Repeat CT Scan for Non-operative Management of Blunt Splenic Trauma
7
0
0
전체 글
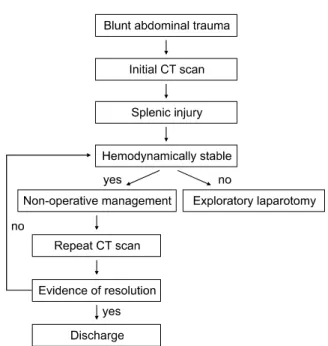
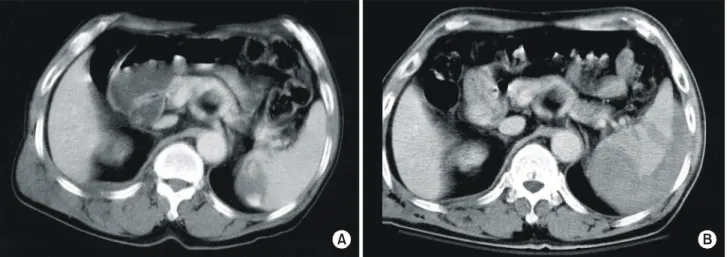
(2) Yong Pil Cho, et al:Repeat CT Scan for Non-operative Management of Blunt Splenic Trauma. 391. ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ. Fig. 1. Management protocol in patients with blunt splenic trauma.. A. C. III injuries were observed and admitted to the intensive care unit to detect any evidence of ongoing hemorrhage and subsequent instability. Repeat CT scan was obtained within 7 days after admission in patients managed non-operatively. A Siemens Somatom CT scanner (Somatom Plus 4, Siemens, Erlangen, Germany) was used in this study. All patients received a total of 100∼150 ml of 60% iodinated solution (Omnipaque 350/100 ml, Amersham Health, Buckinghamshire, England), administered as an initial 50 ml bolus followed by a constant infusion throughout the duration of the scan. Scanning was performed from the lung bases to the iliac crests with 8-mm contiguous sections and continued through the pelvis at 16-mm intervals. Failure of non-operative management was defined as the need for exploratory laparotomy in any patient who was initially admitted to the intensive care unit and managed nonoperatively. The study population was composed of the 49. B. Fig. 2. CT scans of one representative patient successfully managed non-operatively. (A) Initial CT scan revealed a peripheral laceration and posttraumatic infarction with substantial intraperitoneal blood. (B) Follow-up CT scan on day 7 showed improving state of perisplenic hematoma. (C) An additional follow-up CT scan on day 49 showed complete resolution of perisplenic hematoma and healing of splenic injury..
(3) 392. 대한외과학회지:제 67 권 제 5 호 2004. ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ. consecutive patients with blunt splenic trauma between September 2000 and December 2002. Initial CT scans were obtained in all patients. After completion of the initial CT scan, immediate exploratory laparotomy was performed in 20 of 49 patients (40.8%): 10 patients with grade IV or V injuries and the other 10 patients with other significant intra-abdominal injuries. Twenty-nine clinically stable (stable vital signs and hemoglobin levels) patients (59.2%) with grade I, II, or III injuries were initially managed non-operatively and included in this study: grade I in 15 patients, II in 9 patients, and III in 5 patients.. Table 1. Failures of non-operative management. ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Sex/ AAST Days to Case MOI* Repeat CT scan † Age grade failure ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 1 M/38 MVC‡ II 2 active bleeding 2 M/37 MVC I 1 active bleeding 3 M/64 ped-struck§ III 1 increased hematoma 4 M/54 ped-struck I 7 pseudoaneurysm 5 M/35 MVC I 14 pseudoaneurysm ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ *MOI = mechanism of injury; †AAST grade = american association for the surgery of trauma organ injury scale-spleen according to the initial CT findings; ‡MVC = motor vehicle crach; § ped-struck = pedestrian struck.. A. RESULTS. In the 29 patients managed non-operatively, repeat CT scan was obtained to document improvement or progression of injury within 7 days after admission: improvement of injury in 24 patients and progression of injury in 5 patients. Twenty-four patients (82.8%) with improvement of injury on follow-up CT scan successfully managed non-operatively (Fig. 2), and clinical outcome was good. However, the other 5 patients (17.2%) with progression of injury on followup CT scan failed non-operative management, and immediate surgery was mandated (Table 1). Of these 5 patients failed non-operative management, 3 patients failed because of a combination of change in clinical status (unstable vital signs and/or decreased hemoglobin levels) and worsening appearance on repeat CT scan (Fig. 3), and the other 2 patients were deemed failures because of the delayed development of splenic artery pseudoaneurysms on CT scan (Fig. 4). The failures of non-operative management occurred 1 to 14 days after the initial CT scan. In this study, the delayed development of posttraumatic splenic artery pseudoaneurysms occurred in 2 patients (6.9%). The first case was a 54-year-old male who was referred for evaluation and management of blunt trauma associated with pedestrian struck. Initial CT scan exhibited spleen and liver. B. Fig. 3. CT scans of one representative patient failed non-operative management because of change in clinical status. (A) Initial CT scan showed spleen contusion with intraparenchymal hematoma about 4-cm sized in medial portion of spleen. Note a contrast blush in intraparenchymal hematoma. (B) Follow-up CT scan on day 1 showed increased perisplenic hematoma, and emergent splenectomy was performed..
