-110-
Subjective and Objective Results of Radiofrequency Ablation in Drug-Resistant Allergic Rhinitis Based on a
12-Month Follow-up Study
Seon-Sook Han, MD1, Seung-Joon Lee, MD1, Jun Yeon Won, MD2, Hyun Kyung Choi2 and Eui-Cheol Nam, MD2
1Department of Internal Medicine, Kangwon National University School of Medicine;
2Otolaryngology, Kangwon National University Hospital, Chuncheon, Korea
ABSTRACT
Background and Objectives:Allergic rhinitis is a common condition that has been treated using various methods. Never- theless, it remains an intractable condition in some cases. We evaluated the long-term efficacy of radiofrequency ablation (RFA) therapy for drug-resistant allergic rhinitis. Materials and Methods:Eighteen patients with allergic rhinitis were enrolled in this prospective interventional study. Their subjective symptoms and objective findings were assessed using a visual analogue scale and acoustic rhinometry before and after RFA therapy. Postoperative follow-up was carried out at 1, 3, 6, and 12 months.
Results:Nasal obstruction and rhinorrhea were improved significantly (p<0.001 and p=0.015, respectively), and these effects continued for 12 months after RFA therapy. However, the effects on nasal itching and sneezing did not last throughout the year of the study. Patients’ overall satisfaction scores declined at 12 months. On acoustic rhinometry, the minimal cross-sectional area and the total nasal volume did not show improvement, and there were no correlations with the subjective symptoms. Most of the com- plications associated with the RFA procedure were minimal and resolved within 4 weeks. Conclusion:RFA is a safe, simple, and effective procedure for relieving nasal obstruction and rhinorrhea for at least 12 months in drug-resistant allergic rhinitis.
KEY WORDS:Allergic rhinitis·Radiofrequency·Long-term effects.
INTRODUCTION
Allergic rhinitis is a common and troublesome condition, affecting 10-40% of the population worldwide.1-3) Aller- gic rhinitis is clinically defined as a symptomatic disorder of the nose that is induced by IgE-mediated inflammation of the nasal membranes after allergen exposure.3) Most pa- tients with allergic rhinitis have been treated with conven- tional pharmacotherapy such as antihistamines, deconges- tants, anticholinergic agents, mast cell stabilizers, intranas- al steroid spray, leukotriene modifiers, and allergen desen- sitization.4)5) Despite these medical treatments, allergic rhi- nitis remains an intractable condition in some patients. Sur-
gical solutions such as conventional submucosal inferior turbinate resection, argon plasma and other laser surgeries, and radiofrequency ablation (RFA) have been considered in such cases.6-10) However, there is debate regarding the choice of a surgical modality with regard to its clinical ef- fectiveness and long-term benefits.6-8)11)12) Generally, sub- mucosal turbinate resection is associated with additional mucosal and bony damage and increased risk for bleeding, as well as possible discomfort and pain for 1-2 days owing to nasal packing.7) It was recently suggested that laser irra- diation of the mucosa may not cause excessive damage and bleeding, although it caused increased mucosal loss and bony exposure,11)12) and produced more damage to the mu- cociliary function of the turbinate compared with RFA ther- apy.12)13)
RFA therapy has been introduced as superior to other surgical modalities for the reduction of hypertrophied in- ferior turbinate volume13-16) and as a safer and less destruc- tive procedure in comparison with other methods.13)14)17)18)
However, there have been few studies of the efficacy of Address correspondences and reprint requests to Eui-Cheol Nam,
M.D., Department of Otolaryngology, School of Medicine, Kangwon National University, 17-1 Hyoja-2-dong, Chuncheon 200-701, Korea
Tel:82-33-258-2311, Fax:82-33-255-8809 E-mail:[email protected]
Received for publication on December 3, 2008 Accepted for publication on February 18, 2009
RFA therapy against allergic rhinitis.10) Moreover, only limited studies have assessed with objective quantifica- tion of improvements in nasal patency after RFA therapy in drug-resistant allergic rhinitis. Therefore, we carried out a prospective, longitudinal, interventional study to evaluate the efficacy and safety of RFA therapy in drug-resistant allergic rhinitis. Over a period of 12 months after RFA on both inferior turbinates, we performed symptomatic eval- uation using a visual analogue scale (VAS), investigated the incidence and duration of postoperative complications, and measured nasal patency by acoustic rhinometry.
