J Health Tech Assess 2014;2(2):114-123 ISSN 2288-5811
Copyright © 2014 The Korean Association for Health Technology AssessmentComparison of Zotarolimus-Eluting Stent and
Everolimus-Eluting Bioresorbable Vascular Scaffold in Patient with Coronary Artery Disease:
A Systematic Review and Adjusted Indirect Comparison
Hyung-Deuk Park, MSc, RAC, So-Jung Yoo, BA, CCRA, Eun-Young Jung, BA, CCRA, Soo-Yeon Lee, MSc, Ji-Sun Yu, MPH, and Sang-Soo Lee, MBA
Corporate Affairs, Medtronic Korea, Seoul, Korea
관상동맥질환 치료를 위한 조타롤리무스 금속형 약물 방출스텐트와 에버롤리무스 생체흡수성 약물방출 스텐트 간의 안전성·효과성 비교:
체계적 문헌고찰 및 공통대조군 간접비교
메드트로닉코리아
박형득·유소정·정은영·이수연·유지선·이상수
Received September 17, 2014 Accepted September 30, 2014 Address for Correspondence:
Hyung-Deuk Park, MSc, RAC Corporate Affairs, Medtronic Korea, 4F Sajo Building, 424 Yeongdong- daero, Gangnam-gu, Seoul 135-502, Korea
Tel: +82-2-3404-7744 Fax: +82-2-562-7168
E-mail: [email protected]
Objectives:
Recently bioresorbable coronary stent has emerged as new version of percutaneous coro- nary intervention (PCI) technology. The expected benefits of this new technology are the reduction of stent thrombosis and impairment of coronary vasomotion. However, the comparative outcomes between bioresorbable coronary stent and current drug-eluting stents (DESs) are not known. This study is aimed to compare the safety and effectiveness of emerging bioresorbable coronary stents - everolimus-eluting bioresorbable vascular scaffold (BVS) to the well accepted DES technology - zo- tarolimus-eluting stent (ZES) - through Systematic Review and Adjusted Indirect Comparison with everolimus eluting stents (EES) for coronary artery disease (CAD) treatments.Methods:
A meta- analysis of clinical studies in which patients were randomly assigned to ZES versus EES or BVS ver- sus EES were performed, as well as an indirect comparison of ZES versus EES, with EES common comparator. The primary endpoint was target lesion revascularization (TLR), while the secondary endpoints were a target vessel revascularization (TVR), a death, and a major adverse cardiac event (MACE).Results:
Six clinical studies were identified with a total of 7512 patients. Treatments with ZES versus EES were not associated with significant reductions of the TLR [odds ratio (95% confi- dence interval)=1.13 (0.88, 1.47), p=0.34], TVR [1.05 (0.81, 1.37), p=0.72], death [0.89 (0.64, 1.25),p=0.51], MACE [1.02 (0.85, 1.23), p=0.79] and Stent Thrombosis (ST) [1.35 (0.91, 2.00), p=0.13]
BVS versus EES therapy also were not associated with significant reductions of TLR [0.59 (0.14, 2.53), p=0.47], TVR [0.48 (0.11, 1.99), p=0.31], death [0.33 (0.01, 8.20), p=0.50] and MACE [0.41 (0.10, 1.63), p=0.21]. The adjusted indirect comparison found that there were no differences be- tween ZES and BVS in the risk of TLR [1.92 (0.44, 8.31), p=0.61], TVR [2.19 (0.52, 9.14), p=0.29], death [2.70 (0.09, 78.53), p=0.75] and MACE [2.49 (0.61, 10.20), p=0.29].
Conclusion:
In patients with CAD, BVS has similar safety and effectiveness as that of ZES. In the case of indirect compari- son, ZES and BVS may have comparable results in their effectiveness and safety. Long-term and large-scale randomized studies are required to confirm the study results.Key Words
Bioresorbable vascular scaffold · Zotarolimus · Everolimus · Drug eluting stent · Coronary artery disease.Original Article
JoHTA
서 론
관상동맥질환(coronary artery disease, 이하 CAD)은 죽상 경화성 플라크(atherosclerotic plaque)가 침적되어 관상동맥 혈관 내부가 좁아져서 심근으로 전달되는 산소가 부족해지 는 질환을 의미한다. 관상동맥질환의 유발원인이 다양하며, 흡연, 비만, 당뇨, 고혈압 및 가족력 등이 주요한 위험인자로 알려져 있다.1) 관상동맥질환은 전 세계적으로 60세 이상 고령 환자의 사망원인 1순위 질환이며,2) 건강관련 삶의 질(he- alth-related quality of life)을 심각하게 저하시키는 질환 중 하나로, 특히 심근경색이나 협심증의 증상 발생시 신체 기능 저하와 더불어 우울증과 같은 정신학적 손상을 동반함으로써 환자에게 있어 심각한 사회활동을 제한하는 질환이기도 하다.3)
지난 1987년 세계 최초로 Palmaz-Schatz 금속 스텐트가 개발된 이후, 관상동맥질환을 치료하기 위한 스텐트 사용은 폭발적으로 증가해 왔다.4) 하지만 종래의 금속 스텐트는 혈관 에 스텐트 이식 후 혈관 내피세포 증식(endothelial prolifer- ation)으로 인해 스텐트 내부가 또다시 폐색되는 스텐트내 재 협착(in-stent restenosis)을 발생시키는 문제점을 안고 있었 다.5) 최근에 항증식성 약물을 포함한 약물방출스텐트가 개발 되면서 스텐트내 재협착 문제는 대부분 해결되었다.6) 이렇듯 급성 또는 중증의 관상동맥질환 환자에게 있어 약물방출스 텐트 사용은 표준적 치료법으로 자리잡게 되었다.