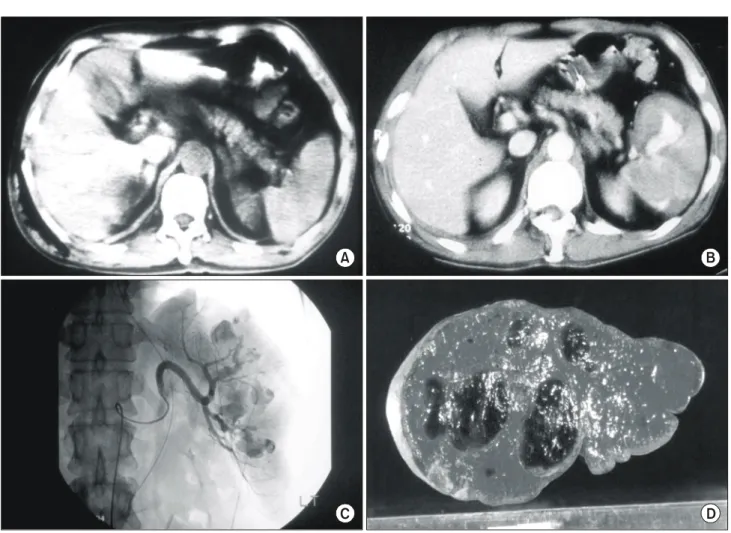
(4) Yong Pil Cho, et al:Repeat CT Scan for Non-operative Management of Blunt Splenic Trauma. 393. ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ. A. B. C. D. Fig. 4. CT scans of one representative patient failed non-operative management because of the delayed development of posttraumatic splenic artery pseudoaneurysm. (A) Initial CT scan showed spleen and liver contusion without evidence of intraperitoneal fluid collection. (B) Follow-up CT scan on day 7 showed splenomegaly with the delayed development of multiple intrasplenic pseudoaneurysms. (C) Selective celiac arteriogram showed multiple intrasplenic pseudoaneurysms. (D) Serial section of operative specimen showed multiple intrasplenic pseudoaneurysms measuring up to 4.5 cm in diameter.. contusion without evidence of intraperitoneal fluid collection. Non-operative management was done because the patient was clinically stable with no evidence of other intra-abdominal organ injuries. Follow-up CT scan on day 7 showed splenomegaly with the delayed development of multiple intrasplenic pseudoaneurysms with about 4.5-cm in maximal diameter. The second case was a 35-yearold male who was referred for evaluation and management of blunt trauma associated with motor vehicle crashes. Initial CT scan exhibited left perinephric hematoma without evidence of intraperitoneal fluid collection. Non-operative management was done because the patient was clinically stable with no evidence of other intra-abdominal organ injuries. Follow-up CT scan on day 3 showed no significant. interval change of left perinephric hematoma. However, an additional follow-up CT scan obtained on day 14 demonstrated the delayed development of large posttraumatic splenic artery pseudoaneurysm with about 6-cm in maximal diameter. In these 2 cases, splenectomy was performed because of failed transarterial embolization and the high risk of delayed splenic rupture. These patients were discharged without complications. In this study, there were no missed intra-abdominal injuries, and no patient developed a delayed rupture. Repeat CT scan is accurate in estimating the severity of blunt splenic injury and provides a valuable clinical information in non-operative management to document improvement or progression of injury..