METHODS Patients
Eighteen patients with drug-resistant allergic rhinitis were prospectively enrolled in this study between 1 May 2003 and 1 June 2004 and were followed for 12 months.
Allergic rhinitis was defined as a positive result for a skin prick allergen presentation test and the presence of nasal symptoms of sneezing, rhinorrhea, nasal obstruction, and itching.19-21) Those symptoms had persisted after medical therapy for at least a month, such as antihistamine, decon- gestants, and intranasal steroid spray. Patients with history of previous nasal surgery were excluded from the study.
The subjects’ mean age was 35±11 years (range, 13- 51 years). Among the 18 patients included in the study, 10 were men (56%). Evaluations were made preoperatively and at 1, 3, 6, and 12 months after the RFA procedure. We instructed the enrolled patients not to take any anti-allergic medication during the study period without notice. All pa- tients were given written informed consent to participate in this study.
Symptom evaluation
A standard VAS ranging from 0 (no symptoms) to 10 (most severe) was used to assess four subjective symp- toms:sneezing, rhinorrhea, nasal obstruction, and nasal itching. Patients’ overall postoperative satisfaction was also graded on a VAS ranging from 0 (complete dissatisfaction) to 10 (complete satisfaction). We also examined postop- erative complications and their durations.
Acoustic rhinometry
At the visits for symptomatic evaluation, acoustic rhi- nometry (E. Benson Hood Laboratories, Pembroke, MA, USA) was performed by the same experienced technician, with the subjects in the sitting position. The two narrowest
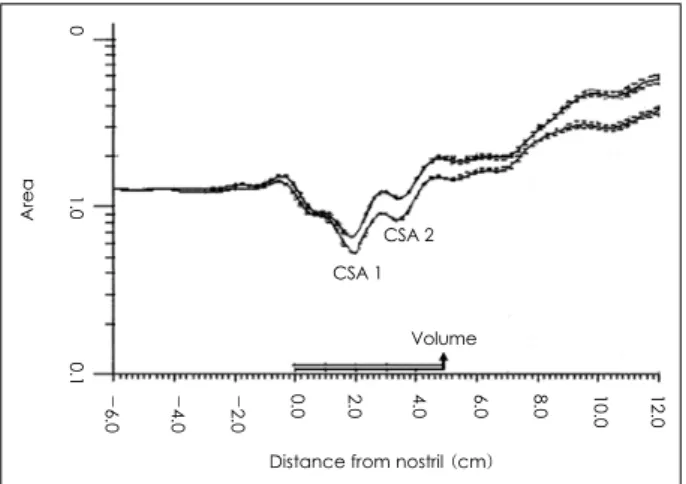
areas in both nasal cavities were determined as minimal cross-sectional areas (CSA1, 2), and the volume at 5 cm posterior from the nostril was measured (Fig. 1). CSA 1 and 2 were identified at approximately 2 and 4 cm from the nostril, respectively,22-24) representing the nasal valve (I-notch or the isthmus nasi) and the anterior end of the in- ferior turbinate (C-notch or the head of inferior turbi- nate).25)26)
Surgical procedure
The surgical procedure was similar to that in common use,10)27)28) and the same surgeon (the corresponding au- thor) performed all the procedures under topical anaesthe- sia, consisting of 10% lidocaine spray and 2% lidocaine infiltration into the anterior and mid-portions of each in- ferior turbinate. Under adequate anaesthesia, radiofre- quency energy at a frequency of 465 Hz was delivered by the RF generator (ENTec Coblator Plasma Surgery Sys- tem;Arthrocare, Sunnyvale, CA, USA) using a Reflex ultra 45 turbinate handpiece. The needle electrode, 1 mm in diameter, was placed submucosally into three or four points within the anterior and mid-portions of each inferior turbinate, with visualization using a nasal endoscope with an angle of 30°and diameter of 4 mm. A coblation power level of 5 was used, and the wand was kept in position for about 10-12 seconds. After completion of the procedure, cotton pledgets soaked with a mixture of 4% lidocaine and 0.1% epinephrine (99:1) were temporarily placed in both nasal cavities for 3-5 min to prevent bleeding. The total duration of the procedure was 10-15 min, and the patients were discharged from our clinic within 30 min af- ter the procedure.
