DOI : 10.3341/jkos.2009.50.6.877
= 증례보고 = 접수번호 : 50-06-10-10
큰 망막색소상피 박리를 동반한 맥락막혈관신생에서의 복합치료
류정완⋅정재훈⋅이원기
가톨릭대학교 의과대학 안과 및 시과학교실
목적: 큰 망막색소상피박리(PED)를 동반한 신생혈관 나이관련황반변성에서 유리체강내 bevacizumab 주사와 광역학요법(PDT)의 복 합치료 효과를 알아보았다.
대상과 방법: 맥락막혈관신생으로 진단된 9안, 맥락막혈관신생과 결절맥락막혈관병증 사이에 진단이 모호한 4안, 총 13안을 대상으로 하였다. Bevacizumab 주사 후 1주일 이내에 인도시아닌형광안저혈관조영에 따른 PDT를 시행하였다. 추가적인 주사는 4~6주, 추가적인 PDT는 늦어도 4개월 간격으로 시행하였다.
결과: 최종 검사 때 시력변화는 호전 3안(23.1%), 유지 7안(53.8%), 악화 3안(23.1%)이었다. PED의 변화는 소실 5안(38.5%), 소실 후 재발 2안(15.4%), 지속 4안(30.8%), 망막색소상피 파열이 2안(15.4%)이었다. 맥락막혈관신생 군은 66.7%(6/9), 진단이 모호한 군은 100% (4/4)에서 시력이 유지되거나 향상되었다.
결론: 큰 망막색소상피박리를 동반한 신생혈관 나이관련황반변성에서 복합치료는 시력유지 및 호전을 기대할 수 있는 선택적인 치료 방법이다. 추후 장기간의 관찰과 항 혈관내피성장인자 항체의 단일치료와 대조연구가 필요하다.
<대한안과학회지 2009:50(6):877-886>
■ 접 수 일: 2008년 10월 14일 ■ 심사통과일: 2009년 3월 25일
■ 통 신 저 자: 이 원 기
서울특별시 서초구 반포동 505
가톨릭대학교 의과대학 서울성모병원 안과 Tel: 02-2258-2846, Fax: 02-590-7405 E-mail: [email protected]
* 본 논문의 요지는 2008년 대한안과학회 제99회 춘계학술대회에서 구연으로 발표되었음.
삼출성 나이관련황반변성은 맥락막혈관신생과 혈관 누출 을 특징으로 하는 질환으로 염증반응과 혈관내피성장인자 (vascular endothelial growth factor, VEGF)의 활성화가 중요한 자극 요인이다.1-4치료의 선택에 있어서도 맥락막혈 관신생의 직접적인 폐쇄 뿐 아니라 염증반응과 VEGF의 발 현이 동시에 억제된다면 보다 효과적일 것이다. 이는 신생 혈관 발생에 있어서 각기 다른 요인을 차단하여 치료의 상 승효과를 기대할 수 있는 복합치료의 근거가 된다.5-11
항 혈관내피성장인자 항체(anti-VEGF antibody)인 약 제들은 VEGF의 조절을 통해 혈관 투과성 감소와 혈관신생을 억제하는 효과가 있다.12,13이와 달리 광역학요법(photodynamic therapy, PDT)은 신생혈관 내에 혈전을 형성하여 신생혈 관을 폐쇄시킨다.14그러나 레이저 조사부위에 포함된 정상 맥락막모세혈관에도 일시적인 폐쇄를 유발한다. 이에 따르는 맥락막 허혈은 VEGF의 분비를 유발하여, 역설적으로 폐쇄된 신생혈관의 재발 및 증식을 일으킬 수 있다.15이런 이유로 항 혈관내피성장인자 항체가 갖는 VEGF의 발현을 억제할 수 있는 효과와 광역학요법이 병용된다면 광역학요법으로
인한 기대하지 않는 2차 효과를 상쇄시킬 수 있고, 보다 강 력한 혈관신생 억제를 통한 장기적인 효과와 치료 횟수를 줄일 수 있을 것으로 기대된다.8-11,16
이에 본 연구에서 복합치료의 순서는 bevacizumab을 먼 저 주입하고, 이어서 7일 이내에 광역학요법을 시행하였다.
이는 큰 망막색소상피박리(pigment epithelial detachment, PED)가 동반된 신생혈관에서 항 혈관내피성장인자 항체를 이용하여 혈관 투과성을 감소시켜, PED와 망막부종을 줄인 후 레이저 에너지가 맥락막혈관신생에 충분히 투과되어 광 역학요법의 효과를 극대화 하고자 하였다. 또한 광역학요법은 플루레신형광안저혈관조영(fluorescein angiography, FA)상 누출 부위를 모두 포함하는 기존방식과 달리,17인도시아닌 형광안저혈관조영(indocyanine green angiography, ICGA) 소견에 따라 시행되었다. 이는 치료 범위를 ICGA에서 파악 된 신생혈관에만 국한시킴으로써 그 치료 범위를 줄이고, 주변 정상 맥락막모세혈관의 폐쇄로 인한 허혈을 최소화하여 VEGF 활성화를 줄이고자 하였다.
대상과 방법
2006년 7월부터 2007년 8월 사이 본원 안과에서 나이관 련황반변성에 의한 맥락막혈관신생으로 유리체강내 bevaci- zumab주사와 광역학요법의 복합치료를 시행 받은 환자 중, 1유두직경 크기 이상의 PED를 동반된 환자 13명 13안을 대 상으로 의무기록과 영상자료를 후향적으로 분석하였다.