(5) 394. 대한외과학회지:제 67 권 제 5 호 2004. ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ. DISCUSSION. The spleen is the most commonly injured organ in blunt abdominal trauma. In parallel with the increased blunt trauma associated with motor vehicle crashes, splenic injuries have been increased in recent years. The management of splenic injury has continued to evolve over the past century. The trend has been increasingly toward avoiding splenectomy in favor of splenic preservation, either operatively or non-operatively. Many splenic injuries are without active bleeding and require no treatment at laparotomy. This important fact leads to the concept of non-operative management in clinically stable patients with blunt splenic trauma. It developed as an extension of splenic salvage techniques in children and has been successfully adapted to adults.(11,12) Non-operative management is now the standard of care for low-grade, isolated blunt splenic injuries in stable patients, and has enabled many patients to avoid a laparotomy after blunt abdominal trauma. The most important criterion for the non-operative management of splenic injury is that the patient be clinically stable.(13) There should be no evidence of persistent hypovolemia and hypotension. There should also be no evidence of other intra-abdominal organ injuries. When non-operative management is selected, isolated splenic injury must be confirmed by some types of diagnostic imaging studies, most commonly an abdominal CT scan. However, potential disadvantages of non-operative management have included failure rates of 10 to 40%.(5,6) Those at particular risk include patients older than 55, with an ISS (Injury Severity Score) greater than 15 to 20, or in the multiply injured patient.(5,10-16) Other criticisms include the fact that many patients who fail non-operative management will require splenectomy, whereas earlier operation would have allowed splenorrhaphy and reduced the risk of overwhelming postsplenectomy sepsis.(16) There is also a potential risk of these patients developing delayed rupture or requiring greater transfusion of red blood cells than those undergoing early operation. There is also a risk of missing other significant intra-abdominal injuries.(6,17) CT scan plays an important role in the evaluation. of abdominal trauma.(4,18-22) Under optimal conditions, lesions to the parenchyma of solid organs and the extravasation of blood are detected with high accuracy in CT scans. Splenic injuries, as detected on CT scan, include contusion, laceration, subcapsular or intraparenchymal hematoma, vascular pedicle injury, pseudoaneurysms, and active bleeding. CT scans with excellent splenic enhancement are at least 98% sensitive to injury when optimally performed and interpreted.(23) Spleens showing superficial laceration or small contusions with minimal free blood are likely to heal without surgical intervention, while severely lacerated spleens with substantial intraperitoneal blood will require urgent surgical intervention. However, the predictive value of CT grading of splenic injury provides limited value in predicting non-operative outcome for a given patient.(24-26) Some factors that clearly predict a poor outcome for non-operative management include demonstration of active bleeding, pseudoaneurysms, and severe maceration.(26,27) Schurr and associates have shown the presence of a vascular blush on CT scan, indicative of splenic pseudoaneurysm, to be a strong prediction of failure in patients managed non-operatively.(26) The need to repeat a CT scan of the spleen after the initial diagnosis of injury and non-operative management without a clear clinical indication is controversial. Although some studies have shown no particular value, others strongly advocate repeat CT scan prior to discharge.(7-9) Some have noted the delayed development of pseudoaneurysm formation and progression of injury on follow-up CT scan of the spleen in several cases without a clear clinical indication and, therefore, recommend repeat CT scan at 3 to 7 days or prior to discharge to document healing or progression of injury.(9,24) In this study, of the 29 patients initially managed non-operatively, 5 patients (17.2%) failed this approach: 3 presented with the progressive deterioration of the clinical status, and 2 did not. In all 5 patients, repeat CT scan revealed the deteriorating appearance of the splenic injury: active bleeding or increased hematoma in 3 patients and splenic artery pseudoaneurysms in the others. In cases with signs and symptoms of continued bleeding, repeat CT scan is accurate in estimating the severity of splenic injury.
