선천적 결손이나 치주질환으로 인해 상실된 치아를 수복하 기 위해 골유착성 치과 임플란트가 폭넓게 사용되고 있다. 특 히 치주질환으로 인하여 상악 구치부에서 치아를 상실한 후 에는 무치악 치조제의 흡수가 발생하여 치조골의 수직적 높 이와 폭의 감소뿐만 아니라 점진적인 상악동의 함기화로 인 하여 더욱 치조제를 상실하게 된다. 현재는 이와 같이 잔존 치
조골의 높이가 불충분한 경우 상악동 거상술을 시행함으로써 임플란트를 식립할 수 있게 되었다. 상악동 거상술은 1976년 Tatum이 처음으로 보고하였고, 이후 Boyne과 James [1]가 상 악 측벽을 제거하고 상악동 점막을 거상한 후 골결손부를 통 해 골이식을 시행하는 측방접근법을 보고하였다. 이후 임플 란트 식립을 위한 많은 변형된 상악동 거상술이 시행되었다 [2-4]. 상악동 거상술을 동반한 임플란트 식립 후의 성공률을 보면, Peleg 등[5]은 2,132개의 임플란트를 식립했을 때 97.9%
의 9년 누적성공률을 보고하였고, Zinser 등[6]은 1,045개의 임 플란트에서 93.3%의 14년 누적성공률을 보고하였다.
상악동 거상술을 시행함에 있어서 상악동 점막의 천공, 출 혈, 비구강 개통, 상악동염 등의 합병증이 일어날 수 있다. 그
상악동 중격 존재 시 상악동 거상술: 증례보고
정명진2,3ㆍ김병옥1,*
조선대학교 치의학전문대학원 1치주과학교실, 2치의생명공학과, 3연변대학교부속병원 구강과
Sinus lifting procedures in the presence of the maxillary sinus septa: Case report
Ming-Zhen Zheng2,3, Byung-Ock Kim1,*
Departments of
1Periodontology,
2Biodental Engineering, School of Dentistry, Chosun University, Gwangju, Korea,
3
Department of Stomatology, The Affiliated Hospital of Yanbian University, Yanji, China
ABSTRACT
The presence of septa in the region of the sinus floor can cause complications during sinus lift procedures; accordingly, it is necessary to identify the sinus septa prior to the operative procedure. Various treatment options have been described for management of septa. This study described three cases of lateral window approach for maxillary sinus bone graft in the presence of sinus septa. Panoramic radiograph and dental cone-beam computed tomographic scans were obtained preoperatively. In the first and third case, two bony windows were created after infracture, while in one case the septal bone was cut off and in the other it was left intact. In the second case, one bony window was prepared and the sharp tip of the septum was reduced. After treatment, all of the cases achieved sufficient bone height and no membrane perforation occurred. Modification of the basic sinus lateral approach is a predictable technique to increase bone volume of the edentulous posterior maxilla; therefore, it can be used for placement of dental implants.
Key Words: Sinus lift, Sinus septa, Lateral approach technique
Received Aug 19, 2013; Revised version received Sep 2, 2013 Accepted Sep 2, 2013
Corresponding author: Byung-Ock Kim
Department of Periodontology, School of Dentistry, Chosun University, 309 Pilmun-daero, Dong-gu, Gwangju 501-759, Korea Tel: 82-62-220-3850, Fax: 82-62-224-4664
E-mail: [email protected]
중 가장 흔한 합병증은 Schneiderian 막의 천공으로 상악동 거상술 실패 원인의 48%를 차지한다는 보고가 있다[7]. 이런 Schneiderian 막의 천공을 일으키는 가장 큰 해부학적 장애가 상악동 중격이다. 상악동 중격은 1910년 Underwood [8]에 의 해 처음 보고되었으며 Underwood’s septum이라고 명명되기도 한다. 상악동 중격은 경우에 따라 상악동 바닥과 내벽에 존재 하며 모양은 주로 inverted gothic arch 형태이다. 이러한 상악동 중격은 상악동을 두 개 혹은 그 이상의 구획으로 완전히 혹은 부분적으로 나눈다. 상악동 중격의 발생빈도에 관한 연구를 보 면, Underwood [8]는 해부학적 연구에서 33%의 발생빈도를 보 고하였고, Pommer 등[9]은 메타분석을 통해 28.4%의 환자에서 상악동 중격의 존재율을 보고하였다. 상악동 중격의 위치에 관 한 연구를 보면, Krennmair 등[10]의 보고에 의하면 대부분의 상악동 중격이 상악 소구치부위에 75% 정도가 존재한다고 하 였고, Underwood [8]는 대부분이 후방부에 존재한다고 보고하 였다. 상악동 중격의 높이에 관한 연구를 보면, Pommer 등[9]
은 리뷰 논문에서 중격의 평균 높이가 7.5 mm라고 보고하였다.