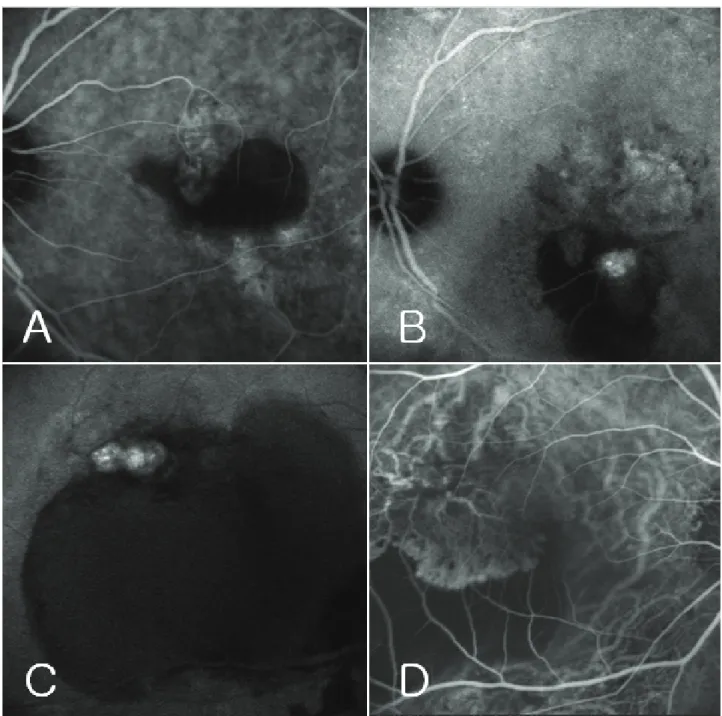
Figure 1. Indocyanine green angiography (ICGA) of case 11 (A, B) and case 13 (C, D) at the initial visit (A, C) and before combined treatment of intravitreal bevacizumab injection and photodynamic therapy (PDT) (B, D). At the initial visit of case 11, ICGA demonstrates neovascular nets with pigment epithelial detachment (PED) (A). After second treatment of PDT, persisted neovascular net mixed with newly appearing polypoidal like lesion on ICGA (B).
At initial visit of case 13, ICGA demonstrates a cluster of polypoidal lesion with large PED (C). After singlecombined treatment of intravitreal triamcinolone injection and PDT, noted the regression of cluster of polypoidal lesion with PED, and then recurred the lesion changed typical neovascular nets with PED on ICGA (D).
모든 환자는 55세 이상이었고, 혈관무늬망막병증, 중심 성장액맥락망막병증, 변성근시, 외상, 포도막염 등 다른 안 과적 질환과 연관된 맥락막혈관신생은 대상군에 포함시키 지 않았다. 13안 중 8안은 본 연구의 복합치료를 시행 받기 전에 레이저치료, 광역학요법, 유리체강내 트리암시놀론 주
사의 단일치료나 병용치료 후 병변이 지속되거나 재발된 경우였다. 또한 기존에 광역학요법을 최종적으로 시행받았 던 환자는 본 연구의 복합치료와의 치료간격이 최소 3개월 이상이었으며, 치료 후 망막색소상피 파열, 망막색소상피 위축이나 지속적인 맥락막 허혈 등의 합병증을 보인 경우는
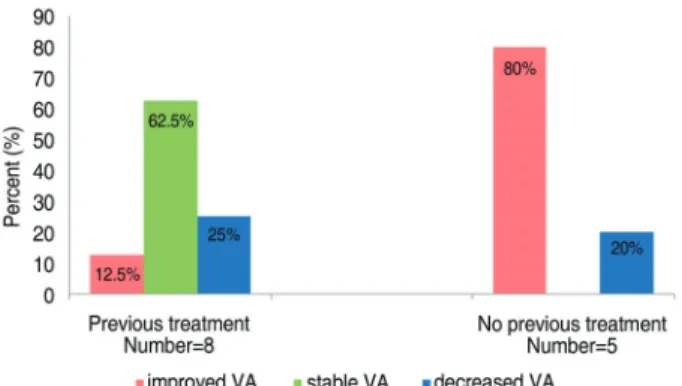
Figure 2.Distribution of final visual outcome for patients having previous treatment and no previous treatment;
VA=visual acuity.
Figure 3.Fundus photographs, fluorescein angiography (FA), optical coherence tomography (OCT) and indocyanine green angiography (ICGA) of case 2 at baseline (A-C) and at 3 months after single combined treatment and consecutive two additional bevacizumab injection (D-F). Note the resolution of the choroidal neovascularization and pigment epithelial detachment on FA, OCT and ICGA.
포함되지 않았다.
대상환자 모두는 confocal scanning laser ophthalmoscope (Heidelberg Retina Angiograph)를 이용한 ICGA의 결과를 후향적으로 분석하여 확실한 맥락막혈관신생으로 진단된 9명, 9안과 맥락막혈관신생과 결절맥락막혈관병증(polypoidal choroidal vasculopathy, PCV) 사이에 구별이 모호한 4명,
4안으로 세분하였다. 전자는 저형광의 PED 내부나 경계부 에 초기상 그물망의 혈관구조(neovascular nets) 또는 후 기상에서 과형광(plaque)이 관찰되는 경우에 진단하였다.
후자는 초기 진단과 달리 치료 후 경과관찰 중에 병변의 형 태가 바뀌거나 결절과 유사한 병변과 그물모양의 신생혈관 이 혼재되어 있는 경우가 관찰되어 진단이 모호한 군을 따 로 구분하였다(Fig. 1). PED의 크기는 ICGA에서 관찰되는 저형광의 크기를 측정하여 평가하였다.
모든 환자에 대해 치료 전 교정시력, 안저검사, 빛간섭단층 촬영(optical coherence tomography, OCT), FA 및 ICGA를 시행하였다. 환자의 경과관찰은 병변이 활동성일때, 기본적 으로 4~6주 간격으로 이루어졌으며, 매 방문시마다 교정 시력, 안저검사 및 OCT를 시행하였고, FA와 ICGA는 3~4개월 간격으로 시행하였다. 그 이후로는 병변의 활동 성에 따라 1~4개월 간격으로 경과관찰 기간을 조절하였고, OCT, FA 및 ICGA는 내원 시 병변의 상태에 따라 결정하 였다. 최대교정시력은 스넬렌 시력표를 이용하여 측정한 후 logMAR 지수로 변환하였다.
