서 론
우리나라 통계청 자료에 따르면 2012년 고령인구의 비율은 11.8%
로 나타났으며, 매년 고령인구의 비율은 증가할 것으로 예상되어 2030년에는 24.3%, 2050년에는 37.4%에 이를 것이라고 보고 있다.1) 많 은 노인들은 질병에 걸리지 않더라도 노화에 따른 신체기능의 저하 로 인해 신체적, 정신적, 사회적 장애를 동반하는 문제가 유발된다.2-4) 노령화에 따라 가장 보편적인 신체변화는 근골격계의 약화이며,
그 결과 골다공증 및 골절 위험 등이 증가한다. 근골격계의 약화를 대표하는 근감소증은 근력의 저하로 인해 각종 신체기능의 감소 및 장애를 유발하며, 이러한 근력의 저하는 당뇨병, 심혈관질환 등 만성 질환자에서 더 크다는 보고가 있다.5) 그러나 노화에 따르는 근육량 감소에 대한 생리 현상에 대해서는 아직 의학적으로 주목 받지 못하 고 있다. 근감소증에 대한 연구는 아직 미미하지만 현실적으로 지출 되는 사회적 비용이 미국에서 2000년 기준으로 185억 달러에 이르 고 있어 이에 대한 이해와 대책이 매우 필요한 상황이다.6)
The Association between Sarcopenia and the Osteoporosis in Korean Men and Women Aged Older than 60 Years
Jae-Hyeok Ro1, Yong Soon Park1,*, Jeong-Hyeon Kim1, See-Won Kim2
1Department of Family Medicine, Hallym University Chuncheon Sacred Heart Hospital, Chuncheon; 2Department of Family Medicine, Hallym University Sacred Heart Hospital, Anyang, Korea
Background: The objective of this study was to explore the association between sarcopenia and osteoporosis in a representative sample of elderly Korean men and women.
Methods: This study was based on data acquired in the Fifth Korean National Health and Nutrition Survey (KNHANES) conducted in 2010. We assessed 1,728 Korean men and women aged above 60 years (765 men, 963 women). Bone mineral density (BMD) and body composition were measured by dual-energy X-ray absorptiometry. Multiple linear regression analyses were performed to assess the relationship between BMD of the lumbar spine, total hip, and femur neck and various parameters. Logistic regression analyses were performed to explore the association between the skeletal muscle index and osteoporosis.
Results: The results showed a significant correlation between total fat mass, skeletal muscle index, and total hip, femur neck, and lumbar spine BMD.
The multiple linear regression analyses of all subjects showed that skeletal muscle index, as an independent variable, was a significant determinant of BMD. In the logistic regression analyses, osteoporosis prevalence decreased by 0.610 fold in men (95% confidence interval [CI], 0.416–0.894) and by 0.650 fold in women (95% CI, 0.467–0.905), with a 1 kg/m2 increase in the skeletal muscle index.
Conclusion: This study suggests that in Korean men and women over 60 years old, skeletal muscle index has a positive correlation with BMD and a decreased risk of osteoporosis.
Keywords: Sarcopenia; Osteoporosis; Skeletal Muscle Index; KNHANES
Received July 1, 2016 Revised September 29, 2016 Accepted October 2, 2016
Corresponding author Yong Soon Park Tel: +82-33-240-5311, Fax: +82-33-240-5440 E-mail: [email protected]
Copyright © 2017 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
한국 60세 이상 남녀의 근감소와 골다공증과의 연관성
노재혁
1, 박용순
1,*, 김정현
1, 김시원
21한림대학교 춘천성심병원 가정의학과, 2한림대학교 성심병원 가정의학과
Original Article
https://doi.org/10.21215/kjfp.2017.7.4.477 eISSN 2233-9116
Korean J Fam Pract. 2017;7(4):477-482
Korean Journal of Family Practice
KJFP
Jae-Hyeok Ro, et al. Sarcopenia and Osteoporosis in Aged Older than 60 Years
Korean Journal of Family Practice
KJFP
근감소증의 정의는 나이가 증가함에 따라 동반되는 근육의 양과 동시에 근력의 감소로 정의되고 있으나 표준화된 진단기준은 없다.
최초 Baumgartner 등7)이 근감소증 진단기준을 제시한 이후, 다양한 연구가 이루어지고 있다. 지금까지 골밀도와 근육량에 관한 많은 연 구들이 이루어졌고,8-10) 이 연구들은 낮은 근육량과 낮은 골밀도간 의 상관성을 보여주었다. 이에 본 연구에서는 60세 이상 남녀간 근육 량 감소에 따른 골다공증의 관련성에 대해 알아보고자 하였다.
