The effects of virtual reality programs on stroke survivors †
Sung-hyun Ryu 1 · Sun Wook Lee 2
1 Ocupational Therapy, Soon Chun Hyang University Hospital
2 Department of Occupational Therapy, Daegu University
Received 26 August 2020, revised 6 September 2020, accepted 7 September 2020
Abstract
Although virtual-reality-based (VR-based) approaches are considered innovative in- terventions, little is known about how they affect stroke survivors’ participation. This study documents the effects of VR-based occupational therapy intervention compared with those of standard physical disability intervention. In a randomized controlled trial, 32 stroke survivors in either a VR-based occupational therapy group or a comparison group received designated intervention for 5 weeks. We found that the VR-based oc- cupational therapy program decreased the Beck Depression Index score with medium effect, increased motivation for rehabilitation scale scores with large effect, and in- creased the total Model of Human Occupation Screening Tool score with large effect.
VR-based occupational therapy for stroke survivors may help enhance motivation for occupation and environment aspects among the six factors necessary for returning to life participation.
Keywords: Model of human occupation screening tool, occupational therapy, virtual reality.
1. Introduction
Multiple factors influence the incidence of stroke care. A meta-analysis including 46 studies (30 psychological factors, 13 vocational factors, 10 interpersonal factors, and 2 behavioral factors) indicated that stroke risk increased by 39% with psychological factors (HR, 1.39 [95% CI, 1.27-1.51]), 35% with vocational factors (HR, 1.35 [95% CI, 1.20-1.51]), and 16%
with interpersonal factors (HR, 1.16 [95% CI, 1.03-1.31])(Clegg et al., 2017). So does the care process for the stroke survivors. A neuroanatomist who survived a stroke, Dr. Jill Bolte Taylor, recounted,
† This study was undertaken by Sung-hyun Ryu in partial fulfillment of the requirements for the degree of Master’s in Rehabilitation Science at Daegu University.
1
Occupational Therapist, Soon Chun Hyang University Hospital, Cheonan 31151, Korea
2
Corresponding author: Assistant Professor, Department of Occupational Therapy, Rehabilitation Sci-
ence, Daegu University, Gyeongsan 38453, Korea. E-mail: [email protected]
I desperately needed people to accept me as the person I was at that moment· · · . I needed those around me to be encouraging. I needed to know that I still had value. I needed to have dreams to work toward· · · . For a successful recovery, it was important that we focus on my ability, not my disability. (Taylor, 2006, pp. 110-121)
The inception of the contemporary conceptualization of health care system centering on participation in life was stipulated by the International Classification of Functioning, Disabil- ity and Health [ICF] in 2001. Since then, the rehabilitation sector has emphasized activity and participation; corresponding changes have been enacted, subsequently transforming the everyday therapy encounter (Dahl, 2002; Perenboom and Chorus, 2003). Occupational ther- apy, which serves multiple populations, including those needing rehabilitation, aligns with ICF in using participation as a core professional construct. Real-life applications focusing on participation have been guided by the profession’s conceptual practice models (Haglund and Henriksson, 2003; Hemmingsson and Jonsson, 2005). Moreover, with the recent release of the International Statistical Classification of Diseases and Related Health Problems (11th ed.; ICD-11; World Health Organization, 2018), and legislative change in Korea to include occupational therapists as providers of mental health services, innovative evidence-based practices that increase service users’ participation are further required.