최근 들어 생체 흡수성 재질의 약물방출스텐트에 대한 연 구가 급속도로 이뤄져 왔다. 금속형 약물방출스텐트를 사용 할 경우 일정기간 항응고제를 복용해야 하는 불편과 더불어 발생률이 낮기는 하지만 스텐트혈전증(stent thrombosis)의 발생위험이 존재한다. 이러한 단점을 보완하기 위한 방안으 로 생체흡수성 재질의 약물방출스텐트 개발의 필요성이 제 기되었다.7) 이러한 생체흡수성 재질로 된 약물방출스텐트가 종래의 금속형 재질의 약물방출 스텐트에 비해 여러 장점을 지닐 것으로 예상되지만,8-12) 이 두 스텐트 간의 직접비교 연구 는 아직까지 부족하여 생체흡수성 약물방출스텐트의 치료 효과는 아직까지는 불명확한 상황이다.
본 연구는 현재 국내에서 널리 사용되고 있는 조타롤리무 스 금속형 약물방출스텐트(zotarolimus-eluting stent, 이하 ZES)와 에버롤리무스 생체흡수성 약물방출스텐트(everoli- mus-eluting bioresorbable vascular scaffold, 이하 BVS) 간 의 안전성과 효과성을 평가하기 위해 에버롤리무스 금속형 약물방출스텐트(everolimus-eluting stent, 이하 EES)를 공 통대조군(common comparator)으로 한 간접비교를 실시하 였다.
방 법
체계적 문헌고찰
연구에 포함될 문헌 검색은 PubMed, EMBASE, Coch- rane library 데이터베이스를 통해 실시되었다. 검색에 사용 된 키워드는 다음과 같다-“coronary artery disease”, “zo- tarolimus eluting stent”, “everolimus eluting stent”, “biore- sorbable vascular scaffold”, “resolute”, “xience”, “absorb”
(부록 1-3). 문헌 선택기준(inclusion criteria)은 관상동맥질 환 환자 치료에 대한 무작위 대조 임상 시험 연구, ZES, BVS 및 EES를 사용한 연구, 적절한 의료결과를 보고한 연구, 그 리고 관찰 연구 문헌일지라도 성향점수(propensity score) 방법 등을 통해 교란요인을 보정한 경우 선택문헌으로 포함 하였다. 배제기준(exclusion criteria)은 무작위 대조 연구가 아닌 경우, 동물실험 및 전임상 시험 연구, 원저가 아닌 연구 그리고 회색문헌으로 결정하였다. 다만, 문헌 중에 초기 연 구 발표 이후 추적 관찰한 결과가 추가로 보고된 연구는 원 칙적으로 배제하였으나 지속 출판된 문헌의 결과 중 필요한 내용은 최종 선택된 문헌에 포함시켰으며, 연구대상이 동일 하고 연구결과가 전체적 혹은 부분적으로 포함된 연구는 중 복출판 연구로 배제하였다.
공통대조군 간접비교
EES를 공통대조군으로 설정하고 ZES와 BVS 간의 치료 효과 비교는 Bucher 등13)이 제안한 공통대조군 간접비교 이 론을 바탕으로 실시하였다.
데이터 추출 및 비뚤림 측정
두 명의 연구자가 일차적으로 문헌의 초록(abstract)을 독 립적으로 검토하여, 문헌의 선정 및 배제 여부를 결정하였 다. 최종 선정된 문헌들에 대한 비뚤림 측정은 Cochrane이 제안한 ‘Risk of Bias’ 도구를 통하여 문헌의 질 평가를 실시 하였다.14)
연구 결과 변수
본 연구의 일차 연구목적(primary endpoint)은 ‘목표병변 부 재시술률(target lesion revascularization, 이하 TLR)’로 결정하였고, 이차 연구목적(secondary endpoint)는 ‘목표혈 관부 재시술률(target vessel revascularization, 이하 TVR)’, 사망(death), 그리고 주요 심혈관 관련 부작용(major adverse cardiac event, 이하 MACE)으로 설정하였다.