상악동 중격의 존재는 측방접근법으로 상악동 거상술을 시 행할 때 측벽에 골창(bony window) 형성을 제한하거나 상악 동 내에 이식재를 충분히 충전하지 못하게 할 수 있으며 적절 한 수술시야의 확보를 방해하기도 한다. 또한 상악동 중격에 Schneiderian 막이 강하게 부착되어 상악동 거상술을 시행할
때 막의 천공 위험성을 직접적으로 증가시킨다.
이 연구의 목적은 상악동 중격 존재 시에 여러 가지 술식을 이용한 상악동 내 골이식을 시행하였던 3편의 증례를 소개하 고자 한다.
증례보고
증례1
63세 남자 환자로 상악 우측 후방의 무치악 부위에 임플란트 를 식립하고 싶다는 주소로 내원하였다. 전신질환은 없으며 약 3년 전 상악 우측 대구치를 발거하였고, 그동안 어떠한 보철치 료도 하지 않았다. 파노라마 방사선 사진상에서 상악 우측 대 구치부위의 치조골정부터 상악동저까지의 골높이를 측정하였 을때 약 2-3 mm로 상악동 골이식이 필요한 것으로 진단되었으 며 상악 우측에 협-구개측 방향으로 주행하는 1개의 중격이 보 였다(Fig. 1A). 국소마취하에 치조정 절개, 제1소구치 원심면에 서 수직절개를 시행하여 전층판막을 거상하였다. 파노라마 사 진을 참고하면서 측방벽에 상악동 중격이 있는 부위를 중심으 로 양쪽에 2개의 골창을 형성하였다. 골창을 형성한 후 외측골 은 Schneiderian 막과 함께 조심스럽게 거상한 뒤, bone rongeur 를 이용하여 상악동 중격을 제거하였다(Fig. 1B). 제거된 중격 골은 분쇄하여 합성골인 MBCP (Biomatlante Sari, Bretagne,
Fig. 1. (A) Preoperative panoramic radiograph demonstrat-
ing a septum in the right maxillary sinus (short arrows). (B)
View of the sinus cavity through the two bony windows after
infracture and cutting the septal bone and elevation of the
Schneiderian membrane. (C) Postoperative panoramic ra-
diograph following sinus augmentation with the bone graft-
ing demonstrated with circle.
France)와 동종골인 ICB (Rocky Mountain Tissue Bank, Denver, CO, USA)를 섞은 이식재와 함께 상악동 내에 채워 넣고 골창 은 비흡수성 차폐막인 PTFE membrane (TefGenTM; Lifecore Dental, St. Paul, MN, USA)을 이용하여 폐쇄한 후 봉합하였다.
술 후 파노라마 사진상 술 전과 비교하여 충분한 골이식재가 충전된 것을 볼 수 있었다(Fig. 1C).
증례2
37세 남자 환자로 발치된 상악 제1, 2대구치 부위에 임플란 트를 식립하고 싶다는 주소로 내원하였다. 전신질환은 없으 며 약 1년 전 심한 치주염으로 상악 좌측 제1대구치를 발거하 였다. 파노라마 방사선 사진상 상악 좌측에 상악동 골이식이 필요한 것으로 진단되었으며 상악동 좌측에 1개의 중격이 보 였다. 정밀한 진단을 위해 3차원 컴퓨터 단층촬영(computed tomography, CT) (CBMercuRayTM; Hitachi, Tokyo, Japan) 결 과 상악 좌측 제1, 2대구치 임플란트 식립 부위의 치조골정부 터 상악동저까지의 잔존골 높이가 각각 1.8 mm, 2.2 mm였으 며 협-구개 방향으로 주행하는 1개의 중격이 존재하였다(Fig.