As such, virtual-reality (VR)-based interventions and research into innovative interven- tion vehicles have been highlighted in the last decades. The profession has increased its attention to the virtual context as a component of the environment factor, referring to VR-based interactions as interactions that occur in simulated, real-time, or near-time sit- uations absent of physical contact (p. S9), (American Occupational Therapy Association, 2014). Such attention comes not only from occupational therapists but also from interdisci- plinary health care teams, as evidenced in several systematic review and/or meta-analyses using VR intervention research. Most of these studies examined the effects of either custom- built virtual-environment-based programs and/or commercial available gaming systems on variables ranging from bodily functions, such as ambulation, cognitive aspects, and upper extremity capacities, to daily functioning, such as activities of daily living, to health-related factors such as quality of life (de Rooij et al., 2016; Grampurohit et al., 2019; Henderson et al., 2007; Lee et al., 2019; Moreira et al., 2013; Ogourtsova et al., 2017; Subramanian and Prasanna, 2018). What is missing among these is well stated in a systematic review study from the earliest available date to 2013, Lohse and colleagues’ (2014) call for VR studies on participation measures and motivating components. Indeed, despite the utility of VR as a motivating component, the evidence pertaining to its impacts on psychosocial aspects of the stroke on service users has been given much less attention to date (Mottura et al., 2015; Reid and Hirji, 2004; Shin et al., 2017), and even when participation level has been measured, the effects of immersive experience in VR-based therapy on participation remain elusive (Laver et al., 2011).
The Model of Human Occupation Screening Tool (MOHOST, Parkinson et al., 2006) is a
theory-based outcome measure whereby the total score represents a person’s participation
while the comparison of the six subscales/factors indicates where to target to promote the
participation level based on the model of human occupation (MOHO), an occupational ther-
apy model (Taylor and Kielhofner, 2017). The MOHO is the most widely used occupation-
focused model internationally (i.e., focusing on participation and dynamics of a person’s
motivation for occupation, roles and routines (i.e., habituation), three different skills for
doing, and environment)(Lee, 2010; Wong and Fisher, 2015). By harnessing the effects of innovative interventions such as VR-based OT based on the established theory, this study sought to explore and document the utility of a VR-based occupational therapy program for factors influencing stroke survivor participation. Therefore, we examined the effects of VR-based occupational therapy intervention in addition to the conventional, standard care (SC) occupational therapy intervention, compared with the effects of SC occupational ther- apy intervention only and measured three different outcomes: depression, motivation for rehabilitation, and six factors influencing stroke survivor participation.
2. Methods
2.1. Design
As a randomized controlled trial, this study employed two-group comparison consisting of the virtual-reality program (VR) group or standard care (SC) group before and after a 5-week intervention period for 32 stroke survivors. The ethical approval was acquired before the study from Daegu university (IRB No. 1040621-201411-HR-023-02).
2.2. Participants
As no direct previous domestic research was available as a baseline for the MOHOST, a minimum sample size for an experimental study was employed (Cohen et al., 2013); and an attrition rate due to transfer to other facilities was regarded for the final decision of 32 participants.
The inclusion criteria were as follows: (a) a stroke diagnosed by computerized tomography and/or magnetic resonance imaging; (b) a score 4 on the Mini-Mental State Examination- Korean version (MMSE-K); (c) no visual and/or auditory impairments/disabilities interfer- ing with tasks; and (d) currently not participating in other studies. The exclusion criteria included (a) comorbid history of other neurological/psychological diagnoses; and (b) inca- pable of participation in activities following instructions.
2.3. Measures
2.3.1. Beck depression inventory (BDI)
BDI (Beck et al., 1996), comprising 21 items, measures non-physical depression (13 items) and physical depression (seven items). A modified version adapted for stroke survivors (Hahn et al., 1986) rated from zero to three, delineates “not depressed” (0-9), “slightly depressed”
(10-15), “moderately depressed” (16-23), and “severely depressed” (24-63). Cronbach’s α for participants without disabilities was 0.89, whereas that for participants living with depres- sion was 0.94.
2.3.2. The scale for the motivation for rehabilitation
A modified version (Kim et al., 2009) of the original scale (Han and Lim, 2002) measuring
motivation for stroke survivors measures five different types of motivation for rehabilitation
services: task-oriented (eight items), change-oriented (seven items), compulsory (four items),
external (four items), and amotivation (four items), totaling 27 items. A 4-point Likert scale
with ratings of not at all (1), very little (2), somewhat (3), or to a great extent (4) was used, and the amotivation subscale was reverse coded. Scores can range from 27 to 108; the higher the score, the more motivated the participant is for rehabilitation services. Cronbach’s α for the original version was 0.86; that for the 123 stroke clients was 0.89; and that for the current study was 0.91.