Area 0 1.0 0.1 12.010.08.0 6.0 4.0 2.0 0.0 - 2.
0- 4.
0- 6.
0
Distance from nostril (cm) Volume CSA 1
CSA 2
Fig. 1. Sample acoustic rhinometry graph. The first valley is CSA 1, and the second valley is CSA 2. Total nasal volume was calcu- lated from the nostril to a depth of 5 cm.
Statistics
The results are presented as means±standard deviation (SD) or medians (interquartile range). The 12-month ef- fects of RFA on symptoms and acoustic rhinometry were analyzed using Friedman’s repeated measures analysis.
The correlations between subjective symptoms and acous- tic rhinometric results were analyzed using Spearman’s test.
All statistical analyses were performed using SPSS version 12.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
All 18 patients were followed until 1 month after RFA, with 17 and 15 patients followed until 6 and 12 months, re- spectively. Acoustic rhinometry was skipped in five pa- tients at 12 months, but their subjective results were in- cluded in this study.
The median duration of disease was 6 years (range, 0-20 years), and five patients had a disease duration of
≤1 year. The most common motive for surgery was a poor quality of life attributable to allergic rhinitis, despite medi- cal therapy (15 patients, 83%) that included antihistamines, decongestants, and intranasal steroid sprays. All patients tolerated the RFA procedure well, and no problem was encountered. No significant postoperative bleeding was reported. On follow-up anterior rhinoscopy, postoperative crust formation was the most commonly observed side ef- fect (14 patients, 78%) for up to 2 weeks after surgery.
Four patients complained of mild nasal pain and discom- fort after surgery (22%), but this did not last until the 4- week follow-up examination and did not require analgesics or unscheduled visits.
Subjective symptoms
Throughout the 12 months of follow-up, Friedman’s re- peated measures analysis indicated that the VAS scores of rhinorrhea (p=0.015) and nasal obstruction (p<0.001) were decreased significantly (Table 1). However, sneezing and itching did not show significant improvement.
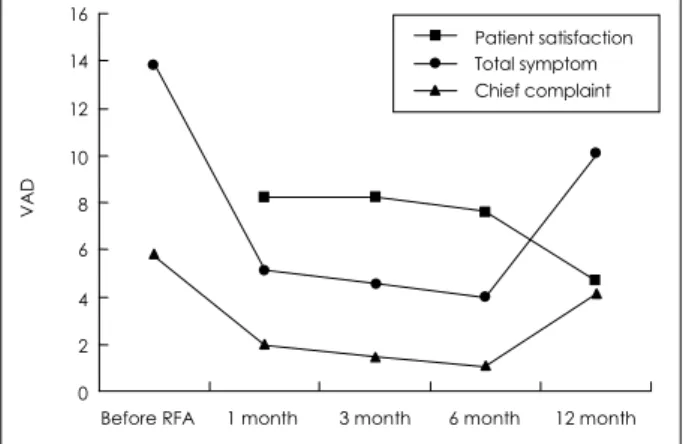
We also investigated changes in the scores for overall satisfaction, chief complaints, and total symptoms. The pa- tients’ overall satisfaction remained essentially constant until 6 months after RAF therapy (mean VAS scores±
SD:8.2±1.4 at 1 month, 8.2±2.2 at 3 months, and 7.6±
2.2 at 6 months) but showed a significant decrease at 12 months (4.7±2.8) compared with the first month (p<
0.05, Wilcoxon’s signed-rank test;Fig. 2). Chief com-
Table 1. Results of symptom and acoustic rhinometry before and after radiofrequency ablation
Before RFA 1 month 3 months 6 months 12 months
VAS scores of symptoms
n=18 n=18 n=17 n=18 n=15
Sneezing 2.0±2.6 1.4±2.4 1.0±1.7 1.5±2.8 2.7±3.8 Rhinorrhea* 3.6±3.0 1.4±1.9 1.5±2.4 1.5±2.2 3.0±3.7
Nasal itching 2.1±2.9 0.7±1.4 0.9±1.9 0±0 1.0±2.1