(6) Yong Pil Cho, et al:Repeat CT Scan for Non-operative Management of Blunt Splenic Trauma. 395. ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ. and can reduce the risk of missing significant intra-abdominal injuries even though therapeutic intervention may be delayed. In cases with the delayed development of posttraumatic pseudoaneurysms of the splenic artery, repeat CT scan is an excellent tool to furnish a rapid precise diagnosis and to allow earlier laparotomy prior to delayed rupture. CT scan has been established as an accurate method for detection and characterization of splenic injuries, either in the acute phase or in various stages of healing. However, any CT scan is merely a "snapshot" of the patient's anatomy at that time; only interval scanning or clinical monitoring can determine ongoing hemorrhage or progressive healing.(8) In some patients, "mild" splenic injuries detected on CT scan subsequently hemorrhage again and may require urgent surgery, whereas in many patients, "severe" splenic injuries do well with non-operative management. CT scan is an excellent tool to depict morphologic features but is limited in its capacity to demonstrate physiologic features.(8) Considering that 8∼29% of adults with blunt splenic trauma managed non-operatively have repeat hemorrhage that requires urgent surgery, and the bleeding may be delayed by hours to weeks,(12,28) repeat CT scan after blunt trauma may be an important diagnostic tool in predicting non-operative outcome in the patient who is deemed clinically stable and does not have other injuries requiring immediate diagnostic and therapeutic intervention. CONCLUSION. Repeat CT scan for the non-operative management of blunt splenic trauma requires further evaluation with full clinical study and this presentation shows only the initial experience of this diagnostic modality to provide a valuable clinical information in diagnosis and management of splenic injury to document healing or progression of injury, even though some studies have shown no particular value.. 3). 4) 5). 6). 7) 8) 9). 10). 11) 12). 13). 14). 15). 16). 17). 18). REFERENCES 19) 1) Wolfman NT, Bechtold RE, Scharling ES, Meredith JW. Blunt upper abdominal trauma: evaluation by CT. Am J Roentgenol 1992;158:493-501. 2) Tom WW, Howells GA, Bree RL, Schwab R, Lucas RJ. A. 20). nonoperative approach to the adult ruptured spleen sustained from blunt trauma. Am Surg 1985;51:367-71. Stivelman RL, Glaubitz JP, Crampton RS. Laceration of the spleen due to nonpenetrating trauma: one hundred cases. Am J Surg 1963;106:888-91. Federle MP, Griffiths B, Minagi H, Jeffrey RB Jr. Splenic trauma: evaluation with CT. Radiology 1987;162:69-71. Smith JS Jr, Wengrovitz MA, DeLong BS. Prospective validation of criteria, including age, for safe, nonsurgical management of the ruptured spleen. J Trauma 1992;33: 363-9. Cogbill TH, Moore EE, Jurkovich GJ, Morris JA, Mucha P Jr, Shackford SR, et al. Nonoperative management of blunt splenic trauma: a multicenter experience. J Trauma 1989; 29:1312-7. Lawson DE, Jacobson JA, Spizarny DL, Pranicoff T. Splenic trauma: value of follow-up CT. Radiology 1995;194:97-100. Federle MP. Splenic trauma: is follow-up CT of value? Radiology 1995;194:23-4. Park EH, Cho YP, Jang HJ, Kim YH, Han MS. Delayed splenic artery aneurysm after blunt trauma. J Korean Surg Soc 2003;65:251-3. Moore EE, Shackford SR, Pachter HL, McAninch JW, Browner BD, Champion HR, et al. Organ injury scaling: spleen, liver, and kidney. J Trauma 1989;29:1664-6. Upadhyaya P, Simpson JS. Splenic trauma in children. Surg Gynecol Obstet 1968;126:781-90. Longo WE, Baker CC, McMillen MA, Modlin IM, Degutis LC, Zucker KA. Nonoperative management of adult blunt splenic trauma. Criteria for successful outcome. Ann Surg 1989;210:626-9. Esposito TJ, Gamelli RL. Injury to the spleen. In: Mattox KL, Feliciano DV, Moore EE, editors. Trauma. 