the challenges of invasive fungal infections.
Int J Antimicrob Agents 2006; 27 (Suppl 1): 1-2.
15. Rex JH, Pappas PG, Karchmer AW, Sobel J, Edwards JE, Hadley S, Brass C, Vazquez JA, Chapman SW, Horowitz HW, Zervos M, McK- insey D, Lee J, Babinchak T, Bradsher RW, Cleary JD, Cohen DM, Danziger L, Goldman M, Goodman J, Hilton E, Hyslop NE, Kett DH, Lutz J, Rubin RH, Scheld WM, Schuster M, Simmons B, Stein DK, Washburn RG, Mautner L, Chu TC, Panzer H, Rosenstein RB, Booth J; National Institute of Allergy and Infectious Diseases Mycoses Study Group. A randomized and blinded multicenter trial of high-dose flu- conazole plus placebo versus fluconazole plus amphotericin B as therapy for candidemia and its consequences in nonneutropenic sub- jects. Clin Infect Dis 2003; 36: 1221-8.
16. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II:
a severity of disease classification system. Crit Care Med 1985; 13:
818-29.
17. Blot SI, Vandewoude KH, Hoste EA, Colardyn FA. Effects of nosoco- mial candidemia on outcomes of critically ill patients. Am J Med 2002;
113: 480-5.
18. Lee YH, Choi HJ, Lee MA. Risk factors for the development of noso- comial candidemia among patients in intensive care unit. Infect Chemother 2004; 36: 219-26.
19. Wey SB, Mori M, Pfaller MA, Woolson RF, Wenzel RP. Hospital- acquired candidemia. The attributable mortality and excess length stay. Arch Intern Med 1998; 148: 2642-5.
20. Maschmeyer G. The changing epidemiology of invasive fungal infec- tions: new threats. Int J Antimicrob Agents 2006; 27 (Suppl 1) : 3-6.
21. Falagas ME, Apostolou KE, Pappas VD. Attributable mortality of can-
didemia: a systematic review of matched cohort and case control stud- ies. Eur J Clin Microbiol Infect Dis 2006; 25: 419-25.
22. Rolando N, Harvey F, Brahm J, Philpott-Haward J, Alexander G, Casewell M, Fagan E, Williams R. Fungal infection: a common, unrecognized complication of acute liver failure. J Hepatol 1991;
12: 1-9.
23. Rolando N, Philpott-Howard J, Williams R. Bacterial and fungal infec- tion in acute liver failure. Semin Liver Dis 1996; 16: 389-402.
24. Chang CS, Chen GH, Lien HC, Yeh HZ. Small intestine dysmotility and bacterial overgrowth in cirrhotic patients with spontaneous bac- terial peritonitis. Hepatology 1998; 28: 1187-90.
25. Fisher NC, Cooper MA, Hastings JG, Mutimer DJ. Fungal colonisa- tion and fluconazole therapy in acute liver disease. Liver 1998; 18:
320-5.
26. Gomez F, Ruiz P, Schreiber AD. Impaired function of macrophage Fc? receptors and bacterial infection in alcoholic cirrhosis. N Engl J Med 1994; 331: 1122-8.
27. Guarner C, Runyon BA. Macrophage function in cirrhosis and the risk of bacterial infection. Hepatology 1995; 22: 367-9.
28. Homann C, Varming K, Hogasen K, Mollnes TE, Graudal N, Thomsen AC, Garred P. Acquired C3 deficiency in patients with alco- holic cirrhosis predisposes to infection and increased mortality. Gut 1997; 40: 544-9.
29. Reisner BS, Woods GL. Times to detection of bacteria and yeasts in BACTEC 9240 blood culture bottles. J Clin Microbiol 1999; 37:
2024-6.
30. Saito T, Senda K, Takakura S, Fujihara N, Kudo T, Iinuma Y, Tani- moto M, Ichiyama S. Detection of bacteria and fungi in BacT/Alert standard blood-culture bottles. J Infect Chemother 2003; 9: 227-32.