2A). 국소마취하에 치조정 절개와 제1소구치 원심면에 수직절 개를 시행하여 전층판막을 거상하였다. 중격이 있는 부위의 직
전까지 골창을 형성하고 외측골은 Schneiderian 막에서 완전히 분리하여 생리식염수에 보관하였다. Schneiderian 막을 조심 스럽게 거상하여 중격을 완전히 노출시킨 후 chisel과 mallet을 이용하여 중격을 골절시켜 조금 더 거상시켰다. 그 후 Kerrison rongeur (G. HARTZELL & SON, Concord, CA, USA)를 이용 하여 골창을 더 확대하였다(Fig. 2B). 상악동 내에는 이종골 인 Bio-Oss® (Geistlich-Pharma AG, Wolhusen, Sweitzerland)와 동종골인 TutoplastTM (Tutogen Medical GmbH, Neunkirchen, Germany)를 1 : 1로 섞은 이식재를 채워 넣고 다시 자가골편을 외측벽에 위치시킨 후 흡수성 차폐막인 Bio-Gide® (Geistlich- Pharma AG)를 이용하여 폐쇄한 후 봉합하였다. 상악동 거상술 후 파노라마 방사선사진에서 임플란트 식립에 충분한 골이식 이 이루어진 것을 볼 수 있다(Fig. 2C).
증례3
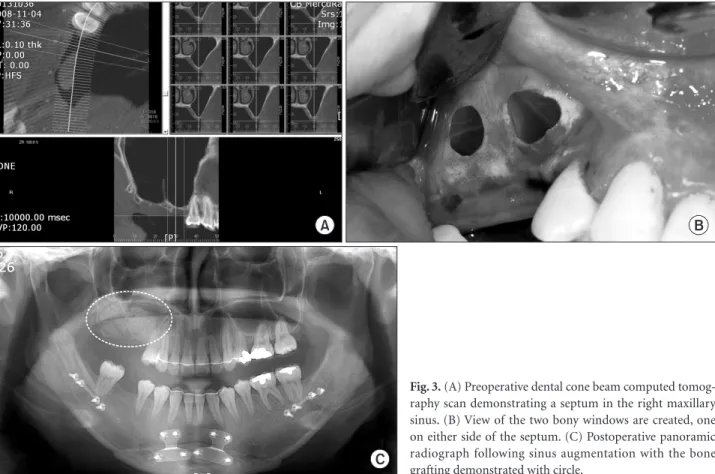
23세 여자 환자로 전반적으로 교정치료하면서 상악 우측 후 방의 무치악 부위에 임플란트를 식립하고 싶다는 주소로 내원 하였다. 전신질환은 없었으며 약 3년 전 상악 우측 제2소구치, 제1대구치와 제2대구치를 발거하였다. 파노라마 방사선 사진 상 상악 우측에 상악동 골이식이 필요한 것으로 진단되었으며
Fig. 2. (A) Preoperative dental cone beam computed to-
mography scan demonstrating a septum in the left maxil-
lary sinus. (B) One bony window was prepared after green-
stick fracture (demonstrated with circle) and the sharp tip
of the septum was reduced. (C) Postoperative panoramic
radiograph following sinus augmentation with the bone
grafting demonstrated with circle.
상악동 우측에 1개의 중격이 보였다. 정밀한 진단을 위해 3차 원 CT (CBMercuRayTM) 결과 상악 우측 구치부 임플란트 식립 부위의 치조골정부터 상악동저까지의 잔존골 높이가 약 0.8 내지 1 mm였으며 협-구개 방향으로 주행하는 1개의 중격이 존재하였다(Fig. 3A). 국소마취 후 상악결절로부터 제1 소구 치의 근심면까지 치조정 수평절개와 열구절개, 그리고 충분한 협측 수직절개를 시행하여 전층판막을 거상하였다. 상악동 측 벽에서 중격이 존재하는 양측에 2개의 골창을 형성한 후 각각 2개의 창으로 조심스럽게 Schneiderian 막을 천공 없이 거상 하였다(Fig. 3B). 상악동 중격은 제거하지 않았으며 이종골인 Bio-Oss®와 동종골인 TutoplastTM를 1 : 1로 섞은 이식재를 상악 동 내에 채워 넣고 다시 자가골편을 외측벽에 위치시킨 후 흡 수성 차폐막인 Bio-Gide®를 이용하여 골창을 폐쇄한 후 봉합 하였다. 수술 후 파노라마 방사선 사진상 충분한 골이식이 이 루어진 것을 관찰할 수 있다(Fig. 3C).