통계분석
ZES와 EES 간의 통합 치료효과 그리고 BVS와 EES 간의 통합 치료효과는 각각 오즈비(평균 및 95% 신뢰구간)로 분 석되었다. 통합 오즈비 계산을 위해서 RevMan software[Re- view Manager(RevMan) Version 5.2. The Cochrane Col- laboration, London, UK]의 Mantel-Haenszel 고정효과 모 형이 사용되었고, 통합 오즈비 간의 공통대조군 간접비교 효 과 추정치는 Indirect Treatment Comparison(ITC Version 1.0, CADTH, Ontario, Canada)과 R(R version 3.1.0, R Fo- undation)을 통해 분석하였다.
결 과
최종 포함된 문헌
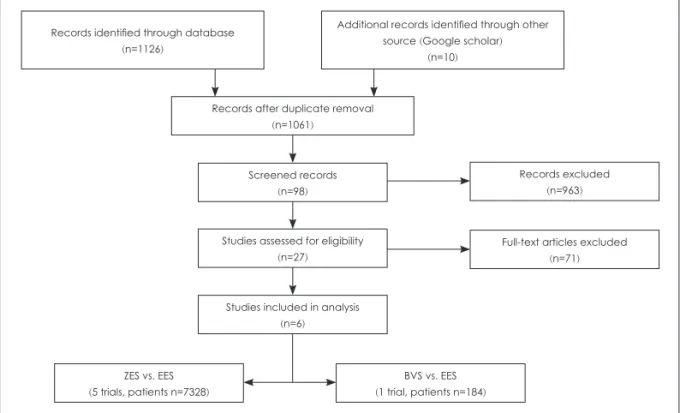
연구에 포함할 문헌의 선택 배제는 preferred reporting items of systematic reviews and meta-analyses(이하 PRI- SMA) 흐름도에 따라 실시하였고, 전체적인 문헌 선택과정 은 다음과 같다(그림 1). 문헌 검색 결과 PubMed에서 432건 의 문헌, EMBASE에서 606건의 문헌, Cochrane에서 88건 의 문헌, 그리고 기타 자료원(google scholar)을 통해 10건의 문헌이 추가적으로 검색되었다. 즉, 문헌 검색 전략에 따라 검색된 문헌은 총 1136건이 검색되었다. 중복문헌 제거 과 정을 통해 총 75건의 문헌을 배제하였고, 남은 1061건의 문 헌에 대해 일차적으로 초록을 중심으로 문헌을 검토하는 작 업이 실시되었다. 초록의 내용만으로 내용 확인이 불가능한
경우 전문을 확인하는 과정을 거쳤으며, 이 과정을 통해 원 저가 아닌 문헌, 연구대상 환자가 아닌 문헌 그리고 연구 대 상 중재법이 사용되지 않은 문헌 총 962건을 추가적으로 배 제하고 선별대상 문헌으로 99건의 문헌을 선정하였다. 이 중 ZES와 EES를 비교한 문헌은 57건 그리고 BVS와 EES를 비 교한 문헌은 42건으로 확인되었다. 선별대상 문헌에 대하여 추가적으로 초록에 대한 평가가 실시되었고, 연구대상 환자 가 포함되지 않거나 연구대상 중재법이 사용되지 않은 문헌 그리고 무작위 대조임상연구가 아닌 문헌 총 71건이 추가적 으로 배제되었고 27건의 문헌을 검토대상으로 선정하였다.
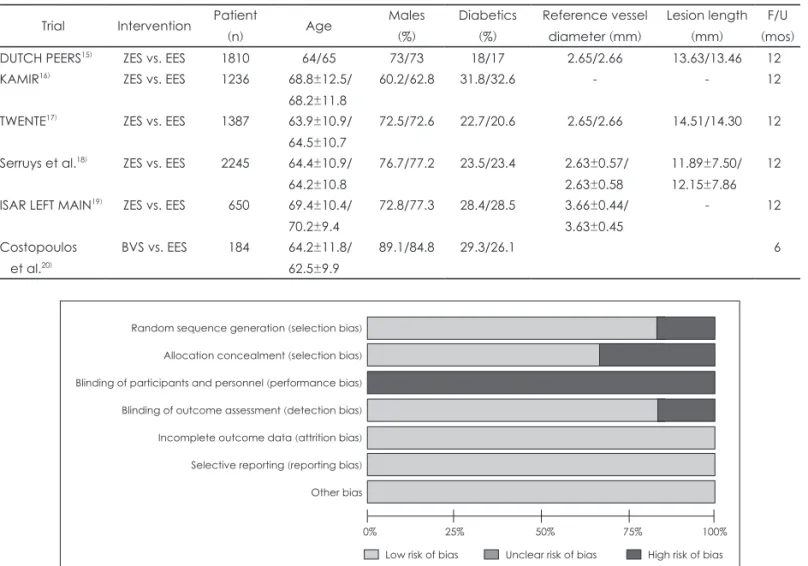
이 중 ZES와 EES를 비교한 문헌은 18건 그리고 BVS와 EES를 비교한 문헌은 9건으로 확인되었다. 선별된 문헌의 전문(full-text)에 대한 평가가 실시되었고, 최종적으로 총 6 건의 문헌이 본 연구에 포함되었다. 최종 선정된 6건의 문헌 중, 5편은 ZES와 EES 간의 치료 효과 비교에 관한 문헌이었 고 나머지 1편은 BVS와 EES 간의 치료 효과 비교에 관한 문헌이었다(표 1).