방 법
1. 연구 대상자
본 연구는 2010년에 시행된 제5기 1차연도 국민건강영양조사 자 료를 이용하였다. 국민건강영양조사는 국민의 전반적인 건강 및 영 양 상태와 보건의식행태를 파악하는 기초 통계를 산출하고자 표본 인구를 대상으로 1998년부터 시행되고 있다. 이 조사는 건강설문 조 사와 영양조사, 검진조사로 구성되어 있다. 제5기 자료는 3단계 층화 집락 표본추출방법을 사용하였으며, 1차 추출단위는 동, 읍, 면, 2차 추출단위는 조사구, 3차 추출단위는 가구로 하여 조사가 진행되었 다.
60세 이상 참여자 2,028명(남자 907명, 여자 1,121명) 중 골밀도 검 사를 측정하지 않았거나 근육량 지수 데이터가 없는 자(남자 142명, 여자 158명)를 제외한 1,728명(남자 765명, 여자 963명)을 최종 분석 대상자로 하였다.
2. 신체계측 및 변수 측정
본 연구에서는 사회 인구학적 특성, 만성질환 유병 상태, 약물복 용, 신체계측과 혈액검사 자료를 이용하였다. 신체계측 변수는 신장 과 체중을 사용하였다. 신장 측정은 신장계(SECA 225; SECA Deutschland, Hamburg, Germany)로 소수점 이하 첫째 자리(0.1 cm)까 지 측정하였고, 체중은 체중계(GL-6000-20; CASKOREA, Seoul, Ko- rea)로 소수점 이하 첫째 자리(0.1 kg)까지 측정하였다.
혈액검사는 최소 8시간 이상 공복 후 시행되었으며, 혈중 25-hy- droxyvitamin D (25[OH]D)는 방사면역측정법으로 측정하였고 장비 는 1470 WIZARD gamma-counter (PerkinElmer, Truku, Finland), 시약 은 25(OH)D 125I RIA KIT (DiaSorin Inc., Stillwater, MN, USA)를 이용 하였다.
설문지를 이용하여 흡연 및 음주습관, 신체활동 유무를 조사하 였다. 흡연상태는 평생 담배를 피운 적이 없는 사람, 과거에는 담배 를 피웠으나 현재에는 피우지 않는 사람, 현재 담배를 피우는 사람으 로 나누었다. 신체활동 유무는 격렬한 신체활동(달리기, 등산, 빠른
속도로 자전거 타기, 빠른 수영, 축구, 농구, 줄넘기, 스쿼시, 단식테니 스, 무거운 물건 나르기 등의 직업활동 및 체육활동)을 1회 20분 이 상, 주 3일 이상 하거나, 중등도 신체활동(천천히 하는 수영, 복식테니 스, 배구, 배드민턴, 탁구, 가벼운 물건 나르기 등의 직업활동 및 체육 활동, 걷기는 제외)을 1회 30분 이상, 주 5일 이상 하는 경우로 정하였 다.
3. 골밀도 측정과 골다공증의 정의
골밀도는 이중에너지 X-선 흡수방법(dual-energy X-ray absorpti- ometry)에 의한 X-선 골밀도 측정기(DISCOVERY-W fan-beam densi- tometer; Hologic Inc., Bedford, MA, USA)를 사용하여 측정한 대퇴부 전체(total femur), 대퇴 경부(femur neck), 요추(lumbar spine) 골밀도의 T-score를 이용하였다. T-score는 골절에 대한 절대적 위험도를 나타 내는 것으로 골질량이 가장 높은 젊은 연령층의 골밀도와 비교한 값 이다. 세계보건기구(World Health Organization)의 가이드라인에 따 라 T-score가 -2.5 표준편차 이하인 경우를 골다공증(osteoporosis)으 로 분류하였다.11)
4. 사지 근육량 및 근육량지수의 정의
본 연구에서 사지근육량(appendicular skeletal muscle mass, ASM) 은 이중에너지 X-선 흡수방법으로 측정한 양측 상하지 근육량의 합 으로 정의하였고, 이 값을 신장의 제곱으로 나누어 신장이 증가할 수록 사지근육량이 증가하는 것을 보정한 것을 근육량지수(skeletal muscle index)라고 정의하였다.4,7)
5. 통계 분석
통계분석은 IBM SPSS Statistics for Windows, version 21.0 (IBM Co., Armonk, NY, USA) 프로그램을 이용하였고, 모든 값은 평균 또는 분 율과 표준오차로 제시하였으며, 유의수준은 P-value <0.05로 정의하 였다. 모든 분석은 제시된 가중치를 이용하여 복합표본 분석방법을 사용하였다. 각 군의 변수 중 범주형 변수의 비교는 카이제곱 검정 을 이용하였고, 연속형 변수의 비교는 t 검정을 이용하였다. 비타민 D, 칼로리 섭취량, 단백질 섭취량, 칼슘 섭취량, 나트륨 섭취량, 가구 균등화소득은 정규분포를 하지 않아 로그치환 후 분석에 이용하였 다. 골밀도와 연관성이 높은 여러 변수들과 각 부위별 골밀도와의 연관성을 살펴보기 위하여 다중선형회귀분석을 시행하였다. 근육 량지수와 골다공증의 연관성을 알아보기 위해 로지스틱 회귀분석 을 시행하여 교차비와 95% 신뢰구간을 구하였다.