복합치료는 유리체강내 bevacizumab (Avastin; Genentech
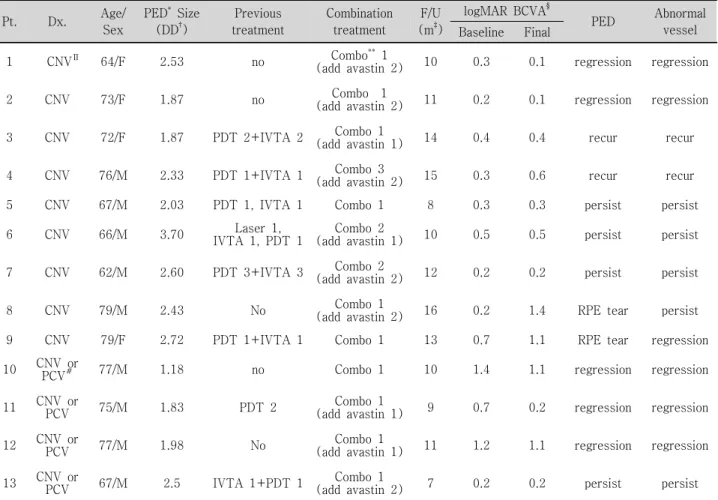
Table 1. Demographic data of patients
Pt. Dx. Age/
Sex
PED* Size (DD†)
Previous treatment
Combination treatment
F/U (m‡)
logMAR BCVA§
PED Abnormal vessel Baseline Final
1 CNV∏ 64/F 2.53 no Combo**1
(add avastin 2) 10 0.3 0.1 regression regression
2 CNV 73/F 1.87 no Combo 1
(add avastin 2) 11 0.2 0.1 regression regression
3 CNV 72/F 1.87 PDT 2+IVTA 2 Combo 1
(add avastin 1) 14 0.4 0.4 recur recur
4 CNV 76/M 2.33 PDT 1+IVTA 1 Combo 3
(add avastin 2) 15 0.3 0.6 recur recur
5 CNV 67/M 2.03 PDT 1, IVTA 1 Combo 1 8 0.3 0.3 persist persist
6 CNV 66/M 3.70 Laser 1,
IVTA 1, PDT 1 Combo 2
(add avastin 1) 10 0.5 0.5 persist persist
7 CNV 62/M 2.60 PDT 3+IVTA 3 Combo 2
(add avastin 2) 12 0.2 0.2 persist persist
8 CNV 79/M 2.43 No Combo 1
(add avastin 2) 16 0.2 1.4 RPE tear persist
9 CNV 79/F 2.72 PDT 1+IVTA 1 Combo 1 13 0.7 1.1 RPE tear regression
10 CNV or
PCV# 77/M 1.18 no Combo 1 10 1.4 1.1 regression regression
11 CNV or
PCV 75/M 1.83 PDT 2 Combo 1
(add avastin 1) 9 0.7 0.2 regression regression 12 CNV or
PCV 77/M 1.98 No Combo 1
(add avastin 1) 11 1.2 1.1 regression regression 13 CNV or
PCV 67/M 2.5 IVTA 1+PDT 1 Combo 1
(add avastin 2) 7 0.2 0.2 persist persist
*PED=retinal pigment epithelial detachment; †DD=disc diameter; ‡m=months; §BCVA=best corrected visual acuity;
∏NV=choroidal neovascularization; #PCV=polypoidal choroidal vasculopathy Combo; **=combination treatment of intravitreal bevacizumab and photodynamic therapy.
In., San Francisco, CA) 1.25 mg/0.05 ml 주사 후 1주일 이내에 시행한 광역학요법을 기본단위로 하였다. 병변이 활 동성일 때, 매 방문 시 시행한 안저검사와 OCT상 PED와 망막하 삼출액이 호전 없이 지속된 경우 추가적인 bevacizumab 주사를 4~6주 간격으로 시행하였다. 추가적인 복합치료는 FA와 ICGA에서 형광누출이나 이상혈관이 지속될 때 늦어도 4개월 간격으로 시행하였다. 광역학요법은 Treatment of Age-Related Macular Degeneration with Photodynamic Therapy (TAP) Study의 치료 지침에 따라서 시행하였고,17 레이저 조사범위는 ICGA에서 파악된 신생혈관을 포함하여 전체 1,000 μm를 추가하였다.
시력의 평가는 스넬렌 시력을 기준으로 2줄 이상(logMAR 교정시력≥0.2)의 증가를 호전, 1줄 이하 (logMAR 교정시 력±0.1)의 변화는 유지, 2줄 이상(logMAR 교정시력≥0.2)의 감소는 악화로 판단하였다. 통계분석은 SPSS 14.0 (SPSS for window version 14.0, SPSS Inc., Chicago, IL)을 이용 하였고, 치료 전후 logMAR 시력의 비교는 Wilcoxon signed-
ranks test를 이용하였다.
결 과
나이는 62세부터 79세까지 평균 71.8±5.94세였고, 남자 9명, 여자 4명이었다. 경과관찰 기간은 8개월에서 16개월로 평균 11.2±3.30개월이었다. 본 연구의 복합치료 전 여러 가지 치료를 시행 받았던 8안중 4안은 병변이 지속되었고 (증례 3, 4, 9, 11), 1안은 병변이 진행하였으며(증례 5), 나머지 3안은 재발한 경우였다(증례 6, 7, 13)(Table 1).
복합치료 횟수는 1회에서 3회로 평균 1.31±0.63회, 추가적 인 유리체강내 bevacizumab 주사는 1회에서 2회까지 평균 1.23±0.52회였다.
