https://doi.org/10.14734/PN.2021.32.2.55 pISSN 2508-4887•eISSN 2508-4895
Myeong Gyun Choi, MD1, Jong Woon Kim, MD, PhD2, Wan Hu Jin, MD2,3, Yoon Ha Kim MD, PhD2
1Mokpo Medical Center, Mokpo;
2Department of Obstetrics and Gynecology, Chonnam National University Medical School, Gwangju, Korea, 3Department of Obstetrics and Gynecology, Yanbian University Hospital, Yanji, China
Objective: The aim of this study was to identify the factors affecting massive hemorrhages in patients with placenta previa. We also made probability models and equations for massive hemorrhage.
Methods: Seven hundred and sixty-four patients with placenta previa who underwent cesarean section from January 2011 to September 2019 were retrospectively reviewed. Massive hemorrhage was defined as a blood loss exceeding 1,500 mL or receiving over four units of packed red blood cells during cesarean section. Logistic regression analysis was used to create a probability model and identify the predictive factors for massive hemorrhage.
Results: Two hundred and seventy-three (35.7%) patients had massive hemorrhages. Preoperative hemoglobin levels, multifetal gestation, emergent surgery, history of a previous cesarean section, location of the placenta, the presence of lacuna, placental adhesion, the type of placenta previa, and multiparity were selected predictive factors for massive hemorrhage. One hundred seventy-eight (23.3%) patients had placenta previa and a history of previous cesarean section. Among them, massive hemorrhage occurred in 101 (56.7%). The selected predictive factors for massive hemorrhage in pati- ents with placenta previa and a history of previous cesarean section were emergent surgery, location of the placenta, the presence of lacuna, placental adhesion, and preoperative hemoglobin levels. An equation for massive hemorrhage in patients with placenta previa was created by combining variables.
Conclusion: An equation for massive hemorrhage in patients with placenta previa was created by combining variables. These equations may help in managing placenta previa patients with high risk.
Key Words: Hemorrhage, Placenta previa, Probability
Introduction
Placenta previa occurs when the placenta attaches inside the uterus but in an abnormal position near or over the cervical opening. The symptoms of placenta previa include vaginal bleeding in the second half of pregnancy, and for those after 36 weeks of pregnancy or with a significant amount of bleeding, a cesarean section is generally recommended.1 However, in some cases, placenta previa causes massive maternal hemorrhage and increases the risk of blood transfusion and cesarean hysterectomy.2,3 Due to the nature of placenta previa, bleeding during a cesarean section occurs immediately after placental separation. When there is a high risk of massive hemorrhage, a discussion among experts including maternal-fetal medicine specialists, medicine physicians, anesthesiologists is needed to manage the patient properly.3
The preoperative management and preparation of patients with placenta previa are impor- tant. Intravenous access with a large cannula is recommended and a central venous catheter should also be considered. Blood products should be ready for an immediate massive he- morrhage. Fresh frozen plasma, and packed red cells should be available.4 However, due to the complications associated with central venous catheters, the application must be carefully proceeded. Besides, prepared blood would be discarded if massive hemorrhage does not Received: 6 October 2020
Revised: 16 November 2020 Accepted: 9 December 2020 Correspondence to Yoon Ha Kim, MD, PhD Department of Obstetrics and Gynecology, Chonnam National University Medical School, 160 Baekseo-ro, Dong-gu, Gwangju 61469, Korea
Tel: +82-62-220-6375 Fax: +82-62-227-1637 E-mail: [email protected]
Copyright© 2021 by The Korean Society of Perinatology
This is an Open Access article distributed under the terms of the Creative Com- mons Attribution Non-Commercial License (http://creativecommons.org/
license/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any
Probability Model of Massive Hemorrhage
in Patients with Placenta Previa
As a result, it is necessary to evaluate the risk of massive he- morrhage and the amount of blood transfusion. In recent decades, massive transfusion protocols in obstetrics have shifted to the early administration of platelets, fresh frozen plasma, cryopre- cipitate. Pacheco et al.5 recommended activating a massive trans- fusion protocol when bleeding continues after the transfusion of four units of packed red blood cells (PRCs). The aim of this study was to identify the predictive factors of massive hemorrhage during operation among patients with placenta previa. Models and equations for the probability of massive hemorrhage were also made. The predictive factors for massive hemorrhage in cases of placenta previa with a previous cesarean section were also analyzed.
Methods
Seven hundred and sixty-four patients with placenta previa who underwent cesarean section from January 2011 to Sep- tember 2019 at the Department of Obstetrics and Gynecology were retrospectively reviewed. Clinical records, including ma- ternal demographics, clinical and ultrasonographic findings, and blood bank data were reviewed. Elective cesareasn delivery was done at 36+0 to 37+6 weeks. Placenta previa was diagnosed by prenatal vaginal or abdominal ultrasonography. Patients who were diagnosed with a low-lying placenta and delivered before 24 weeks were excluded. Low-lying placenta was diagnosed when the lower margin of the placenta was located within 2 cm of the internal cervical orifice. Patients who underwent vaginal deliveries were also excluded. Location of placenta were clas- sified based on the position of the main placenta (anterior, post- erior or lateral). Anterior placenta was categorized as type I and type II to consider the occupied percentage of lower segment by placenta (anterior type I, placenta is attached at the anterior wall of uterus; anterior type II, placenta is attached at the anterior wall of uterus and extends to the posterior lower segment of uterus [internal cervical os-posterior edge of placenta ≥2 cm]).