노재혁 외. 한국 60세 이상 남녀의 근감소와 골다공증과의 연관성 Korean Journal of Family Practice
KJFP
결 과
대상자 평균 연령은 남자 68.5세(표준오차 0.3), 여자 70.4세(표준오 차 0.3)였고, 골다공증 유병률은 남자 10.9% (표준오차 1.2), 여자 50.4% (표준오차 2.0)였다. 연령은 남녀 모두 골다공증군에서 더 높았 으나, 신장, 체중, 체질량지수, 허리둘레, 총 지방량, 체지방률, 근육량 지수, 단백질 섭취량, 칼슘 섭취량은 남녀 모두 골다공증이 없는 군 에서 유의하게 더 높았다(Table 1).
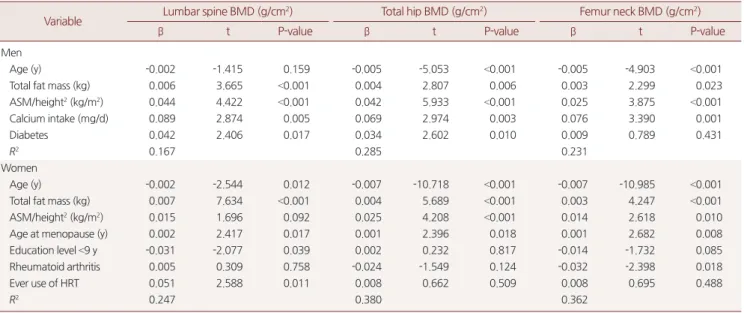
골밀도에 영향을 미치는 요인을 확인하기 위하여 선형회귀분석 을 실시한 결과, 남성에서 총 지방량, 근육량지수, 칼슘섭취량은 골 밀도 증가에 따라 유의한 상관관계를 보였으며, 연령은 대퇴 전체와 대퇴 경부 골밀도 감소에 유의한 상관관계를 보였다. 당뇨병의 경우
는 요추 골밀도 및 대퇴 전체 골밀도 증가와 유의한 상관관계를 보였 다. 여성에서 연령은 골밀도 감소와 유의한 상관관계를 보였으며, 총 지방량, 폐경 연령은 골밀도 증가에 유의한 연관성을 보였다. 근육량 지수는 대퇴 전체와 대퇴 경부 골밀도와 유의한 상관관계를 나타냈 다(Table 2).