치료 전 logMAR 최대교정시력은 1.4에서 0.2 사이로 평균 0.50±0.39 (Snellen equivalent 20/63)였고, 치료 후 logMAR 최대교정시력은 1.4에서 0.1 사이로 평균 0.56±0.46 (Snellen equivalent 20/73)였다(p>0.05). 치료 후 최종 내원 시 시
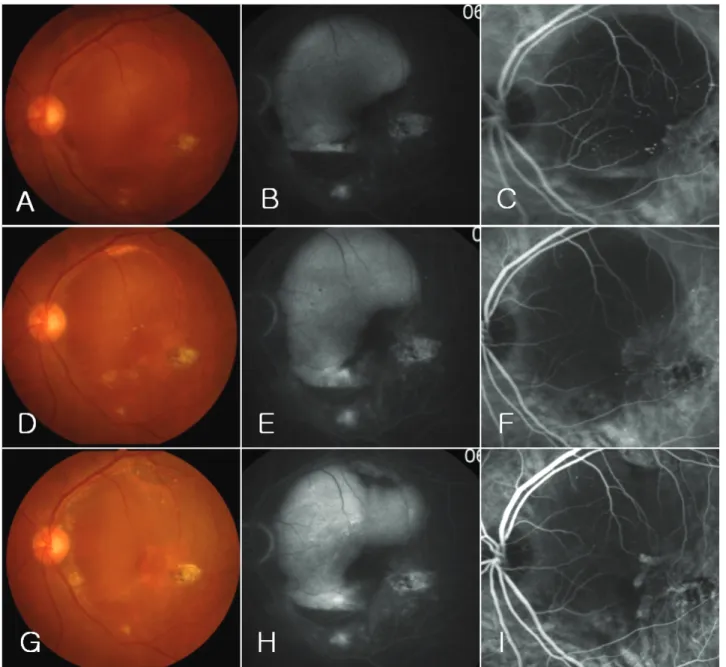
Figure 4.Fundus photographs, fluorescein angiography (FA) and indocyanine green angiography (ICGA) of case 6 at baseline (A-C), at 3 months after first combined treatment (D-F) and at 3 months after second combined treatment and one additional bevacizumab injection (G-I). Note the persistent of pigment epithelial detachment and choroidal neovascularization on FA and ICGA, but visual acuity remained stable.
력의 변화는 호전 3안(23.1%), 유지 7안(53.8%), 악화 3 안(23.1%)이었다. 치료 전 PED의 크기는 1.18에서 3.70 유두직경 크기로 평균 2.27±0.60 유두직경 크기였다. 치료 후 최종 내원 시 PED의 크기 변화는 소실 5안(38.5%), 소실 후 재발 2안(15.4%), 지속 4안(30.8%), 망막색소상피 파열이 2안(15.4%)이었다(Table 1).
기존에 광역학요법을 포함한 치료를 시행 받았던 8안에 서 최종 검사상 망막색소상피 파열이 발생한 1안(12.5%) 과 병변이 소실 후 재발된 1안(12.5%)은 시력이 감소하였 다. 나머지 6안중 1안(12.5%)은 병변 소실 후 5줄의 시력
호전을 보였고, 5안(62.5%)은 병변이 지속 또는 재발하였 으나 시력은 유지되었다. 치료의 과거력이 없는 5안은 망막 색소상피 파열이 발생하여 시력이 저하된 1안(20%)을 제 외하고, 4안(80%)에서 PED와 맥락막혈관신생이 소실되고 평균 1.8줄의 시력호전을 보였다(Fig. 2)(Table 1).
ICGA에서 확실한 맥락막혈관신생으로 진단된 9안의 경 우 최종 경과관찰 시 2안(22%)에서 PED 및 맥락막혈관신 생이 소실되었고, 시력은 유지 및 향상되었다(Fig. 3). 3안 (33%)은 PED 및 맥락막혈관신생이 지속되었으나 시력은 유지되었다(Fig. 4). 2안(22%)에서는 복합치료 후 PED 및
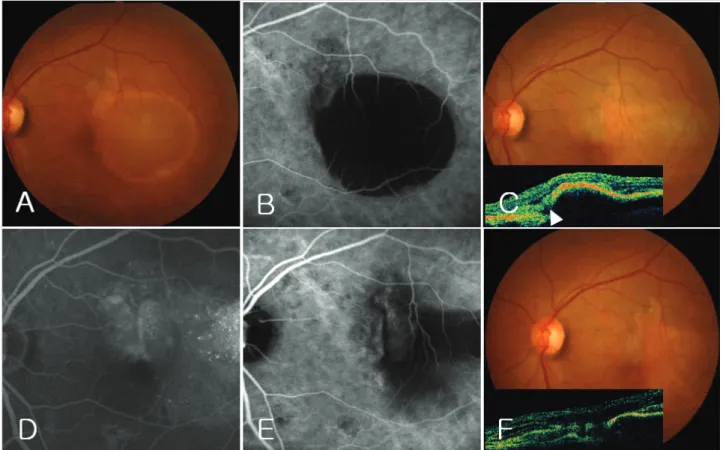
Figure 5.Fundus photographs, fluorescein angiography (FA), optical coherence tomography (OCT) and indocyanine green angiography (ICGA) of case 8. At baseline, showing choroidal neovascularization with pigment epithelial detachment (PED) (A-B). At 2 months after single combined treatment and consecutive two additional bevacizumab injection, showing the retinal pigment epithelial (RPE) tear on fundus photograph, FA, OCT, and ICGA (C-E). The arrowhead on OCT demonstrates RPE rip at the edge of detached RPE (C), but visual acuity was decreased within the 2 lines. At the 15 months, showing the subretinal fluid on OCT and marked decrease of visual acuity (F).
맥락막혈관신생이 소실되었으나 재발하였다. 재발 당시 1 안은 시력이 유지되었고(증례 3), 나머지 1안은 PED 및 맥 락막혈관신생이 재발 후 크기가 증가되고 시력이 감소하였 다(증례 4). 나머지 2안(22%)은 망막색소상피 파열이 발생 한 경우로 1안은 복합치료와 2회의 추가적인 bevacizumab 주사 후 8주째 파열이 발생하였고, 이후 맥락막혈관신생은 지속되었으나 시력감소가 2줄 이내로 유지되다가 15개월째 망막하액이 발생하여 12줄의 현저한 시력저하가 발생하였 다(증례 8)(Fig. 5). 파열이 발생한 나머지 1안은 복합치료 후 7주째 파열이 발생하였고, 맥락막혈관신생은 소실되었 으나 4줄의 급격한 시력저하를 보였다(증례 9)(Fig. 6) (Table 2).