2.3.3. Model of human occupation screening tool (MOHOST)
MOHOST is a screening measure for the occupational therapy intervention process (Parkin- son et al., 2006). Comprising six factor areas (i.e., motivation for occupation, patterns of occupation, communication/interaction skills, process skills, motor skills, and environment), it provides a numerical and visual profile of areas of strength or weakness to facilitate one’s participation in life. The total of 24 items (i.e., four items per factor or a subscale) renders a score ranging from 24 to 96. Using multiple methods (i.e., observation, interviews, and/or proxy reports), a therapist rates whether an item either facilitates (4), allows (3), interferes (2), or restricts (1) a client’s participation. Applicability and psychometric properties of the MOHOST in multi-cultural environments has been documented (Kielhofner et al., 2010;
Pan et al., 2011).
2.4. Procedure
Thirty-two stroke survivors recruited from a metropolitan area who consented to partic- ipate were randomly allocated into two groups. In each group, 16 participants’ depression, motivation for rehabilitation, and occupational participation level were measured to test the group’s homogeneity at baseline. The comparison group participants received standard OT interventions eight times per week, mainly consisting of neurodevelopmental occupa- tional therapy approaches focused on inhibiting muscle spasms and abnormal movement patterning, sensory stimulation, positioning, and bilateral upper extremities using occupa- tional therapy to facilitate normal movement for participation. The intervention was carried out by 14 therapists. On the contrary, the experimental group had VR training 3 times per week and standard care occupational therapy program five times per week as described in the following section.
2.4.1. Virtual reality (VR) training program
Nintendo Wii ® gaming technology, which provides a choice of activities in a safe en- vironment was employed for the VR program. The Wii system comprised a TV monitor, gaming CD, Wii sensor box, and remote control. A wireless Bluetooth connection-activated enabled a motion sensor to capture movement within 5 m of the TV screen. In turn, it provided participants with feedback on wrist, arm, and hand in direction, speed, and accel- eration in 3-axis format, all of which movement an avatar realized on screen. This motion detection system provided immediate visual and auditory feedback on successful or failed performance. Further details are described online (http://www.nintendo.com). The feed- back the TV screen provided generated positive reinforcement, thus facilitating a client’s training and task improvement. The following, iterative process was employed:
Step 1 (Temporality and Delivery): Participants chose three out of five mini-programs
(e.g., tennis, baseball, gold, bowling, or boxing) with their own interests and prefer-
ences; they used each wii program for 10 minutes for a total of 30 minutes, exclusive of other scheduled treatment.
Step 2 (Person-environment fit): The environment for the Wii program was modified to eliminate noises and other interference so as to maximize attention span; adapted positioning (e.g., sitting compared to standing) was applied to prevent falling and to support balancing; five minutes of intermittent break was provided when associated movement occurred and/or participants indicated a fatigue response.
Step 3 (Designing successful participation): Physical support was provided, such as distributing body weight by holding the participant’s elbow and/or using non-stroke side, strapping for secure grip of the remote control, along with detailed/repetitive explanation about how to use the Wii, including appropriate distance, positioning, and/or cautions in performing the task during the entire intervention time period.
2.5. Data analysis
SPSS version 25.0 was used to analyze our data (SPSS, Inc., Chicago, IL). Descriptive statistics, Fisher’s exact test, Fisher-Freeman-Halton exact test of independence, and Chi- square test were conducted for between-group comparisons at baseline for demographic information. Independent t-test or Mann-Whitney U test was used for between-group com- parisons of depression, motivation for rehabilitation, and occupational participation. Paired-t test or Wilcoxon signed-rank test was performed for the within-group comparisons for the 5-week intervention period. With statistical significance set at .05, clinical differences us- ing Cohen’s d and Rosenthal’s r were calculated; a correlation analysis was performed to establish correlations among the three outcome variables.