남녀 각각에서 근육량지수(ASM/height2)가 1 kg/m2 증가 시 골다 공증 유병 위험과의 관련성을 확인하기 위하여 모형을 세 단계로 구 성하였다. 일 단계 모형으로 연령과 총 지방량을 보정하였고, 두 번 째 단계로 칼슘 섭취량, 여자에서 폐경 연령, 교육 수준, 류마티스관 절염 및 여성호르몬 대체요법, 남자에서 당뇨병 여부를 추가로 포함 하였고, 세 번째 모형으로 단백질 섭취량, 가구균등화소득, 흡연력, 근력 운동 변수를 추가 보정하여 분석하였다(Table 3). 남자에서 근
Table 1. General characteristics of elderly Korean with and without osteoporosis (n=1,728) Variable
Men Women
Without osteoporosis (n=677)
With osteoporosis
(n=88) P-value Without osteoporosis (n=497)
With osteoporosis
(n=466) P-value
Age (y) 67.9±0.3 73.1±0.8 <0.001 67.3±0.3 73.2±0.4 <0.001
Height (cm) 166.1±0.3 162.8±0.8 <0.001 153.4±0.3 149.6±0.3 <0.001
Weight (kg) 65.5±0.4 56.6±1.0 <0.001 59.3±0.4 52.1±0.4 <0.001
Body mass index (kg/m2) 23.7±0.1 21.4±0.3 <0.001 25.2±0.2 23.2±0.2 <0.001
Waist circumference (cm) 86.1±0.4 79.4±1.0 <0.001 85.4±0.5 81.2±0.5 <0.001
Total fat mass (kg) 15.8±0.3 12.8±0.5 <0.001 21.7±0.3 18.1±0.3 <0.001
Body fat (%) 23.9±0.3 22.2±0.6 0.006 36.3±0.4 34.3±0.4 <0.001
ASM/height2 (kg/m2) 7.27±0.05 6.72±0.09 <0.001 5.97±0.04 5.71±0.04 <0.001
25(OH)D* (ng/mL) 21.2±0.5 20.4±1.0 0.423 18.7±0.6 18.0±0.5 0.501
Total energy intake* (kcal/d) 2,115±37 2,017±113 0.169 1,531±32 1,475±29 0.076
Protein intake* (g/d) 73.6±1.7 60.9±4.3 0.007 50.6±1.5 45.6±1.1 0.002
Calcium intake* (mg/d) 558.8±15.1 439.6±38.1 0.006 447.5±20.0 361.4± 3.7 0.001
Sodium intake* (mg/d) 5,467±142 4,721±338 0.119 3,575±149 3,591±129 0.728
Age at menarche (y) - - - 16.4±0.1 16.6±0.1 0.115
Age at menopause (y) - - - 49.7±0.3 47.7±0.4 <0.001
Equivalent income*,†
(×104 Korean won)
154.5±7.7 152.0±59.9 0.002 135.4±12.2 121.8±9.8 0.055
Marital status: single 9.1 (1.3) 9.9 (3.5) 0.830 40.7 (2.6) 58.6 (2.9) <0.001
Education level <9 y 42.5 (2.7) 58.3 (6.1) 0.014 74.5 (2.2) 92.3 (1.3) <0.001
Current smoker 28.7 (1.9) 26.3 (5.8) 0.710 2.0 (0.7) 6.3 (1.6) 0.005
High-risk alcohol drink 11.8 (1.8) 11.3 (4.8) 0.924 0.3 (0.3) 0.5 (0.3) 0.755
High-intensity PA 84.4 (1.9) 82.2 (5.0) 0.647 9.1 (1.6) 7.7 (1.6) 0.519
Moderate-intensity PA 88.8 (1.5) 87.6 (3.7) 0.747 11.4 (1.6) 9.1 (1.3) 0.240
Walking 44.9 (1.9) 40.1 (6.7) 0.472 46.2 (3.0) 33.9 (2.7) 0.001
Muscle strength training 32.3 (2.1) 17.5 (4.7) 0.011 14.7 (2.0) 4.4 (0.9) <0.001
Diabetes 21.0 (2.0) 13.2 (4.3) 0.164 24.1 (2.7) 17.9 (2.5) 0.096
Rheumatoid arthritis 2.2 (0.7) 1.4 (1.1) 0.605 3.1 (0.8) 6.2 (1.1) 0.027
Thyroid disease 0.8 (0.4) 1.7 (1.2) 0.394 7.8 (1.3) 4.7 (1.1) 0.072
Family history of osteoporosis 8.0 (1.3) 6.9 (4.0) 0.804 18.4 (2.1) 12.2 (1.9) 0.018
Ever use of HRT - - - 17.0 (1.8) 7.2 (1.5) <0.001
Data are expressed as estimated mean±standard error or estimated percentage (standard error), as appropriate. P-values are those of Student’s t-test for means or chi- square test for proportions.
ASM, appendicular skeletal muscle mass; 25(OH)D, 25-hydroxyvitamin D; PA, physical activity; HRT, hormone replacement therapy.
*Values presented are the estimated means but log-transformed values were used for comparisons. †Equivalent income=monthly household income/√family size.
Jae-Hyeok Ro, et al. Sarcopenia and Osteoporosis in Aged Older than 60 Years
Korean Journal of Family Practice
KJFP
육량지수가 1 kg/m2 증가 시 1단계 모형의 골다공증 유병 여부에 대 한 교차비는 0.587 (95% 신뢰구간, 0.400–0.861), 2단계 모형의 교차비 는 0.615 (95% 신뢰구간, 0.421–0.898), 3단계 모형의 교차비는 0.610 (95% 신뢰구간, 0.416–0.894)으로 통계적으로 유의한 차이를 나타냈 다. 여자에서는 근육량지수가 1 kg/m2 증가 시 1단계 모형의 골다공 증 유병 여부에 대한 교차비는 0.691 (95% 신뢰구간, 0.522–0.916), 2단 계 모형의 교차비는 0.655 (95% 신뢰구간, 0.474–0.904), 3단계 모형의 교차비는 0.650 (95% 신뢰구간, 0.467–0.905)였다.