문헌의 질 평가
선택된 문헌의 질 평가는 cochrane에서 제안하는 risk of bias 도구를 사용하였다. 의료기기의 특성상 이중 맹검이 제 대로 실시되지 않아 ‘performance bias’가 높게 분석되었고
‘selection bias’와 ‘detection bias’에 대한 언급이 문헌상에 명 확히 명시되어 있지 않아 비뚤림의 위험성이 높은 것으로 평가되었다(그림 2, 3).
Records identified through database (n=1126)
Records after duplicate removal (n=1061)
Screened records (n=98)
Studies assessed for eligibility (n=27)
Studies included in analysis (n=6)
ZES vs. EES (5 trials, patients n=7328)
BVS vs. EES (1 trial, patients n=184)
Records excluded (n=963)
Full-text articles excluded (n=71) Additional records identified through other
source (Google scholar) (n=10)
Fig. 1. PRISMA flow chart for the trial selection process.
통합 추정치 결과
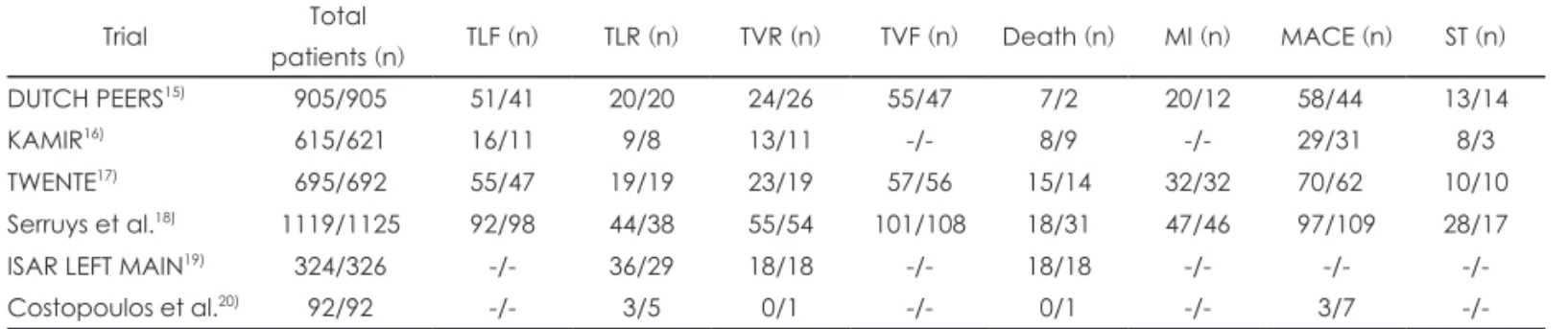
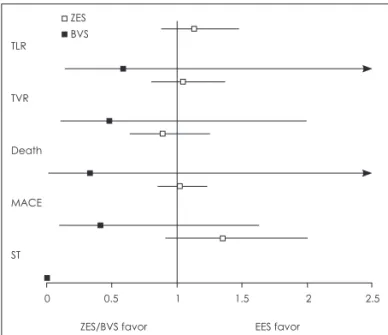
연구에 포함된 각 문헌들의 결과 요약치는 표 2에 요약되 어 있으며, ZES와 EES 그리고 BVS와 EES 간의 통합 추정 치는 표 3과 그림 4에 요약되어 있다.
ZES vs. EES
목표병변부 재시술률(TLR)은 ZES 치료군에서 총 128명 (3.5%), 그리고 EES 치료군에서 총 145명(3.1%)이었다. ZES 에 비해 EES 사용이 TLR을 소폭 감소시켜 주는 것으로 나타 났으나 통계적으로 유의한 차이는 발생되지 않았다 [OR(95%
CI)=1.13(0.88, 1.47), p=0.58, I2=0%, χ2=0.26]. 목표혈관부 재시술률(TVR)은 ZES 치료군에서 총 115명(3.1%), 그리고 EES 치료군에서 총 110명(3.0%)이었다. ZES에 비해 EES 사용이 TVR을 소폭 감소시켜주는 것으로 나타났으나 통계 적으로 유의한 차이는 발생되지 않았다[1.05(0.81, 1.37), p=
0.72, I2=0%, χ2=0.53]. 사망은 ZES 치료군에서 총 66건 (1.8%), 그리고 EES 치료군에서 총 74건(2.0%) 발생하였다.