결절맥락막혈관병증과 구별이 모호한 4안은 치료 후 최종 경과관찰 시 3안(75%)에서 PED 및 이상혈관이 소실 되었고, 시력변화는 2안은 호전, 1안은 유지되었다. 나머지 1안(25%)은 PED 및 이상혈관은 지속되었으나 시력은 유 지되었다(Fig. 6)(Table 2). 복합치료에 따른 안내염, 포도
막염, 안압의 증가, 망막색소상피 위축 및 전신적인 합병증 은 발생하지 않았다.
고 찰
맥락막혈관신생과 연관된 PED의 자연 경과는 PED의 지 속, 망막색소상피 위축, 원반반흔 형성이나 망막색소상피 파열이 발생하여 결국 대부분에서 심한 시력저하를 초래한
다.18-21이런 이유로 그 동안 레이저광응고술이나 광역학요
법이 시도되었으나, 해부학적 결과나 시력결과는 매우 불량 하였다.22-27
최근에는 항 혈관내피성장인자 항체인 bevacizumab 치료 후 Bom Aggio et al28은 1예에서 시력호전과 PED의 소실 을 보고하였고, Frimpong-Boateng et al29은 6개월간의 단 지적인 결과이지만 93.8% (15/16)에서 시력이 안정화되었 다고 하였다. 또한 Chen et al30은 기존의 다른 치료에 반응 을 보이지 않은 10안 중 9안에서 bevacizumab 주사 후 시력
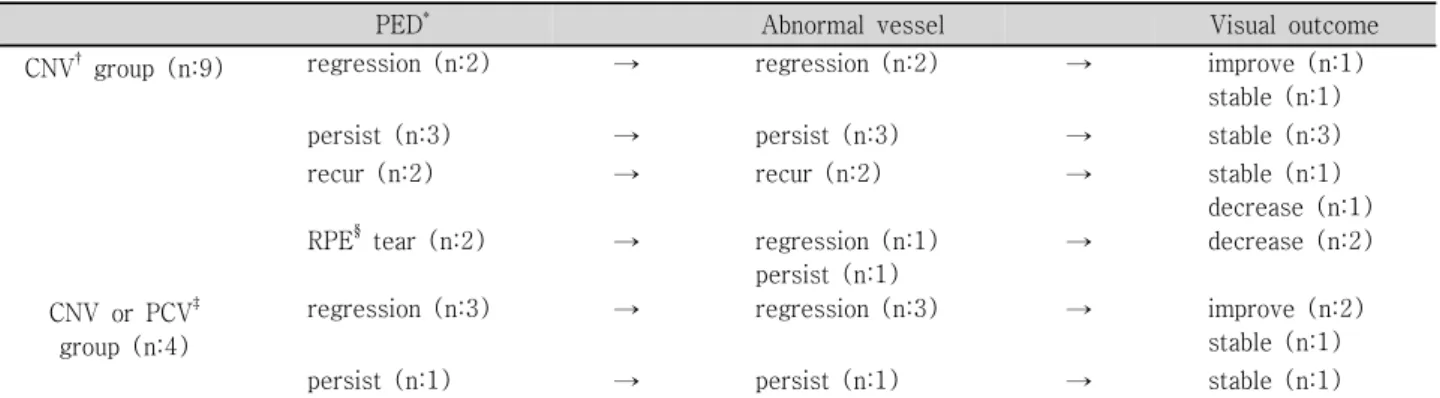
Table 2. Subdivide into final result of CNV and PCV or CNV group according to serial state of PED and abnormal vessel and visual outcome
PED* Abnormal vessel Visual outcome
CNV† group (n:9) regression (n:2) → regression (n:2) → improve (n:1)
stable (n:1)
persist (n:3) → persist (n:3) → stable (n:3)
recur (n:2) → recur (n:2) → stable (n:1)
decrease (n:1)
RPE§ tear (n:2) → regression (n:1)
persist (n:1)
→ decrease (n:2)
CNV or PCV‡ group (n:4)
regression (n:3) → regression (n:3) → improve (n:2)
stable (n:1)
persist (n:1) → persist (n:1) → stable (n:1)
*PED=retinal pigment epithelial detachment; †CNV=choroidal neovascularization; ‡PCV=polypoidal choroidal vasculopathy;
§RPE=retinal pigment epithelium.
Figure 6. Distribution of final visual outcome of CNV group and CNV or PCV group; CNV=choroidal neovasculari- zation; PCV=polypoidal choroidal vasculopathy; VA=
visual acuity.
이 유지되거나 호전되며, 6개월 이전까지는 통계적으로 의미 있는 시력호전을 보였다고 하였다. 이렇듯 bevacizumab은 PED를 동반한 맥락막혈관신생의 선택적인 치료방법으로 단 기적이지만 희망적인 결과를 보여주었다. 본 연구에서도 6개 월까지 13안 중 망막색소상피 파열이 발생하여 시력이 저하 된 2안을 제외한 11안(85%)에서 시력이 호전되거나 유지되 었다. 이는 발생시점으로 미루어 치료와 연관된 파열로 예상 되는 2안을 제외한다면 11안 모두에서 6개월까지는 안정된 시력이 유지되었다.
본 연구에는 기존에 광역학요법을 포함한 여러 가지 치 료를 시행 받은 후 병변이 지속되거나 재발된 8안이 포함되 었는데, 8안 중 1안(13%)에서만 병변이 소실된 후 시력호 전을 보였고, 5안(63%)은 시력이 유지되었으나 병변은 지 속되거나 재발하였다. 이에 비해 치료의 과거력이 없는 5안 중 4안(80%)은 병변이 소실되고 평균 1.8줄의 시력호전을 보였다. 이는 기존의 여러 가지 치료를 받았던 경우에 비해 새롭게 진단된 경우가 복합치료에 대한 단기적인 시력예후
및 해부학적 결과가 좋았다.