고 찰
본 연구는 국민건강영양조사 자료를 기반으로 60세 이상 노년 인 구에서 근육량지수와 골다공증 간의 관련성을 분석한 결과로서, 골 다공증과 관련된 다른 요인들을 보정한 후에도 근육량지수 증가 시 골다공증 위험이 낮아질 수 있음을 보여주었다.
급속한 노인 인구의 증가로 인해 유병률이 높아지고 있는 골다공 증은 이와 관련된 골절에 의해 많은 의료비 지출을 동반한다. 골밀 도 감소 및 골다공증의 발생은 선천적인 유전인자와 후천적인 환경 인자에 의해 영향을 받는다. 아직 골다공증의 발생에 영향을 미치는 선천적인 유전적인 인자가 모두 밝혀져 있지는 않지만, 현재까지 보 고된 것은 비타민 D 수용체 유전자 다형성과 에스트로겐 수용체 유 전자 다형성 및 제1형 콜라겐 유전자 다형성 등이 있다. 후천적인 환 경인자로는 폐경, 저체중, 늦은 초경, 오랜 폐경기간, 적은 칼슘 섭취 량, 음주, 흡연 및 운동 등의 여러 인자들이 골대사에 영향을 주는 것 으로 알려지고 있다.12) 이들 중 체중이 골다공증의 중요한 위험인자 로 잘 알려져 있으며 골밀도에 영향을 주게 되는 원인은 체중이 골격 계에 스트레스로 작용하기 때문에 스트레스가 작용하는 부위의 골 형성세포의 활성도가 증가하게 되어 골량이 증가하는 효과를 보이 기 때문이다.13,14)
본 연구는 폐경 후 여성과 남성을 포함하여 체중, 근육량과 골다 Table 2. Multiple linear regression analysis of relationship between bone mineral density of the lumbar spine, total hip, and femur neck and various parameters*
Variable Lumbar spine BMD (g/cm2) Total hip BMD (g/cm2) Femur neck BMD (g/cm2)
β t P-value β t P-value β t P-value
Men
Age (y) -0.002 -1.415 0.159 -0.005 -5.053 <0.001 -0.005 -4.903 <0.001
Total fat mass (kg) 0.006 3.665 <0.001 0.004 2.807 0.006 0.003 2.299 0.023
ASM/height2 (kg/m2) 0.044 4.422 <0.001 0.042 5.933 <0.001 0.025 3.875 <0.001
Calcium intake (mg/d) 0.089 2.874 0.005 0.069 2.974 0.003 0.076 3.390 0.001
Diabetes 0.042 2.406 0.017 0.034 2.602 0.010 0.009 0.789 0.431
R2 0.167 0.285 0.231
Women
Age (y) -0.002 -2.544 0.012 -0.007 -10.718 <0.001 -0.007 -10.985 <0.001
Total fat mass (kg) 0.007 7.634 <0.001 0.004 5.689 <0.001 0.003 4.247 <0.001
ASM/height2 (kg/m2) 0.015 1.696 0.092 0.025 4.208 <0.001 0.014 2.618 0.010
Age at menopause (y) 0.002 2.417 0.017 0.001 2.396 0.018 0.001 2.682 0.008
Education level <9 y -0.031 -2.077 0.039 0.002 0.232 0.817 -0.014 -1.732 0.085
Rheumatoid arthritis 0.005 0.309 0.758 -0.024 -1.549 0.124 -0.032 -2.398 0.018
Ever use of HRT 0.051 2.588 0.011 0.008 0.662 0.509 0.008 0.695 0.488
R2 0.247 0.380 0.362
BMD, bone mineral density; ASM, appendicular skeletal muscle mass; HRT, hormone replacement therapy.
*Age, total fat mass, ASM/height2, total energy intake (log-transformed), protein intake (log-transformed), calcium intake (log-transformed), age at menopause (only in women), equivalent income (log-transformed), marital status, education level, cigarette smoking status, physical activity level such as walking and muscle strength train- ing, medical history of diabetes, rheumatoid arthritis, and thyroid disease, family history of osteoporosis, and history of use of hormone replacement therapy (only in women).