Nasal obstruction† 6.2±2.8 1.5±1.2 1.2±2.2 1.0±1.4 3.4±2.6
Acoustic rhinometry results
n=18 n=18 n=17 n=13 n=10
CSA 1 (cm2) 0.6±0.2 0.7±0.1 0.6±0.1 0.7±0.2 0.6±0.2
CSA 2 (cm2) 1.2±0.4 1.4±0.4 1.5±0.6 1.5±0.4 1.1±0.2
Volume (cm3) 6.6±1.7 7.4±1.3 7.5±1.7 7.9±1.5 6.3±1.3
*:p<0.05 by Friedman’s repeated measures analysis, †:p<0.001 by Friedman’s repeated measures analysis. Data are presented as means±SD. Acoustic rhinometric data are the mean values for both nasal cavities. VAS:visual analogue scale, CSA:cross-sec- tional area
VAD
16 14 12 10 8 6 4 2 0
Before RFA 1 month 3 month 6 month 12 month Fig. 2. Postoperative patient satisfaction. Patient satisfaction re- mained unchanged for 6 months after RFA. After 12 months, the mean patient satisfaction score was decreased compared with the first-month score (p<0.05, Wilcoxon’s signed-rank test). VAS scores of total symptoms and chief complaint showed signifi- cant improvements (both p<0.001, Friedman’s repeated measures analysis). Visual analogue scale (VAS):0, complete dissatisfac- tion;10, complete satisfaction.
Patient satisfaction Total symptom Chief complaint
plaints were nasal obstruction in 11 patients (61%), rhi- norrhea in four (22%), and sneezing in three (17%);
none had nasal itching as the chief complaint. The mean VAS scores of the chief complaints were 5.8±3.1 before RFA, 2.0±2.4 at 1 month, 1.5±2.1 at 3 months, 1.1±
1.3 at 6 months, and 4.1±3.3 at 12 months. The total symptom score was defined as the sum of the scores of the four symptoms. The mean total symptom scores were 13.8±7.6 before RFA, 5.1±4.7 at 1 month, 4.5±6.3 at 3 months, 4.0±4.3 at 6 months, and 10.1±8.6 at 12 months.
Friedman’s repeated measures analysis indicated that the chief complaint (p<0.001) and total symptom scores (p<
0.001) decreased significantly over the 12-month follow- up period (Fig. 2).
Acoustic rhinometry
The results of acoustic rhinometry are presented as the mean scores of both nasal cavities. After RFA, no signifi- cant improvements were observed in the acoustic rhino- metry results over the 12-month study period, according to Friedman’s repeated measures analysis (Table 1). Further- more, no correlations were observed between any subjec- tive symptoms and the acoustic rhinometry measurements (Spearman’s test, data not shown).
Additional follow-up
We performed additional follow-up by telephone inter- view after 4-5 years. Among the 18 patients, 17 replied to the interview.
Given that ‘relapse’ was considered as same or more aggressive symptoms compared to pre-RFA period, nine (53%) out of 17 had a relapse:the symptoms were same in eight (47%) and more aggressive in a patient. Eight pa- tients (47%) expressed overall, satisfaction with the effect of RFA even after 4 or 5 years;the symptoms were reduc- ed in two (12%), and no symptom in six (35%). Among the patients with relapse, four (36%) stated that they would consider RFA therapy again.