EES에 비해 ZES 사용이 사망 위험률을 감소시켜주는 것으 로 나타났으나 통계적으로 유의한 차이는 발생되지 않았다
[0.89(0.64, 1.25), p=0.44, I2=42%, χ2=5.19]. 주요 심혈관 관 련 부작용(MACE)은 ZES 치료군에서 총 254건(6.9%), 그리 고 EES 치료군에서 총 246건(6.7%) 발생하였다. 주요 심혈 관 관련 부작용에 대한 ZES와 EES 간의 위험 발생률은 통 계적으로 차이가 없었다[1.02(0.85, 1.23), p=0.79, I2=0%, χ2
=2.88]. 스텐트 혈전증(stent thrombosis)은 ZES 치료군에서 총 59건(1.6%), 그리고 EES 치료군에서 총 44건(1.2%) 발생 하였다. ZES에 비해 EES 사용이 스텐트 혈전증 발생 위험 률을 감소시켜주는 것으로 나타났으나 이 또한 통계적으로 유의한 차이는 없었다[1.35(0.91, 2.00), p=0.13, I2=0%, χ2= 2.93].
BVS vs. EES
목표병변부 재시술률(TLR)은 BVS 치료군에서 총 3명 (3.3%), 그리고 EES 치료군에서 총 5명(5.4%)이었다. EES 에 비해 BVS 사용이 TLR을 낮춰주는 경향성을 보였으나 통계적으로 유의한 차이는 없었다[OR(95%CI)=0.59(0.14, 2.52), p=0.47]. 목표혈관부 재시술률(TVR)은 BVS 치료군에 서 총 3명(3.3%), 그리고 EES 치료군에서 총 6명(6.54%)에
Table 1. Main characteristics of patients enrolled among trials included in the study
Trial Intervention Patient
(n) Age Males
(%)
Diabetics (%)
Reference vessel diameter (mm)
Lesion length (mm)
F/U (mos)
DUTCH PEERS
15)ZES vs. EES 1810 64/65 73/73 18/17 2.65/2.66 13.63/13.46 12
KAMIR
16)ZES vs. EES 1236 68.8±12.5/
68.2±11.8
60.2/62.8 31.8/32.6 - - 12
TWENTE
17)ZES vs. EES 1387 63.9±10.9/
64.5±10.7
72.5/72.6 22.7/20.6 2.65/2.66 14.51/14.30 12
Serruys et al.
18)ZES vs. EES 2245 64.4±10.9/
64.2±10.8
76.7/77.2 23.5/23.4 2.63±0.57/
2.63±0.58
11.89±7.50/
12.15±7.86 12
ISAR LEFT MAIN
19)ZES vs. EES 650 69.4±10.4/
70.2±9.4
72.8/77.3 28.4/28.5 3.66±0.44/
3.63±0.45
- 12
Costopoulos et al.
20)BVS vs. EES 184 64.2±11.8/
62.5±9.9
89.1/84.8 29.3/26.1 6
0% 25% 50% 75% 100%
Low risk of bias Unclear risk of bias High risk of bias Random sequence generation (selection bias)
Allocation concealment (selection bias) Blinding of participants and personnel (performance bias) Blinding of outcome assessment (detection bias) Incomplete outcome data (attrition bias) Selective reporting (reporting bias) Other bias
Fig. 2. Analysis of risk of each included trials according to the Cochrane Collaboration tool.
서 발생되었다. 마찬가지로 EES에 비해 BVS 사용이 TVR 을 낮춰주는 경향성을 보였으나 통계적으로 유의한 차이는 없었다[0.48(0.12, 2.00), p=0.31]. 환자 사망은 BVS 치료군에 서 총 0명(0%), 그리고 EES 치료군에서 총 1명(1.1%) 발생 되었다. EES에 비해 BVS 사용이 환자 사망의 위험성을 낮 춰주는 경향성을 보였으나 통계적으로 유의한 차이는 없었 다[0.33(0.01, 8.20), p =0.50]. 주요 심혈관 관련 부작용 (MACE)은 BVS 치료군에서 총 3건(3.3%), 그리고 EES 치 료군에서 총 7건(7.6%) 발생되었다. 주요 심혈관 관련 부작 용에 대해 BVS가 EES에 비해 우수한 경향을 보였으나 통
계적 유의성 차이는 발생되지 않았다[0.41(0.10, 1.63), p=0.20].