Table 3. Osteoporosis associated with increase in muscle mass index (increase of 1 kg/m2 for ASM/height2)
Models Men
P-value Women
P-value
OR (95% CI) OR (95% CI)
Model 1 0.587 (0.400–0.861) 0.007 0.691 (0.522–0.916) 0.010 Model 2 0.615 (0.421–0.898) 0.012 0.655 (0.474–0.904) 0.011 Model 3 0.610 (0.416–0.894) 0.012 0.650 (0.467–0.905) 0.011 ASM, appendicular skeletal muscle mass; OR, odds ratio; CI, confidence interval.
Model 1 was adjusted for age and total fat mass. Model 2 was adjusted for cal- cium intake (log-transformed; only in men), age at menopause (only in women), education level (only in women), medical history of diabetes (only in men) and rheumatoid arthritis (only in women), and history of use of hormone replace- ment therapy (only in women) in addition to the covariates included in model 1.
Model 3 was adjusted for protein intake (log-transformed), equivalent income (log-transformed), cigarette smoking status, and muscle strength training in ad- dition to the covariates included in model 2.
노재혁 외. 한국 60세 이상 남녀의 근감소와 골다공증과의 연관성 Korean Journal of Family Practice
KJFP
공증과의 관계를 살펴본 다른 연구들의 결과와 유사하다.8,15-17) 한편, 골밀도는 체질량지수와 상관관계가 있다고 알려져 있으며 체중을 구성하는 근육, 체지방, 골격 등 각각의 체성분과 골밀도와의 상관관 계에 대한 연구들이 발표되고 있다. Sower 등18)은 제지방량과 체지 방 백분율, 상완부의 근육량과 지방량 등을 포함한 체성분보다 체 중이 대퇴골부위 골밀도와 상관관계가 높다고 보고하였으나 이듬 해에는19) 젊은 여성에서는 근육량이 적을 시 골다공증의 위험인자 이며 풍부한 근육과 연관된 지방량이 많으면 골다공증을 예방한다 고 하였다.
체지방과 골밀도의 관련성에 대하여 과거 서양인을 대상으로 한 연구에서 체지방은 골밀도와 양의 상관관계를 가지는 것으로 나타
났으나,20,21) 체지방량이 가지는 물리적 하중부하를 보정하면 체지방
이 높을수록 골밀도가 낮다는 의견도 최근 제시되고 있다.22) 또한 1,694명의 한국 여성을 대상으로 한 연구에서 체중을 보정 한 후 체 지방량이 많아질수록 요추 골밀도가 감소하는 음의 관련성을 보여 주었다.23) 체지방이 골밀도에 영향을 주는 기전으로는 뼈에 물리적 인 하중을 더하여 뼈를 자극할 뿐 아니라, 폐경 후에는 남성호르몬 인 안드로겐을 에스트로겐으로 변환시켜 골 소실을 예방해 주는 효 과가 있다고 알려져 있다. 이러한 기전 이외에도 비만한 사람은 인슐 린 저항성을 동반한 경우가 많은데, 인슐린 저항성은 인슐린의 혈당 저하 기능만 감소하고 나머지 인슐린의 기능은 유지되는 상태로, 인 슐린 증가로 인해 간의 성호르몬결합 글로불린 생산이 감소하고 이 로 인해 활성화된 에스트로겐이 증가하여 골 소실 예방이 가능한 것으로 생각된다.24)
본 연구는 다음과 같은 제한점이 있다. 첫째, 국민건강영양조사를 이용한 단면연구이기 때문에 골밀도 감소와 연관된 요인들 사이에 원인-결과 관계를 확립하기 어렵다. 둘째, 영양섭취의 경우 설문 조 사 시 연구 대상자가 회상을 잘못하거나 거짓말 등으로 정보가 왜곡 될 수 있는 자기 기입식 설문조사의 한계(recall bias)를 갖고 있어 조 사된 섭취량이 평소의 섭취량보다 과다하게 혹은 부족하게 반영되 었을 가능성을 배제하기 어렵다. 셋째, 본 연구에서는 골밀도에 영향 을 줄 수 있는 연령, 총 지방량, 칼슘섭취량, 단백질섭취량, 가구균등 화소득, 흡연 여부, 근력운동, 여자에서 폐경 연령, 교육 수준, 류마티 스관절염, 여성호르몬 대체요법, 남자에서 당뇨병 여부 등을 보정하 였으나, 그 이외에 골밀도에 영향을 줄 수 있는 요인 중 고려하지 못 한 변수들이 있을 수 있다. 관련된 요인으로 초경 연령, 부갑상선 호 르몬 등이 있을 수 있는데, 과거 연구에서 이들이 골밀도에 주는 영 향은 연령이나 총지방량 등 본 연구에서 고려한 주요 변수들보다 미 치는 영향이 크지 않은 것으로 나타나 본 연구 결과 변화는 미미할 것으로 생각된다.25-27) 넷째, 골다공증 자체보다 골다공증성 골절 여
부가 분석에 고려되지 않았다는 점이다. 여러 제한점에도 불구하고, 본 연구는 한국인을 대표할 수 있는 국민건강영양조사 자료를 바탕 으로 하여 한국 60세 이상 남녀 각각의 근감소와 골다공증과의 연 관성이 있다는 것을 밝힌 데 의의가 있다고 하겠다.