한편, Ladas et al31은 PED를 동반한 맥락막혈관신생 6안 에 대해 bevacizumab 유리체강내 주사와 광역학요법의 복 합치료 후 모든 예에서 9개월까지 시력이 유지되거나 향상 되었고, 5안(83.3%)에서 PED가 소실되었다고 보고하였다.
본 연구는 평균 11.2개월의 경과관찰을 시행하였고, 13안중 10안(76.9%)에서 시력이 유지되거나 호전되었다. 53.8%(7/13) 에서PED 및 맥락막혈관신생이 소실되었고, 이 중 2안은 PED 소실 후 각각 11개월(증례 3)과 7개월(증례 4)째 재발하였 다. 나머지 5안은 병변의 소실 후 최소 6개월 이상 재발없 이 유지되었다. 이는 복합치료 후 PED가 소실된 경우 병변 의 안정화가 최소한 6개월까지는 유지됨을 알 수 있었다.
또한 본 연구가 광역학요법의 과거력이 61.5% (8/13)로 Ladas et al31의 16.7% (1/6)에 비해 현저히 높고, 망막색소 상피 파열이 2안에서 발생하였으며, 경과관찰 기간이 더 긴 점이 재발의 가능성을 높여 Ladas et al31의 보고에 비해 시력 예후가 나빴을 것으로 여겨진다.
Chen et al30의 PED의 크기의 변화는 시력과 연관성이 없었다는 보고처럼, 본 연구에서 13안에 대한 복합치료 후 PED와 맥막막혈관신생이 소실된 5안, 소실 후 재발된 1안, 지속된 4안, 총 10안(76.9%)에서 시력이 유지되거나 향상 되었다. 단지 망막색소상피 파열이 발생한 2안과 PED가 소실 후 재발하고 맥락막혈관신생의 크기가 증가한 1안, 총 3안 (23.1%)에서 시력이 감소하였다. 이로 미루어 PED의 소실 및 맥락막혈관신생의 퇴행을 유도하는 것이 가장 이상적인 치료 목표이나, PED는 지속되어도 맥락막혈관신생의 증식을 억제시킨다면 시력의 유지에 단기적으로는 치료적 의의가 있을 것으로 생각된다.
본 연구에서는 진단이 모호한 군을 따로 분류하였다. 이는 모든 대상환자의 ICGA 소견을 재검토한 결과 초진과 달리 치료 후 경과에 따라 병변의 형태가 바뀌거나 결절맥락막
혈관병증의 결절형태와 맥락막혈관신생에서 보이는 그물 모양의 혈관구조가 혼재되어 있는 경우가 관찰되었기 때문 이다. 이러한 진단이 모호한 군은 100% (4/4)에서 시력이 호전 및 유지되었고, PED와 혈관신생의 소실은 75% (3/4) 에서 관찰되었다. 이에 비해 확실한 맥락막혈관신생군은 66.7% (6/9)에서 시력이 호전 및 유지되었고, 병변의 소실은 44.4% (4/9)에서 관찰되었으나 2안은 재발하였다. 이는 ICGA상 진단이 모호한 군이 확실한 맥락막혈관신생 형태를 동반한 경우에 비해 단기적으로 PED와 신생혈관 소실의 가 능성이 높으며 시력예후가 더 좋을 것으로 여겨진다.
일반적으로 크기가 큰 불규칙한 형태의 PED를 동반한 맥락막혈관신생에서 망막색소상피 파열의 위험성이 증가하 는 것으로 알려져 있다.32-34이러한 파열은 자연경과관찰 중 10~12.5%에서 발생하는 것에 비해 광역학요법 후에는 13%, 유리체강내 항 혈관내피성장인자 항체를 주사한 경 우에는 15~17.1%까지 발생이 증가된다고 보고되고 있
다.21,33-36또한 치료와 연관된 파열은 대부분 치료 후 4~8주
이내에 발생하는 것으로 알려져 있다.26,27,33,34,37,38
본 연구 에서도 13안중 2안(15.4%)에서 각각 복합치료와 추가적인 bevacizumab 주사 후 8주째(증례 8), 복합치료 후 7주째 (증례 9) 파열이 발생하였고, 2안 모두 확실한 맥락막혈관 신생 환자에서 발생하였다. 증례 8은 균일한 형광고임을 보 이는 2.43 유두직경 크기, 증례 9는 불규칙한 형광고임을 보이는 2.72 유두직경 크기의 PED로 평균 2.27 유두직경 크기에 비해 큰 경우였다. 이는 크기가 큰 PED에서 치료와 연관된 파열의 발생이 증가된다는 위험요소와 일치하는 소 견이었다. 또한 확실한 맥락막혈관신생군에서는 66.6%
(6/9), 진단인 모호한 군에서는 25% (1/4)에서 평균 PED에 비해 크기가 큰 경우였다. 이는 진단이 모호한 경우가 망막 색소상피 파열의 가능성이 적다고 단정하기는 어려웠다. 망 막색소상피 파열의 정확한 기전은 확립되지 않았지만,33,39,40 복합치료가 각각의 치료에 대한 상호작용에 의해 망막색 소상피 파열의 가능성이 증가될 수 있다. 그러나 본 연구에 서는 15.4%로 항 혈관내피성장인자 항체의 단일치료 후 보 고되는 파열의 빈도보다 높지 않았다.
광역학요법은 신생혈관뿐 아니라 주위의 정상 맥락막모 세혈관에도 일시적으로 저관류를 일으킨다. 이러한 정상 맥 락막모세혈관의 재관류에는 VEGF가 필요한데, 항 혈관내 피성장인자 항체를 사용한 복합치료는 정상 모세혈관의 재 관류에 필요한 VEGF까지 억제하여, 정상적인 맥락막모세 혈관의 심각한 허혈을 야기할 수 있다.15,16그러나 본 연구 에서는 평균 1.3회의 복합치료를 시행 후 경과관찰 기간 동안, 레이저 조사범위의 지속적인 저형광은 모든 예에서 관찰되지 않았다.