DISCUSSION
Since its application for reduction of tongue volume in a porcine model with obstructive sleep apnea syndrome,29) RFA therapy has been widely applied in various upper air- way disorders. The effects of RFA on hypertrophied infer- ior turbinates have recently been reported, and the safety and efficacy of RFA have been suggested.14)15)17)28)30)31)
Volume reduction by RFA is mediated by fibrosis, with wound contraction in the inferior turbinates.2) The fibro- blastic response begins 1 week after RFA, and the healing process with contraction occurs from 2 to 4 weeks after RFA.
In allergic rhinitis, nasal obstruction may be caused by increased blood supply and tissue edema of the nasal mu- cosa. Dilated venous sinuses in the inferior turbinate would restrict airflow, especially at the narrowest area between the inferior turbinate and nasal septum.32) We suggest that coagulation and subsequent blockage of the sinuses by RAF at the anterior portion of the turbinate may induce re- lief of nasal obstruction in allergic rhinitis. In the present study, we confirmed that the volume reduction effect ap- peared at the first month and continued until 12 months (p<0.001).
Nasal mucosal goblet cells, nasal submucosal glands, and permeability changes in nasal submucosal blood vessels participate and contribute to the production of rhinorrhea.32) The density of goblet cells in the upper airway is highest at the inferior turbinate. We postulated that RFA may reduce the number of glands and consequently rhinorrhea.
However, no improvements were observed in itching and sneezing. Stimulation of the sensory nerves in the nasal mucosa plays an important role in itching,2)33) and sneezing is a protective neural reflex involved in expelling irritants forcefully and rapidly. Histological examination of the tis- sue response to RFA has indicated no evidence of extra- lesional neural damage, and viable neural structures have been found in newly formed fibrous structures, even in the early stage after RFA.29) In the present study, pre-RFA scores of itching and sneezing were much lower than those of nasal obstruction and rhinorrhea (Table 1). Neural sur- vival and low initial symptom scores may explain why the effects of RFA on itching and sneezing were less obvious and temporary in the present study.
Acoustic rhinometry, which applies audible reflected sound waves into the nasal cavity and produces a plot of the area-distance relationship26) (Fig. 1), is commonly used for objectively evaluating nasal obstruction.23)25)26) Although its reproducibility is more favourable than that of other cli- nical tests,26)34) acoustic rhinometry has not given consis- tent results for measuring the volume-reduction effect of RFA in previous studies.15)17)27) In addition, it has not been applied previously in studies of allergic rhinitis. Our results indicated a tendency toward the widening of CSA 2 and total nasal volume, but these effects were not statistically significant.
Moreover, the acoustic rhinometric results were not cor-
related with the subjective assessment of nasal obstruction before and after RFA, corresponding to the results of other studies regarding the clinical implications of acoustic rhi- nometry.27)28)35)36) We presume that the subjective feeling of nasal obstruction may involve subtle and complex mecha- nisms which the rhinometry could not effectively demon- strate,35)37) or the limited number of subjects included in this study might have restricted the investigation.
In additional follow up after 4-5 years, nine (53%) had a relapse. However, this result was obtained by not visual anolgue scale but telephone interview after a long time, so it is insufficient to conclude. Therefore we analyzed the result of 12 months follow up and suggest the effect of RFA in drug-resistant allergic rhinitis sustains for at least 12 months.
Based on our clinical experience, we believe that RFA of the anterior part of the inferior turbinate is a safe procedure and does not cause serious bleeding or mucosal damage;
only transient mild pain and crust formation were observed.
RFA may be superior to laser methods in that the major nasal epithelial function, mucociliary clearance, could be preserved.17)27)38)
In conclusion, the results of the present study demon- strate that RFA is a safe and effective procedure for re- lieving nasal obstruction and rhinorrhea for at least 12 months in drug-resistant allergic rhinitis.