결론적으로 본 연구에서 근육량지수(ASM/height2)가 증가할수 록 골다공증 교차비가 감소하는 결과를 보여 주고 있어 노년 인구에 서 골다공증의 치료 및 예방을 위하여 약물요법 외에도 근육량 증 가를 위한 중재가 중요할 것으로 생각된다.
요 약
연구배경:
대표성 있는 자료를 기반으로 하여 60세 이상 남녀간 근 육량 감소에 따른 골다공증의 관련성에 대해 알아보고자 하였다.방법:
본 연구는 5기 국민건강영양조사(2010년) 자료를 이용하였고 60세 이상 참여자 1,728명(남자 765명, 여자 963명)을 최종 분석 대상 자로 하였다. 대퇴부 전체, 대퇴 경부 및 요추의 골밀도와 체성분은 이중에너지 X-선 흡수방법(dual-energy X-ray absorptiometry)으로 측 정하였다. 다중선형회귀분석 및 로지스틱 회귀분석을 이용하여 근 육량지수와 골밀도 및 골다공증의 연관성을 분석하였다.결과:
대상자 평균 연령은 남자 68.5세(표준오차 0.3), 여자 70.4세(표 준오차 0.3)이었고, 골다공증 유병률은 남자 10.9% (표준오차 1.2), 여 자 50.4% (표준오차 2.0)이었다. 골다공증의 유병 위험은 근육량지수 가 1 kg/m2 증가할수록 남성에서 0.615배(95% 신뢰구간, 0.416–0.894), 여성에서 0.650배(95% 신뢰구간, 0.467–0.905) 감소하였다.결론:
60세 이상 성인에서 근육량지수가 증가할수록 골다공증의 유병 위험이 감소하는 결과를 보여주고 있어 노년 인구에서 골다공 증의 예방을 위하여 근육량 증가를 위한 중재가 중요할 것으로 생각 한다.중심단어:
근감소증; 골다공증; 근육량지수; 국민건강영양조사REFERENCES
1. Korean Statistical Information Service. Statistics Korea [Internet]. [cited 2014 Aug 4]. Available from: http://kostat.go.kr/portal/korea/kor_nw/3/in- dex.board?bmode=read&bSeq=&aSeq=306746&pageNo=68&rowNum=
10&navCount=10&currPg=&sTarget=title&sTxt=.
2. Cesari M, Leeuwenburgh C, Lauretani F, Onder G, Bandinelli S, Maraldi C, et al. Frailty syndrome and skeletal muscle: results from the Invecchiare in Chianti study. Am J Clin Nutr 2006; 83: 1142-8.
3. Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al.
Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci 2001; 56: M146-56.
Jae-Hyeok Ro, et al. Sarcopenia and Osteoporosis in Aged Older than 60 Years
Korean Journal of Family Practice
KJFP
4. Janssen I, Heymsfield SB, Ross R. Low relative skeletal muscle mass (sarco- penia) in older persons is associated with functional impairment and physi- cal disability. J Am Geriatr Soc 2002; 50: 889-96.
5. Morley JE. Diabetes, sarcopenia, and frailty. Clin Geriatr Med 2008; 24: 455- 69, vi.
6. Janssen I, Shepard DS, Katzmarzyk PT, Roubenoff R. The healthcare costs of sarcopenia in the United States. J Am Geriatr Soc 2004; 52: 80-5.
7. Baumgartner RN, Koehler KM, Gallagher D, Romero L, Heymsfield SB, Ross RR, et al. Epidemiology of sarcopenia among the elderly in New Mexi- co. Am J Epidemiol 1998; 147: 755-63.