3. Results
3.1. Participant characteristics
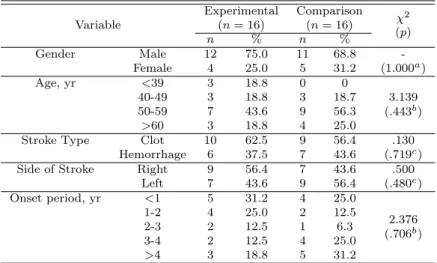
Participants for both groups included more men than women. The mean age for the
experimental group was 51.5 (SD=15.94), whereas that for the comparison group was 56.3
(SD=9.87). We found no statistically different demographic characteristics in relation to
stroke experience (Table 3.1) and three outcome measures at baseline (Table 3.2).
Table 3.1 The general characteristics of the participants at baseline (N=32)
Variable
Experimental Comparison χ
2(n = 16) (n = 16)
n % n % (p)
Gender Male 12 75.0 11 68.8 -
Female 4 25.0 5 31.2 (1.000
a)
Age, yr <39 3 18.8 0 0
3.139
40-49 3 18.8 3 18.7
(.443
b)
50-59 7 43.6 9 56.3
>60 3 18.8 4 25.0
Stroke Type Clot 10 62.5 9 56.4 .130
Hemorrhage 6 37.5 7 43.6 (.719
c)
Side of Stroke Right 9 56.4 7 43.6 .500
Left 7 43.6 9 56.4 (.480
c)
Onset period, yr <1 5 31.2 4 25.0
2.376
1-2 4 25.0 2 12.5
(.706
b)
2-3 2 12.5 1 6.3
3-4 2 12.5 4 25.0
>4 3 18.8 5 31.2
a
Fisher’s exact test (2-sided)
b
Fisher-Freeman-Halton exact test of independence
c
Chi-square test
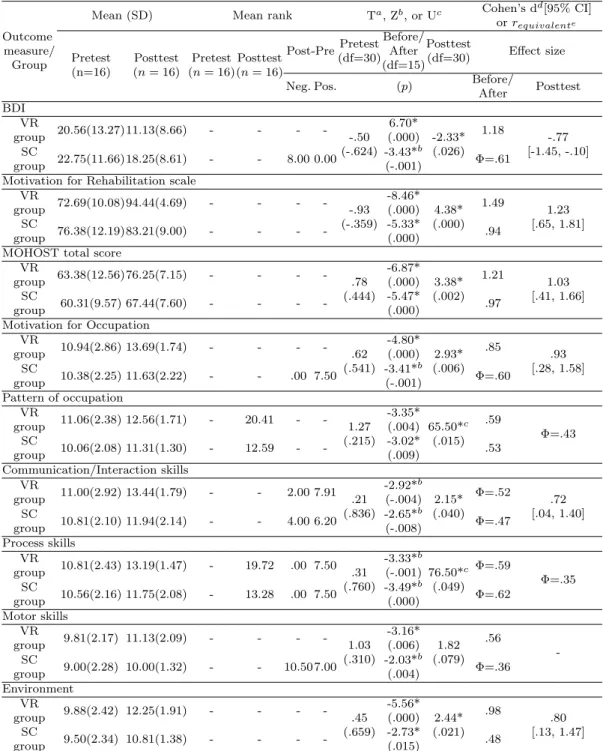
3.2. Within-group comparison of depression, motivation for rehabilitation, and occupational participation
Table 3.2 shows the within-group comparison and the between-group comparison. First,
for the BDI, both groups showed statistically different changes when compared before and
after the 5-week intervention period. The magnitude of clinical difference was larger in the
VR-based OT group, compared with the medium effect in the SC group. Second, the total
score on the motivation for rehabilitation scale also differed significantly for both groups
with large effects. Third, the total MOHOST score also showed a significant change in
participation level for both groups with large effects. When we looked at the six MOHOST
subscales, for the VR-based group, we observed a large effect in motivation for occupation,
communication/interaction skills, process skills, and environment, whereas we observed a
medium effect in habituation and motor skills; for the SC group, we observed a large effect
in motivation for occupation and process skills and a medium effect in habituation and
communication and interaction skills. We observed small effects in the motor skills and the
environment factors.