REFERENCES
1) Bellanti JA, Wallerstedt DB. Allergic rhinitis update: epidemiology and natural history. Allergy Asthma Proc 2000;21:367-70.
2) Skoner DP. Allergic rhinitis: definition, epidemiology, pathophysiolo- gy, detection, and diagnosis. J Allergy Clin Immunol 2001;108:S2-8.
3) Bachert C, van Cauwenberge P, Khaltaev N. Allergic rhinitis and its impact on asthma. In collaboration with the World Health Organiza- tion. Executive summary of the workshop report. 7-10 December 1999, Geneva, Switzerland. Allergy 2002;57:841-55.
4) Seth D, Secord E, Kamat D. Allergic rhinitis. Clin Pediatr (Phila) 2007;46:401-7.
5) Mahr TA. Therapy in allergic rhinoconjunctivitis: new horizons. Al- lergy Asthma Proc 2007;28:404-9.
6) Mori S, Fujieda S, Yamada T, Kimura Y, Takahashi N, Saito H. Long- term effect of submucous turbinectomy in patients with perennial allergic rhinitis. Laryngoscope 2002;112:865-9.
7) Ogawa T, Takeno S, Ishino T, Hirakawa K. Submucous turbinectomy combined with posterior nasal neurectomy in the management of se- vere allergic rhinitis: clinical outcomes and local cytokine changes.
Auris Nasus Larynx 2007;34:319-26.
8) Fukazawa K, Ogasawara H, Tomofuji S, Fujii M, Sakagami M. Ar- gon Plasma Surgery for the inferior turbinate of patients with peren- nial nasal allergy. Laryngoscope 2001;111:147-52.
9) Imamura SI. Carbon dioxide laser vaporization of the inferior turbi- nate for allergic rhinitis: short-term results. Ann Otol Rhinol Laryngol 2003;112:1043-9.
10) Lin CH, Lin PW, Su CY, Chang HW. Radiofrequency for the treat-
ment of allergic rhinitis refractory to medical therapy. Laryngoscope 2003;113:673-8.
11) Clement WA, White PS. Trends in turbinate surgery literature: a 35- year review. Clin Otolaryngol Allied Sci 2001;26:124-8.
12) Chang CW, Ries WR. Surgical treatment of the inferior turbinate: new techniques. Curr Opin Otolaryngol Head Neck Surg 2004;12:53-7.
13) Sapi T, Sahin B, Karavus A, Akbulut UG. Comparison of the effect of radiofrequency tissue ablation, CO2 laser ablation, and partial turbin- ectomy applications on nasal mucociliary functions. Laryngoscope 2003;113:514-9.
14) Cavaliere M, Mottola G, Iemma M. Comparison of the effectiveness and safety of radiofrequency turbinoplasty and traditional surgical technique in treatment of inferior turbinate hypertrophy. Otolaryngol Head Neck Surg 2005;133:972-8.
15) Cavaliere M, Mottola G, Iemma M. Monopolar and bipolar radio- frequency thermal ablation of inferior turbinates: 20-month follow-up.
Otolaryngol Head Neck Surg 2007;137:256-63.
16) Harrill WC, Pillsbury HC 3rd, McGuirt WF, Stewart MG. Radiofre- quency turbinate reduction: a NOSE evaluation. Laryngoscope 2007;
117:1912-9.
17) Coste A, Yona L, Blumen M, Louis B, Zerah F, Rugina M, et al. Ra- diofrequency is a safe and effective treatment of turbinate hypertro- phy. Laryngoscope 2001;111:894-9.
18) Kezirian E, Powell NB, Riley RW, Hester JE. Incidence of compli- cations in radiofrequency treatment of the upper airway. Laryngos- cope 2005;115:1298-304.