고 찰
상악동 거상술이 도입된 이후로 상악 구치부에서 골량이 불 충분한 경우에도 골이식을 통해 임플란트를 식립할 수 있게
되었다. 상악동 골이식술에서 상악동 중격의 존재는 상악동 거상술을 어렵게 한다.
상악동 중격의 발생기전에 대해 여러 이론이 제시되고 있 다. Underwood [8]는 중격이 치아 간의 맹출시기의 차이에 기 인한다고 하였고, Krennmair 등[10]은 상악동 중격을 1차 중 격과 2차 중격으로 구분하였는데 1차 중격은 상악동의 발생 과 함께 발생하는 선천적인 중격이며 2차 중격은 치아 상실을 동반한 상악동 하방벽의 불규칙한 함기화에 의해 형성된 중 격이라고 하였다.
Ulm 등[11]은 무치악 상악골에 대한 연구에서 소구치부는 대구치보다 오랫동안 잔존하고 대구치부는 치아 상실과 함께 지속적으로 함기화가 일어나기 때문에 소구치부에서 2차 중 격이 많이 발생되게 되고 상악동 중격의 발생률이 높다고 보 고하였다. 그러나 Krennmair [12]는 인접한 상악 구치 사이에 잔존 치근간 골로부터 생기는 후방 부위에서 2차 중격인 상악 동 중격이 높은 발생률을 보인다고 보고하였고, Underwood [8]도 관찰된 대부분의 중격은 후방 부분에 위치했다고 밝혔 다. 본 논문에서는 세 증례 모두 상악 제1, 2대구치 부위에서 상악동 중격이 존재하였으며 중격의 높이는 각각 12 mm, 8.5 mm, 그리고 13.7 mm로 측정되었다.
Fig. 3. (A) Preoperative dental cone beam computed tomog-
raphy scan demonstrating a septum in the right maxillary
sinus. (B) View of the two bony windows are created, one
on either side of the septum. (C) Postoperative panoramic
radiograph following sinus augmentation with the bone
grafting demonstrated with circle.
술 전에 상악동 중격의 존재를 발견하지 못하게 된다면 상 악동 거상술 시 중격으로 인해 측벽의 부적절한 골절, 골창 거 상의 어려움, Schneiderian 막의 천공, 상악동 내 시야방해, 상 악동 내로 이식재의 부적절한 충전 등을 유발할 수 있으므로 반드시 중격의 존재 여부를 술 전에 확인하여야 한다. 상악동 중격을 평가하는 방법에는 치근단 방사선 사진, 파노라마 방 사선 사진, CT 사진, 수술 중 직접 측정하는 방법 등이 있는데 CT를 이용하면 상악동 중격을 포함한 상악동 내의 미세한 해 부학적 구조물을 관찰할 수 있을 뿐만 아니라 상악동염 등 병 적인 상태를 쉽게 발견할 수 있으므로 상악동 거상술을 시행 하기 전에 술 전 CT 사진을 촬영하는 것을 추천한다[13,14]. 반 면 파노라마 방사선 사진은 CT에 비해 경제적이고 전반적인 해부학적 구조를 보여주며 사용하기 용이하지만 중첩효과, 상의 왜곡과 불규칙한 확대율로 인해서 상대적으로 정확한 정보를 제공하지 못한다[15,16]. Krennmair 등[10]은 파노라 마 상에서 상악동 중격 검사 시 21.3% 정도 위양성/위음성으 로 잘못된 진단을 할 수 있다고 하였다. Lee 등[17]의 논문에서 는 총 130개의 중격에 대한 파노라마와 cone beam computed tomography (CBCT)로 측정한 결과 85개만 정확하였으며 정 확도는 65%라고 보고하였다. 본 논문의 증례 1에서는 파노라 마 방사선 사진만으로 상악동 중격을 관찰하였으며, 증례 2와 3에서는 파노라마 방사선 사진과 CBCT를 이용하여 여러 방 향에서 관찰 후 상악동 중격의 주행 방향을 진단할 수 있었다.