Table 3.2 The general characteristics of the participants at baseline (N=32)
Outcome
Mean (SD) Mean rank T
a, Z
b, or U
cCohen’s d
d[95% CI]
measure/
or r
equivalenteGroup Pretest Posttest Pretest Posttest Post-Pre Pretest Before/
Posttest
Effect size (n=16) (n = 16) (n = 16)(n = 16)
(df=30) After
(df=30) (df=15)
Neg. Pos. (p) Before/
Posttest After
BDI
VR 20.56(13.27)11.13(8.66) - - - -
-.50 6.70*
-2.33* 1.18
-.77 group
(-.624) (.000)
(.026) [-1.45, -.10]
SC 22.75(11.66)18.25(8.61) - - 8.00 0.00 -3.43*
bΦ=.61
group (-.001)
Motivation for Rehabilitation scale
VR 72.69(10.08)94.44(4.69) - - - -
-.93
-8.46*
4.38* 1.49
1.23 group
(-.359) (.000)
(.000) [.65, 1.81]
SC 76.38(12.19)83.21(9.00) - - - - -5.33*
group (.000) .94
MOHOST total score
VR 63.38(12.56)76.25(7.15) - - - -
.78
-6.87*
3.38* 1.21
1.03 group
(.444) (.000)
(.002) [.41, 1.66]
SC 60.31(9.57) 67.44(7.60) - - - - -5.47*
group (.000) .97
Motivation for Occupation
VR 10.94(2.86) 13.69(1.74) - - - -
.62
-4.80*
2.93* .85
.93 group
(.541) (.000)
(.006) [.28, 1.58]
SC 10.38(2.25) 11.63(2.22) - - .00 7.50 -3.41*
bΦ=.60
group (-.001)
Pattern of occupation
VR 11.06(2.38) 12.56(1.71) - 20.41 - - 1.27
-3.35*
65.50*
c.59
Φ=.43 group
(.215) (.004)
(.015)
SC 10.06(2.08) 11.31(1.30) - 12.59 - - -3.02*
group (.009) .53
Communication/Interaction skills
VR 11.00(2.92) 13.44(1.79) - - 2.00 7.91 .21
-2.92*
b2.15* Φ=.52
.72 group
(.836) (-.004)
(.040) [.04, 1.40]
SC 10.81(2.10) 11.94(2.14) - - 4.00 6.20 -2.65*
bΦ=.47
group (-.008)
Process skills
VR 10.81(2.43) 13.19(1.47) - 19.72 .00 7.50 .31
-3.33*
b76.50*
cΦ=.59
Φ=.35 group
(.760) (-.001)
(.049) SC 10.56(2.16) 11.75(2.08) - 13.28 .00 7.50 -3.49*
bΦ=.62
group (.000)
Motor skills
VR 9.81(2.17) 11.13(2.09) - - - -
1.03 -3.16*
1.82 .56 group -
(.310) (.006)
(.079) SC 9.00(2.28) 10.00(1.32) - - 10.50 7.00 -2.03*
bΦ=.36
group (.004)
Environment
VR 9.88(2.42) 12.25(1.91) - - - -
.45
-5.56*
2.44* .98
.80 group
(.659) (.000)
(.021) [.13, 1.47]
SC 9.50(2.34) 10.81(1.38) - - - - -2.73*
group (.015) .48
BDI: Beck depression index, CI: Confidence interval, MOHOST: Model of Human Occupation Screening Tool, Neg.: Negative, Pos.: Positive, SC: Standard care occupational therapy, VR: Virtual reality Wii training program.
a
Independent t-test and cMann-Whitney U test was used for between group comparison at baseline and posttest.
b
Paired-samples t-test and bWilcoxon signed-rank test was used for within group comparison.
d
Cohen’s d was calculated by (mean posttest / mean pretest)/(pooled SD) for group measure scores.
The interpretation is as follows: small= .20, medium = .50, and large= .80.
e