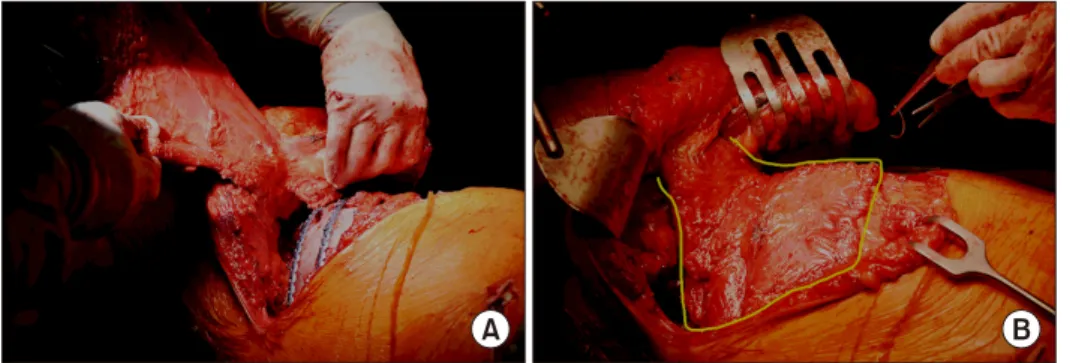
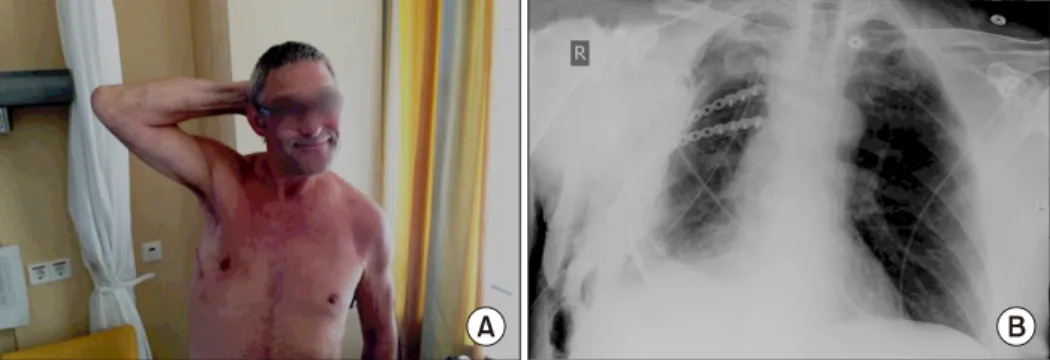
Reconstruction of Chest Wall Defects Using a Technique Involving Mesh, Titanium Plates, and a Pedunculated Muscle Flap
4
0
0
전체 글
(2)
(3)
(4)
수치
관련 문서
In the efficiency review of the Trombe wall system through the experiment, if the Trombe wall was applied in the building structure, the Trombe wall had the
Salama H, Rose LF, Salama M, Betts NJ : Immediate loading of bilaterally splinted titanium root-form implants in fixed prosthodontics.. A technique reexamined:
Alveolar ridge augmentation with titanium mesh and a combination of autogenous bone and anorganic bovine bone: a 2-year prospective study.. Corinaldesi G, Pieri F, Sapigni
success rates of dental implants placed at the time of or after alveolar ridge augmentation with an autogenous mandibular bone graft and titanium mesh: a 3-to
This study was to do a comparative analysis on kinematic differences and differences in muscle activity between the skilled and the unskilled in windsurfing
The third was combination of levator palpebrae, superior rectus, inferior oblique muscle weakness(n=5) and the fourth was the third group plus medial rectus
The preparation of osseodensification technique should start with a smaller diameter than conventional technique because of the recovery of elastic strain. It
Results: The results demonstrated a significant positive correlation between the muscle atrophy and the tendon tear.(p<0.05) And there was statistically