간접비교결과
공통대조군 간접비교 분석을 통한 ZES와 BVS 간의 안전 성 효과성 비교 결과, 두 치료군 간 치료효과에 대한 통계적 으로 유의한 차이는 없었다(표 4). 두 치료군 간 목표병변부 재시술률[OR(95%CI)=1.92(0.44, 8.31), p=0.61], 목표혈관부 재시술률[2.19(0.52, 9.14), p=0.29], 사망률[2.70(0.09, 78.54), p=0.75] 그리고 주요 심혈관 관련 부작용[2.49(0.61, 10.20),
Fig. 3. Analysis of risk of each included trials according to the Cochrane Collaboration tool.
Random sequence generation (selection bias) Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias) Blinding of outcome assessment (detection bias) Incomplete outcome data (attrition bias) Selective reporting (reporting bias) Other bias
+ + + +
+ +
+ +
+ + + +
+ +
+ + +
+ +
+ + + +
+ +
+ + + + +
+ +
––
––
–
– – – –
– Costopoulos 2014DUTCH PEERS 2014ISA-LEFT-MAIN 2013
KAMIR 2014
Serruys 2010
TWENTE 2012
Table 2. Main outcomes event among trials included in the study
Trial Total
patients (n) TLF (n) TLR (n) TVR (n) TVF (n) Death (n) MI (n) MACE (n) ST (n)
DUTCH PEERS
15)905/905 51/41 20/20 24/26 55/47 7/2 20/12 58/44 13/14
KAMIR
16)615/621 16/11 9/8 13/11 -/- 8/9 -/- 29/31 8/3
TWENTE
17)695/692 55/47 19/19 23/19 57/56 15/14 32/32 70/62 10/10
Serruys et al.
18)1119/1125 92/98 44/38 55/54 101/108 18/31 47/46 97/109 28/17
ISAR LEFT MAIN
19)324/326 -/- 36/29 18/18 -/- 18/18 -/- -/- -/-
Costopoulos et al.
20)92/92 -/- 3/5 0/1 -/- 0/1 -/- 3/7 -/-
Table 3. Outcome estimates of endpoints in ZES and BVS groups Endpoint
ZES group BVS group
Incidence
(ZES/EES, %) OR (95%CI)
p valueI
2(%) χ
2Incidence
(BVS/EES, %) OR (95%CI)
p valueTLR 3.5/3.1 1.13 (0.88, 1.47) 0.34 0 0.55 3.3/5.4 0.59 (0.14, 2.53) 0.47
TVR 3.1/3.0 1.05 (0.81, 1.37) 0.72 0 0.53 3.3/6.5 0.48 (0.11, 1.99) 0.31
Death 1.8/2.0 0.89 (0.64, 1.25) 0.51 26 5.39 0/1.1 0.33 (0.01, 8.20) 0.50
MACE 6.9/6.7 1.02 (0.85, 1.23) 0.79 0 2.88 3.3/7.6 0.41 (0.10, 1.63) 0.21
ST 1.6/1.2 1.35 (0.91, 2.00) 0.13 0 2.93 -/- - -
p=0.29] 간의 차이는 없는 것으로 분석되었다.
고 찰
급성 및 중증 관상동맥질환 환자를 치료하는 데 있어 금속 형 약물방출 스텐트를 이용한 경피적 관상동맥 중재술은 표 준적 시술법으로 자리잡고 있다. 조타롤리무스 또는 에버롤 리무스로 대표되는 2세대 약물방출 스텐트들은 개선된 항증 식성 약물과 생체적합성 폴리머 사용을 통해 기존 약물방출 스텐트의 가장 큰 단점인 스텐트 혈전증 발생을 현저히 낮 추었다. 이러한 약물방출스텐트의 발전에도 불구하고 환자 체내에 평생 금속성 스텐트를 이식해야 하는 제한점을 극복 하기 위해 최근 생체흡수성 재질을 이용한 약물방출스텐트 에 대한 연구가 활발히 진행되고 있다. 이 중 ABSORB Bio- resorbable Vascular Scaffold(Poly-l-lactide 재질의 에버롤 리무스 약물방출스텐트)에 대한 임상 연구가 활발히 진행되 고 있다. ABSORB Cohort A 관찰연구를21) 통해 세계 최초 로 생체흡수성 약물방출스텐트에 대한 임상 연구가 실시되 었고, 5년 예후관찰 시점에서 Ischemia Driven-MACE 발생 률 3.4%, 사망률 0%, MI 발생률 3.4% 그리고 Ischemia
Driven-TLR 발생률은 0%로 우수한 임상결과를 보고하였 다. 환자 101명에 대해 관찰연구인 ABSORB Cohort B에서22) 2년 예후관찰 시점에서 심혈관 관련 사망률 0%, MI 발생률 3%, Ischemia Driven-TLR 발생률 6%, MACE 발생률 9%
그리고 스텐트 관련 혈전증 발생은 발생하지 않은 것으로 보고하였다. 연구대상 환자수를 1000명까지 확대한 ABSO- RB EXTEND 관찰연구는 6개월 예후관찰 시점에서, 심혈관 관련 사망률 0.4%, 심근경색 발생률 2.6%, Ischemia Driv- en-TLR 발생률 0.4% 그리고 MACE 발생률을 3%로 보고 하고 있다. 이와 같이 ABSORB 생체흡수성 재질의 약물방 출스텐트에 대한 현재까지의 관찰연구 결과는 매우 고무적 이다. 그러나, 최근 유럽에서 발표된 GHOST-EU 레지스트 리에서는23) 6개월 예후관찰시점에서의 스텐트 혈전증 발생 률이 2.1%로 종래의 금속형 약물방출스텐트보다 더 높게 나 타났으며, 이는 기존에 발표된 관찰연구들의 결과와는 매우 상반된 결과를 보고하기도 하였다.