19) Long A, McFadden C, Devine D, Chew P, Kupelnick B, Lau J. Man- agement of allergic rhinitis and nonallergic rhinitis. Evid Rep Technol Assess (Summ) 2002;54:1-6.
20) Gendo K, Larson EB. Evidence-based diagnostic strategies for eval- uating suspected allergic rhinitis. Ann Intern Med 2004;140:278-89.
21) Quillen DM, Feller DB. Diagnosing rhinitis: allergic vs. nonallergic.
Am Fam Physician 2006;73:1583-90.
22) Corey JP, Nalbone VP, Ng BA. Anatomic correlates of Acoustic rhi- nometry as measured by rigid nasal endoscopy. Otolaryngol Head Neck Surg 1999;121:572-6.
23) Mamikoglu B, Houser SM, Corey JP. An interpretation method for objective assessment of nasal congestion with acoustic rhinometry.
Laryngoscope 2002;112:926-9.
24) Cakmak O, Coskun M, Celik H, Buyuklu F, Ozluoglu LN. Value of acoustic rhinometry for measuring nasal valve area. Laryngoscope 2003;113:295-302.
25) Clement PAR, Gordts F. Consensus report on acoustic rhinometry and rhinomanometry. Rhinology 2005;43:169-79.
26) Corey JP. Acoustic rhinometry: should we be using it? Curr Opin Otolaryngol Head Neck Surg 2006;14:29-34.
27) Back LJ, Hytontn ML, Ylikoski JS. Submucosal bipolar radiofre- quency thermal ablation of inferior turbinates: a long-term follow up with subjective and objective assessment. Laryngoscope 2002;112:
1806-12.
28) Seeger J, Zenev E, Gundlach P. Stein T, Muller G. Bipolar radiofre- quency-induced thermoplasty of turbinate hypertrophy: pilot study and 20 months’ follow up. Laryngoscope 2003;113:130-5.
29) Powell NB, Riley RW, Troell RJ, Blumen MB, Guilleminault C.
Radiofrequency volumetric reduction of the tongue. A porcine pilot study for the treatment of obstructive sleep apnea syndrome. Chest 1997;111:1348-55.
30) Nease CJ, Krempl GA. Radiofrequency treatment of turbinate hyper- trophy: a randomized, blinded, placebo-controlled trial. Otolaryngol Head Neck Surg 2004;130:291-9.
31) Porter MW, Hales NW, Nease CJ, Krempl GA. Long-term results of inferior turbinate hypertrophy with radiofrequency treatment: a new standard care? Laryngoscope 2006;116:554-7.
32) Broide DH. The pathophysiology of allergic rhinoconjunctivitis. Al-
lergy Asthma Proc 2007;28:398-403.
33) Hansen I, Klimek L, Mosges R, Hormann K. Mediators of inflamma- tion in the early and the late phase of allergic rhinitis. Curr Opin Al- lergy Clin Immunol 2004;4:159-63.
34) Silkoff PE, Chakravorty S, Chapnik J, Cole P, Zamel N. Reproduci- bility of acoustic rhinometry and rhinomanometry in normal sub- jects. Am J Rhinol 1999;13:131-5.
35) Tomkinson A, Eccles R. Comparison of the relative abilities of acous- tic rhinometry, rhinomanometry, and the visual analogue scale in de- tecting changes in the nasal cavity in a healthy adult population. Am
J Rhinol 1996;10:161-5.
36) Lane AP, Zweiman B, Lanza DC, Swift D, Doty R, Dhong HJ, et al.
Acoustic rhinometry in the study of the acute nasal allergic response.
Ann Otol Rhinol Laryngol 1996;105:811-8.
37) Hanif J, Jawad SS, Eccles R. The nasal cycle in health and disease.
Clin Otolaryngol Allied Sci 2000;25:461-7.
38) Rhee CS, Kim DY, Won TB, Lee HJ, Park SW, Kwon TY, et al.
Changes of nasal function after temperature-controlled radiofrequency tissue volume reduction for turbinate. Laryngoscope 2001;111:153-8.