본 연구는 대상환자가 적고, 평균 11.2개월의 단기적인 결과이며, 표준화된 계획에 따른 경과관찰과 검사가 시행되지 못했다. 또한 본 연구의 복합치료 전 광역학요법 및 여러 가지 치료를 시행 받았던 8안(61.5%)을 포함시켜, 치료의 과거력이 없는 환자만을 대상으로 한 연구와의 해부학적 결과 및 시력예후에 차이를 보일 수 있는 제한점이 있다.
결론적으로 이번 연구를 통해 bevacizumab 유리체강내 주사와 광역학요법의 복합치료는 맥락막혈관신생과 연관된 PED 환자에서 시력의 안정화에 기여할 수 있는 하나의 치료 방법으로 이용될 수 있다. 특히 치료에 과거력이 없이 새롭 게 진단된 환자나 ICGA에 따른 병의 경과과정에서 진단이 모호한 경우 본 연구의 복합치료가 보다 효과적일 것으로 여겨진다. 다만 PED의 크기가 큰 경우 망막색소상피 파열 로 인한 예기치 않는 시력저하를 고려해야 한다. 추후 보다 많은 환자를 대상으로 장기적인 추적관찰 및 항 혈관내피 성장인자 항체인 약제들의 단일요법과 대조연구가 필요할 것으로 생각된다.
참고문헌
1) Dastgheib K, Green WR. Granulomatous reaction to Bruch’s membrane in age-related macular degeneration. Arch Ophthalmol 1994;112:813-8.
2) Oh H, Takagi H, Takagi C, et al. The potential angiogenic role of macrophages in the formation of choroidal neovascular membranes.
Invest Ophthalmol Vis Sci 1999;40:1891-8.
3) Ferrara N. Vascular endothelial growth factor. The trigger for neovascularization in the eye. Lab Invest 1995;72:615-18.
4) Adamis SP, Shima DT. The role of vascular endothelial growth factor in ocular health and disease. Retina 2005;25:111-8.
5) Spaide RF, Sorenson J, Maranan L. Combined photodynamic therapy with verteporfin and intravitreal triamcinolone acetonide for choroidal neovascularization. Ophthalmology 2003;110:1517- 25.
6) Chan WM, Lai TY, Wong AL, et al. Combined photodynamic therapy and intravitreal triamcinolone injection for the treatment of subfoveal choroidal neovascularization in age related macular degeneration: a comparative study. Br J Ophthalmol 2006;90:
337-41.
7) Freund KB, Klais CM, Eandi CM, et al. Sequenced combined intravitreal triamcinolone and indocyanine green angiography- guided photodynamic therapy for retinal angiomatous prolifera- tion. Arch Ophthalmol 2006;124:487-92.
8) Dhalla MS, Shah GK, Blinder KJ, et al. Combined photodynamic therapy with verteporfin and intravitreal bevacizumab for choroidal neovascularization in age-related macular degeneration. Retina 2006;26:988-93.
9) Costa RA, Jorge R, Calucci D, et al. Intravitreal bevacizumab (Avastin) in combination with verteporfin photodynamic therapy for choroidal neovascularization associated with age-related macular degeneration (IBeVe Study). Graefes Arch Clin Exp Ophthalmol
2007;245:1273-80.
10) Smith BT, Dhalla MS, Shah GK, et al. Intravitreal injection of bevacizumab combined with verteporfin photodynamic therapy for choroidal neovascularization in age-related macular degenera- tion. Retina 2008;28:675-81.
11) Ladewig MS, Karl SE, Hamelmann V, et al. Combined intravitreal bevacizumab and photodynamic therapy for neovascular age- related macular degeneration. Graefes Arch Clin Exp Ophthalmol 2008;246:17-25.
12) Krzystolik MG, Afshari MA, Adamis AP, et al. Prevention of experimental choroidal neovascularization with intravitreal anti- vascular endothelial growth factor antibody fragment. Arch Ophthalmol 2002;120:338-46.
13) Ferrara N, Damico L, Shams N, et al. Development of ranibizumab, an anti-vascular endothelial growth factor antigen binding fragment, as therapy for neovascular age-related macular degeneration. Retina 200626:859-70.
14) Schmidt-Erfurth U, Hasan T. Mechanisms of action of photo- dynamic therapy with verteporfin for the treatment of age-related macular degeneration. Surv Ophthalmol 2000;45:195-214.
15) Schmidt-Erfurth U, Schlötzer-Schrehard U, Cursiefen C, et al.
Influence of photodynamic therapy on expression of vascular endothelial growth factor (VEGF), VEGF receptor 3, and pigment epithelium-derived factor. Invest Ophthalmol Vis Sci 2003;44:
4473-80.
16) Spaide RF. Rationale for combination therapies for choroidal neovascularization. Am J Ophthalmol 2006;141:149-56.
17) Photodynamic therapy of subfoveal choroidal neovascularization in age-related macular degeneration with verteporfin: one-year results of 2 randomized clinical trials—TAP report. Treatment of Age-Related Macular Degeneration with Photodynamic Therapy (TAP) Study Group. Arch Ophthalmol 1999;117:1329-45.
18) Meredith TA, Braley RE, Aaberg TM. Natural history of serous detachments of the retinal pigment epithelium. Am J Ophthalmol 1979;88:643–51.
19) Poliner LS, Olk RJ, Burgess D, et al. Natural history of retinal pigment epithelial detachments in age-related macular degeneration.
Ophthalmology 1986;93:543–50.
20) Elman MJ, Finde SL, Murphy RP et al. The naturalhistory of serous retinal pigment epithelium detachment in patients with age-related macular degeneration. Ophthalmology 1986;93:224-30.
21) Pauleikhoff D, Löffert D, Spital G, et al. Pigment epithelial detachment in the elderly. Clinical differentiation, natural course and pathogenetic implications. Graefes Arch Clin Exp Ophthalmol 2002;240:533-8.
22) Slakter JS, Yannuzzi LA, Sorenson JA, et al. A pilot study of indocyanine green videoangiography guided laser photocoagu- lation treatment of occult choroidal neovascularization. Arch Ophthalmol 1994:112:465-72.