결 론
본 연구는 조타롤리무스 금속형 약물방출스텐트와 에버 롤리무스 생체흡수성 약물방출스텐트 간의 안전성과 효과 성을 비교한 연구이다. 초기 관찰연구들에서 생체흡수성 약 물방출스텐트에 관한 유망한 임상결과들이 보고되고 있으 나, 여타의 관찰연구에서는 기존과 상반되는 임상 결과들이 보고되는 등 생체흡수성 약물방출스텐트에 대한 정확한 치 료효과는 아직까지 불분명하다. 공통대조군 간접비교를 통 한 본 연구에서 에버롤리무스 생체흡수성 약물방출 스텐트 에 대한 안전성과 효과성은 조타롤리무스 금속형 약물방출 스텐트와 유의한 차이를 보이지 않았다. 추가적인 장기간, 대규모의 무작위 비교임상연구가 추가적으로 실시됨으로 인해서 에버롤리무스 생체적합성 약물방출스텐트에 대한 좀 더 정확한 치료 효과 판단이 가능할 것으로 사료된다.
REFERENCES
1) Congdon P. Estimating prevalence of coronary heart disease for small areas using collateral indicators of morbidity. Int J Environ Res Public Health 2010;7:164-177.
2) World Health Organization. Deaths from coronary heart disease.
2004. Available from: http://www.who.int/cardiovascular_diseases/
en/cvd_atlas_14_deathHD.pdf.
3) Agewall S, Henareh L. Quality of life and insulin resistance in pa- tients with coronary heart disease. Coron Artery Dis 2008;19:289- 4) Garg S, Serruys PW. Coronary stents: current status. J Am Coll Car- 292.
diol 2010;56(10 Suppl):S1-S42.
5) Al SJ, Berger PB, Holmes DR Jr. Coronary artery stents. JAMA 2000;284:1828-1836.
6) Moses JW, Leon MB, Popma JJ, Fitzgerald PJ, Holmes DR,
TLR
TVR
Death
MACE
ST
0 0.5 1 1.5 2 2.5
ZES/BVS favor EES favor
Fig. 4. Estimates (odds ratio) of endpoints in the ZES and BVS groups.
ZES BVS
Table 4. Outcome estimates of primary and secondary endpoint at adjusted indirect comparison
Endpoint ZES vs. BVS
OR (95%CI)
p valueTLR 1.92 (0.44, 8.31) 0.61
TVR 2.19 (0.52, 9.14) 0.29
Death 2.70 (0.09, 78.53) 0.75
MACE 2.49 (0.61,10.20) 0.29
O’Shaughnessy C. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N Engl J Med 2003;349:1315-1323.
7) Ullah M, Islam AKMM, Majumder AAS. Bioabsorbable vascular scaffold: a revolution in coronary intervention. Cardiovasc J 2014;6:149-163.
8) Ormiston JA, Webster MW, Armstrong G. First-in-human implanta- tion of a fully bioabsorbable drug-eluting stent: the BVS poly-L-lac- tic acid everolimus-eluting coronary stent. Catheter Cardiovasc In- terv 2007;69:128-131.
9) Brugaletta S, Farooq V, Onuma Y, Diletti R, Windecker S, Thuesen L, et al. Head-to-head comparison of the neointimal response be- tween metallic and bioresorbable everolimus-eluting scaffolds using optical coherence tomography. JACC Cardiovasc Interv 2011;4:1271-1280.
10) Diletti R, Farooq V, Girasis C, Bourantas C, Onuma Y, Heo JH, et al.
Clinical and intravascular imaging outcomes at 1 and 2 years after implantation of absorb everolimus eluting bioresorbable vascular scaffolds in small vessels. Late lumen enlargement: does bioresorp- tion matter with small vessel size? Insight from the ABSORB cohort B trial. Heart 2013;99:98-105.
11) Ormiston JA, Serruys PW, Regar E, Dudek D, Thuesen L, Webster MW, et al. Abioabsorbable everolimus-eluting coronary stent system for patients with single de-novo coronary artery lesions (ABSORB):
a prospective open-label trial. The Lancet 2008:371:899-907.