Ulm 등[11]은 모든 중격은 전두측 방향이나 이방향과 유사하 게 협-구개측으로 주행하며 치열궁에 평행한 시상측 방향은 관찰되지 않았으며 중격의 기시부위가 중간부보다 두드러지 게 높고 넓다고 하였다. Oh와 Rhy [18]는 448명 환자의 CT를 통하여 협-구개형이 157개(86.3%)로 대부분을 차지하고 시상 형이 16개(8.8%), 횡단형이 9개(4.9%)로 관찰되었다고 보고하 였다. 본 논문에서는 세 증례 모두 수직적으로 존재하는 협-구 개형 중격이였다.
Chanavaz [19]와 Tatum [2]은 상악동 거상 시 중격의 존재 로 시야 확보가 어렵게 하고 막이 중격에 강하게 부착되기에 거상이 어렵고 천공 위험이 증가한다고 하였다. 이러한 상악 동 중격을 고려한 상악동 거상 수술 방법으로는 중격을 적극 적으로 제거하는 방법과 중격을 피하여 수술하는 방법으로 나눈다[20]. Boyne과 James [1]는 중격을 chisel로 절단한 후 제 거하는 방법을 보고하였고, Van der Bergh 등[21]은 크고 높 은 중격으로 인해 나누어진 상악동에서 중격을 경계로 두 개 의 분리된 골창을 열어서 따로 상악동 점막을 형성하고 높이 가 낮거나 날카로운 중격의 경우에는 중격을 절단하거나 W 자 형태의 골창을 형성하는 상악동 거상술을 추천하였다. 본 논문의 증례 1에서는 중격이 높지만 얇기 때문에 먼저 측방벽
에 2개의 골창을 형성한 후 bone rongeur를 이용하여 상악동 중격을 제거하였다. 증례 3에서도 마찬가지로 중격이 높은 동 시에 내측으로 가면서 두꺼웠기 때문에 상악동 중격을 중심 으로 독립된 2개의 골창을 형성한 후 막을 각각 거상하여 이식 재를 채워 넣었다. 증례 2에서는 중격의 높이가 낮았기 때문 에 먼저 중격 직전까지 골창을 형성한 후 막을 중격에서 충분 히 분리시킨 후 중격을 제거하였다. Zijderveld 등[22]은 48%
의 환자에서 중격의 존재로 인해 Tatum 방식의 시술이 어려 웠다고 보고하면서 변형된 시술을 시행한 5%의 경우에도 중 격의 위치에서 Schneiderian 막의 천공이 발생하였다고 하였 다. Schneiderian 막의 두께는 약 0.13 mm 내지 0.5 mm로 매우 얇고 약하기 때문에 쉽게 천공될 수 있다[23]. 특히 중격의 상 방 경계부위에서 천공의 위험이 높으며 막 거상 시 2 mm 이하 의 천공은 혈병에 의해 자연치유가 가능하지만 3 mm 이상의 천공은 콜라겐막을 사용하여 천공부위를 막은 다음 골이식을 고려해 보아야 한다. 본 논문의 세 증례 모두 Schneiderian 막 거상 시 천공이 발생하지 않았으며 술 후 파노라마 방사선 사 진상 충분한 골이식이 이루어진 것을 관찰할 수 있었다. 상악 동 중격은 파노라마 방사선 사진으로는 정확한 진단이 어려 우므로 오진단이 의심되는 경우 정밀한 치과용 CBCT를 이용 해 정확한 해부학적 구조물을 파악하여 상악동 거상술 전 중 격의 위치나 형태를 고려하여 중격에 대한 정확한 치료 계획 을 세움으로써 시술 시 합병증이 발생하지 않도록 해야 한다.
참고문헌