8. Blain H, Jaussent A, Thomas E, Micallef JP, Dupuy AM, Bernard PL, et al.
Appendicular skeletal muscle mass is the strongest independent factor asso- ciated with femoral neck bone mineral density in adult and older men. Exp Gerontol 2010; 45: 679-84.
9. Coin A, Sergi G, Marin S, Vianello A, Perissinotto E, Sarti S, et al. Predictors of low bone mineral density in elderly males with chronic obstructive pul- monary disease: the role of body mass index. Aging Male 2010; 13: 142-7.
10. Frisoli A Jr, Chaves PH, Ingham SJ, Fried LP. Severe osteopenia and osteopo- rosis, sarcopenia, and frailty status in community-dwelling older women:
results from the Women’s Health and Aging Study (WHAS) II. Bone 2011;
48: 952-7.
11. Assessment of fracture risk and its application to screening for postmeno- pausal osteoporosis. Report of a WHO Study Group. World Health Organ Tech Rep Ser 1994; 843: 1-129.
12. Kim YI, Park JH, Lee JS, Kim JW, Yang SO, Jeon DJ, et al. Prevalence and risk factors of the osteoporosis of perimenopausal women in the community population. Korean J Med 2002; 62: 11-24.
13. Ravn P, Cizza G, Bjarnason NH, Thompson D, Daley M, Wasnich RD, et al.
Low body mass index is an important risk factor for low bone mass and in- creased bone loss in early postmenopausal women. Early Postmenopausal Intervention Cohort (EPIC) study group. J Bone Miner Res 1999; 14: 1622- 7.
14. Gillette-Guyonnet S, Nourhashemi F, Lauque S, Grandjean H, Vellas B. Body composition and osteoporosis in elderly women. Gerontology 2000; 46:
189-93.
15. Genaro PS, Pereira GA, Pinheiro MM, Szejnfeld VL, Martini LA. Influence of body composition on bone mass in postmenopausal osteoporotic wom-
en. Arch Gerontol Geriatr 2010; 51: 295-8.
16. Pluijm SM, Visser M, Smit JH, Popp-Snijders C, Roos JC, Lips P. Determi- nants of bone mineral density in older men and women: body composition as mediator. J Bone Miner Res 2001; 16: 2142-51.
17. Van Langendonck L, Claessens AL, Lefevre J, Thomis M, Philippaerts R, Delvaux K, et al. Association between bone mineral density (DXA), body structure, and body composition in middle-aged men. Am J Hum Biol 2002; 14: 735-42.
18. Sowers M, Kshirsagar A, Crutchfield M, Updike S. Body composition, age and femoral bone mass of young adult women. Ann Epidemiol 1991; 1:
245-54.
19. Sowers MF, Kshirsagar A, Crutchfield MM, Updike S. Joint influence of fat and lean body composition compartments on femoral bone mineral densi- ty in premenopausal women. Am J Epidemiol 1992; 136: 257-65.
20. Bogl LH, Latvala A, Kaprio J, Sovijärvi O, Rissanen A, Pietiläinen KH. An in- vestigation into the relationship between soft tissue body composition and bone mineral density in a young adult twin sample. J Bone Miner Res 2011;
26: 79-87.
21. Gjesdal CG, Halse JI, Eide GE, Brun JG, Tell GS. Impact of lean mass and fat mass on bone mineral density: The Hordaland Health Study. Maturitas 2008; 59: 191-200.
22. Zhao LJ, Liu YJ, Liu PY, Hamilton J, Recker RR, Deng HW. Relationship of obesity with osteoporosis. J Clin Endocrinol Metab 2007; 92: 1640-6.
23. Kim CJ, Oh KW, Rhee EJ, Kim KH, Jo SK, Jung CH, et al. Relationship be- tween body composition and bone mineral density (BMD) in perimeno- pausal Korean women. Clin Endocrinol (Oxf) 2009; 71: 18-26.
24. Reid IR. Relationships between fat and bone. Osteoporos Int 2008; 19: 595- 606.
25. Albanese CV, Civitelli R, Tibollo FG, Masciangelo R, Mango D. Endocrine and physical determinants of bone mass in late postmenopause. Exp Clin Endocrinol Diabetes 1996; 104: 263-70.
26. Collins D, Jasani C, Fogelman I, Swaminathan R. Vitamin D and bone min- eral density. Osteoporos Int 1998; 8: 110-4.
27. Lau HH, Ng MY, Ho AY, Luk KD, Kung AW. Genetic and environmental de- terminants of bone mineral density in Chinese women. Bone 2005; 36: 700- 9.