4th ed. New York: McGraw-Hill; 2000. p.683-711. Elmore JR, Clark DE, Isler RJ, Horner WR. Selective nonoperative management of blunt splenic trauma in adults. Arch Surg 1989;124:581-6. Kohn JS, Clark DE, Isler RJ, Pope CF. Is computed tomographic grading of splenic injury useful in the nonsurgical management of blunt trauma? J Trauma 1994;36:385-9. Rappaport W, McIntyre KE Jr, Carmona R. The management of splenic trauma in the adult patient with blunt multiple injuries. Surg Gynecol Obstet 1990;170:204-8. Kluger Y, Paul DB, Raves JJ, Fonda M, Young JC, Townsend RN, et al. Delayed rupture of the spleen--myths, facts, and their importance: case reports and literature review. J Trauma 1994;36:568-71. Federle MP, Crass RA, Jeffrey RB, Trunkey DD. Computed tomography in blunt abdominal trauma. Arch Surg 1982;117: 645-50. Jeffrey RB, Laing FC, Federle MP, Goodman PC. Computed tomography of splenic trauma. Radiology 1981;141:729-32. Goldstein AS, Sclafani SJ, Kupferstein NH, Bass I, Lewis T, Panetta T, et al. The diagnostic superiority of computerized tomography. J Trauma 1985;25:938-46..
(7) 396. 대한외과학회지:제 67 권 제 5 호 2004. ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 21) Meredith JW, Trunkey DD. CT scanning in acute abdominal injuries. Surg Clin North Am 1988;68:255-68. 22) Phillips T, Sclafani SJ, Goldstein A, Scalea T, Panetta T, Shaftan G. Use of the contrast-enhanced CT enema in the management of penetrating trauma to the flank and back. J Trauma 1986;26:593-601. 23) Wing VW, Federle MP, Morris JA Jr, Jeffrey RB, Bluth R. The clinical impact of CT for blunt abdominal trauma. Am J Roentgenol 1985;145:1191-4. 24) Mirvis SE, Whitley NO, Gens DR. Blunt splenic trauma in adults: CT-based classification and correlation with prognosis and treatment. Radiology 1989;171:33-9. 25) Sutyak JP, Chiu WC, D'Amelio LF, Amorosa JK, Hammond. JS. Computed tomography is inaccurate in estimating the severity of adult splenic injury. J Trauma 1995;39:514-8. 26) Schurr MJ, Fabian TC, Gavant MD, Croce MA, Kudsk KA, Minard G, et al. Management of blunt splenic trauma: computed tomographic contrast blush predicts failure of nonoperative management. J Trauma 1995;39:507-12. 27) Federle MP, Courcoulas AP, Powell M, Ferris JV, Peitzman AB. Blunt splenic injury in adults: clinical and CT criteria for management with emphasis on active extravasation. Radiology 1998;206:137-42. 28) Mucha P, Daly RC, Farnell MB. Selective management of blunt splenic trauma. J Trauma 1986;26:970-4..
(8)
수치
관련 문서
The ATmega48PA/88PA/168PA/328P provides the following features: 4/8/16/32K bytes of In- System Programmable Flash with Read-While-Write capabilities, 256/512/512/1K
Additional reasons which may result in the termination of the development, launch or operation of the Platform includes, but is not limited to, (aa) an unfavorable fluctuation
Blunt ends DNA containing restriction enzyme
• Oxygen dissolved in water (DO) is important for many forms of aquatic life. • From Henry’s Law, the DO concentration in air-saturated water is 8 to 15 mg/L depending
– To assist the Engineered Safety Features System by assuring that there is sufficient time for actuating the auxiliary feedwater pumps to remove decay heat from the reactor
Adsorptive capacity of THM according to repeat use of clay ball Unit: ㎍ THM/g clay, Blank: Reduction or increase amount.. Adsorptive capacity of THM according to repeat use
– To assist the Engineered Safety Features System by assuring that there is sufficient time for actuating the auxiliary feedwater pumps to remove decay heat from the reactor
Kernel 1, which has an arithmetic intensity of 0.5 FLOPs/byte, is limited by memory bandwidth to no more than 8 GFLOPS/sec. Kernel 2, which has an arithmetic intensity of