12) Serruys PW, Ormiston JA, Onuma Y, Regar E, Gonzalo N, Garcia- Garcia HM, et al. A bioabsorbable everolimus-eluting coronary stent system (ABSORB): 2-year outcomes and results from multiple im- aging methods. Lancet 2009;373:897-910.
13) Bucher HC, Guyatt GH, Griffith LE, Walter SD. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. Journal of Clinical Epidemiology 1997;50:683-691.
14) Higgins, Julian PT. Cochrane handbook for systematic reviews of in- terventions. Vol. 5. Chichester: Wiley-Blackwell;2008.
15) von Birgelen C, Sen H, Lam MK, Danse PW, Jessurun G, Hautvast R, et al. Third-generation zotarolimus-eluting and everolimus-eluting stents in all-comer patients requiring a percutaneous coronary inter- vention (DUTCH PEERS): a randomised, single-blind, multicentre, non-inferiority trial. The Lancet 2014;383:413-423.
16) Cho SC, Jeong MH, Kim W, Ahn YK, Hong YJ, Kim YJ, et al. Clini-
cal outcomes of everolimus-and zotarolimus-eluting stents in patients with acute myocardial infarction for small coronary artery disease.
Journal of Cardiology 2014;63:409-417.
17) von Birgelen C, Basalus M, Tandjung K, van Houwelingen K, Stoel M, Louwerenburg J, et al. A Randomized Controlled Trial in Second- Generation Zotarolimus-Eluting Resolute Stents Versus Everolimus- Eluting Xience V Stents in Real-World Patients. The TWENTE Trial.
Journal of the American College of Cardiology 2012;59:1350-1361.
18) Serruys PW, Silber S, Garg S, van Geuns RJ, Richardt G, Buszman PE, et al. Comparison of zotarolimus-eluting and everolimus-eluting coronary stents. New England Journal of Medicine 2010;363:136- 19) Mehilli J, Richardt G, Valgimigli M, Schulz S, Singh A, Abdel-Wa- 146.
hab M, et al. Zotarolimus-versus Everolimus-eluting stents for un- protected left main coronary artery disease. Journal of the American College of Cardiology 2013;62:2075-2082.
20) Costopoulos C, Latib A, Naganuma T, Miyazaki T, Sato K, Figini F, et al. Comparison of early clinical outcomes between ABSORB bio- resorbable vascular scaffold and everolimus-eluting stent implanta- tion in a real-world population. Catheterization and Cardiovascular Interventions 2014.
21) Onuma Y, Dudek D, Thuesen L, Webster M, Nieman K, Garcia-Gar- cia HM, et al. Five-year clinicaland functional multislice computed tomography angiographic results after coronary implantation of the fully resorbable polymeric everolimus-eluting scaffold in patients with de novo coronary artery disease. The ABSORB Cohort A Trial.
J Am Coll Cardiol Intv 2013;6:999-1009.
22) Serruys PW, Onuma Y, Dudek D, Smits PC, Koolen J, Chevalier B.
Evaluation of the second generation of a bioresorbable everolimus- eluting vascular scaffold for the treatment of de novo coronary artery stenosis: 12-month clinical and imaging outcomes. J Am Coll Cardi- ol 2011;58:1578-1588.
23) Capodanno D, Gori T, Nef H, Latib A, Mehilli J, Lesiak M, et al.
Percutaneous coronary intervention with everolimus-eluting biore-
sorbable vascular scaffolds in routine clinical practice: early and
midterm outcomes from the European multicentre GHOST-EU reg-
istry. EuroIntervention: journal of EuroPCR in collaboration with the
Working Group on Interventional Cardiology of the European Soci-
ety of Cardiology 2014.
Appendix 1. PubMed search strategy and result
Item No. Search term Results
Patient #1 “Coronary artery disease” [MeSH Terms] 179,414
#2 “CAD [tiab]” 23,005
P #3 #1 or #2 190,347
Intervention &
comparison
#4 “zotarolimus eluting stent” or “zotarolimus eluted stent” or “zotarolimus coating stent”
or “zotarolimus coated stent” or “endeavor” or “resolute” or “resolute integrity”
4,241
#5 “everolimus eluting stent” or “everolimus eluted stent” or “everolimus coating stent” or “everolimus coated stent” or “xience” or “xience prime” or “xience v”
420
#6 “bioabsorbable vascular scaffold” or “bioresorbable vascular scaffold” or “biodegradable vascular scaffold” or “absorb”
6,430
#7 #4 or #5 or #6 10,966
I & C #8 #3 and #7 449
#9 Humans [Filter] 13,175,484
PubMed #10 #8 and #9 432
Search date: 2014.05.12 (http://www.ncbi.nlm.nih.gov/pubmed)
▒ 부 록 ▒