23) Lim JI, Aaberg TM, Capone A, Sternberg P. Indocyanine green angiography-guided photocoagulation of choroidal neovasculari- zation associated with retinal pigment epithelial detachment. Am J Ophthalmol 1997;123:524-32.
24) Brancato R, Introini U, Bolognesi G, et al. ICGA-guided laser photocoagulation of occult choroidal neovascularization in age- related macular degeneration. Retina 2000;20:134-42.
25) Han JW, Lee WK. Photodynamic therapy of choroidal neova- scularization associated with large serous pigment epithelial detach- ment. J Korean Ophthalmol Soc 2004;45:79-86.
26) Axer-Siegel R, Rosenblatt I, Kramer M, et al. Photodynamic therapy for occult choroidal neovascularization with pigment epithelium detachment in age-related macular degeneration. Arch Ophthalmol 2004;122:453-9.
27) Ladas ID, Kotsolis AI, Rouvas A, et al. Efficacy of photodynamic therapy in the management of occult choroidal neovascularization associated with serous pigment epithelium detachment. Ophthal- mologica 2007;221:313-9.
28) Bom Aggio F, Eid Farah M, Melo GB. Intravitreal bevacizumab for occult choroidal neovascularization with pigment epithelium detachment in age-related macular degeneration. Acta Ophthalmol Scand 2006;84:713-4.
29) Frimpong-Boateng A, Varde MA, Rüfer F, et al. Intravitreal administration of triamcinolone and bevacizumab for pigment epithelial detachment in conjunction with AMD. Ophthalmologe 2008;105:661-8.
30) Chen E, Kaiser RS, Vander JF. Intravitreal bevacizumab for refractory pigment epithelial detachment with occult choroidal neovascularization in age-related macular degeneration. Retina 2007;27:445-50.
31) Ladas ID, Kotsolis AI, Papakostas TD, et al. Intravitreal bevacizumab combined with photodynamic therapy for the treatment of occult choroidal neovascularization associated with serous pigment epithelium detachment in age-related macular degeneration. Retina 2007;27:891-6.
32) Coscas G, Koenig F, Soubrane G. The pretear characteristics of pigment epithelial detachments. A study of 40 eyes. Arch Oph- thalmol 1990;108:1687-93.
33) Chang LK, Sarraf D. Tears of the retinal pigment epithelium: an old problem in a new era. Retina 2007;27:523-34.
34) Chan CK, Meyer CH, Gross JG, et al. Retinal pigment epithelial tears after intravitreal bevacizumab injection for neovascular age- related macular degeneration. Retina 2007;27:541-51.
35) Casswell AG, Kohen D, Bird AC. Retinal pigment epithelial detachments in the elderly: classification and outcome. Br J Ophthalmol 1985;69:397-403.
36) Pece A, Isola V, Vadala M, Calori G. Photodynamic therapy with verteporfin for choroidal neovascularization associated with retinal pigment epithelial detachment in age-related macular degeneration.
Retina 2007;27:342-8.
37) Meyer CH, Mennel S, Schmith JC, et al. Acute retinal pigment epithelial tear following intravitreal bevacizumab (Avastin) in- jection for occult choroidal neovascularization secondary to age related macular degeneration. Br J Ophthalmol 2006;90:1207-8.
38) Chang LK, Flaxel CJ, Lauer AK, Sarraf D. RPE tears after pegaptanib treatment in age-related macular degeneration. Retina 2007;27:857-63.
39) Goldstein M, Heilweil G, Barak A, et al. Retinal pigment epithelial tear following photodynamic therapy for choroidal neovasculari- zation secondary to AMD. Eye 2005;9:1315-24.
40) Gass JD. Retinal pigment epithelial rip during krypton red laser photocoagulation. Am J Ophthalmol 1984;98:700-6.
=ABSTRACT=
Combination Treatment for Choroidal Neovascularization Associated With Large Retinal Pigment Epithelial Detachment
Jung-Wan Ryu, MD1, Jae-Hun Jung, MD2, Won-Ki Lee, MD1
Department of Ophthalmology and Visual Science, College of Medicine, The Catholic University of Korea, Seoul, Korea
Purpose: To evaluate the efficacy of the combination therapy of intravitreal bevacizumab injection and photodynamic therapy in neovascular age-related macular degeneration associated with large retinal pigment epithelial detachment.
Methods: A total of 13 eyes were reviewed, with 9 eyes diagnosed with definite choroidal neovascularization (CNV) and 4 eyes diagnosed with CNV or polypoidal choroidal vasculopathy (PCV) becausethe exact type could not be determined. Photodynamic therapy was performed within 1 week after bevacizumab injection according to indocyanine green angiography (ICGA). Additional bevacizumab injections were performed within a 4 to 6 week interval. Additional photodynamic therapy was performed within 4 months.
Results: The visual acuity on final examination had improved in 3 eyes (23.1%), was maintained in 7 eyes (53.8%), and decreased in 3 eyes (23.1%). The change of the PED before and after treatment showed regression in 5 eyes (38.5%), recurrence after regression in 2 eyes (15.4%), persistence in 4 eyes (30.8%), and retinal pigment epithelial tear in 2 eyes (15.4%). The maintained or improved visual acuity rate was 66.7% (6/9) and 100% (4/4) in the CNV and CNV or PCV group, respectively.
Conclusions: The combination therapy in neovascular age-related macular degenerationassociated with large retinal pigment epithelial detachment is a viable alternative treatment in the stabilization and improvement of vision. However, further studies with long-term follow up and controlled studies with anti-vascular endothelial growth factor antibody monotherapy are required.
J Korean Ophthalmol Soc 2009;50(6):877-886
Key Words: Bevacizumab, Choroidal neovascularization, Combination treatment, Photodynamic therapy, Retinal pigment epithelial detachment
Address reprint requests to Won Ki Lee, MD
Department of Opthalmology and Visual Science, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University
#505 Banpo-dong, Seocho-gu, Seoul 137-701, Korea
Tel: 82-2-2258-2846, Fax: 82-2-590-7405, E-mail: [email protected]