Massive hemorrhage was defined as a blood loss exceeding 1,500 mL or receiving over four units of PRCs during cesarean section.6 Obstetric massive hemorrhage is variably defined, but we focused on the recommendation activating massive transfu- sion protocol after the transfusion of four units of PRCs. The
Cli nical factors evaluated were maternal age, gestational age at delivery, parity, abortion history, cesarean section history, multifetal gestation, and presentation part when delivery, whe- ther the operation was emergent, tocolytic use before delivery, whe ther bleeding had started before surgery, and whether artificial reproductive technologies had been performed. The preoperative hemoglobin and estimated blood loss were mea- sured. The presence of lacuna, placental adhesion, the type of placenta previa, and the location of placenta were evaluated through ultrasonography. Lacuna was defined as an irregular lake-like area of low echogenicity within the placenta paren- chyma.7 Placental adhesion was diagnosed as the presence of at least 2 ultrasound findings among 5 findings (multiple vascular lacunae within the placenta, loss of the normal hypoechoic zone between the placenta and the myometrium, decreased retroplacental myo metrial thickness [less than 1 mm], abnor- malities of the uterine serosa-bladder interface, and the extension of the placenta into the myometrium, serosa).8,9
An independent t-test was used for the continuous variables.
The chi-squared test or Fisher’s exact test was used for the categorical variables. Multivariable logistic regression analysis was used to assess the association between massive hemorrhage and maternal age, gestational age at delivery, parity, history of abortion, history of cesarean section, preoperative hemoglobin levels, multifetal gestation, the presence of lacuna, the type of placenta previa, presentation part, location of the placenta, use of tocolytics, placental adhesion, and emergent surgery. The Hosmer-Lemeshow goodness of fit test was used to evaluate the significance of the probability models. P-values of >0.05 indicated that the model was suitable. The discrimination of the models was evaluated by area under the receiver operating cha racteristic curves (AUCs). The statistical analyses were performed using SPSS (version 25.0., IBM Corp., Armonk, NY, USA), 95% confidence intervals (CI) were calculated, and P- values of <0.05 indicated statistical significance.
Results
Among 764 patients included in the study, 273 (35.7%) had massive hemorrhages during cesarean sections and 491 (64.3%) patients did not. One hundred and one patients with a history of a
previous cesarean section had massive hemorrhages (37%) and 77 (15.7%) did not, showing a significant difference (P<0.01).
We performed cesarean hysterectomy on 37 patients with massive hemorrhage. Furthermore, 5 patients had arterial em- bolization and 3 patients had uterine artery ligation. A total of 41 patients were admitted to Intensive Care Units (ICU).
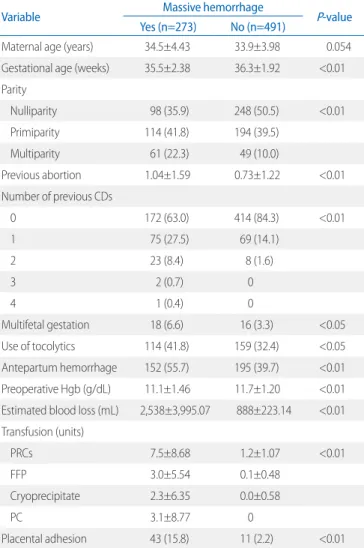
History of previous cesarean section, history of abortion, multifetal gestation, use of tocolytics, antepartum hemorrhage, number of parity, placental adhesion, the presence of lacuna, placenta previa totalis, location of the placenta, and emergent surgery were all significantly associated with massive hemorrh- age (P<0.05). Maternal age, uterine myoma, presentation part, and the use of assisted reproductive technologies were not significantly associated (Table 1).
Tables 2 and 3 show multivariable logistic regression analyses
Table 1. Univariate Association with Massive Hemorrhage
Variable Massive hemorrhage
P-value Yes (n=273) No (n=491)
Maternal age (years) 34.5±4.43 33.9±3.98 0.054
Gestational age (weeks) 35.5±2.38 36.3±1.92 <0.01 Parity
Nulliparity 98 (35.9) 248 (50.5) <0.01
Primiparity 114 (41.8) 194 (39.5)
Multiparity 61 (22.3) 49 (10.0)
Previous abortion 1.04±1.59 0.73±1.22 <0.01
Number of previous CDs
0 172 (63.0) 414 (84.3) <0.01
1 75 (27.5) 69 (14.1)
2 23 (8.4) 8 (1.6)
3 2 (0.7) 0
4 1 (0.4) 0
Multifetal gestation 18 (6.6) 16 (3.3) <0.05
Use of tocolytics 114 (41.8) 159 (32.4) <0.05
Antepartum hemorrhage 152 (55.7) 195 (39.7) <0.01 Preoperative Hgb (g/dL) 11.1±1.46 11.7±1.20 <0.01 Estimated blood loss (mL) 2,538±3,995.07 888±223.14 <0.01 Transfusion (units)
PRCs 7.5±8.68 1.2±1.07 <0.01
FFP 3.0±5.54 0.1±0.48
Cryoprecipitate 2.3±6.35 0.0±0.58
PC 3.1±8.77 0
Placental adhesion 43 (15.8) 11 (2.2) <0.01
Table 1. Continued
Variable Massive hemorrhage
P-value Yes (n=273) No (n=491)
Uterine myoma 22 (8.1) 43 (8.8) 0.740
Presence of lacuna 68 (24.9) 44 (9.0) <0.01
Presentation part
Vertex 233 (85.3) 442 (90.0) 0.054
Others 40 (14.7) 49 (10.0)
Type of previa
Totalis 233 (85.3) 308 (62.7) <0.01
Partialis or marginalis 40 (14.6) 183 (37.3) Location of placenta
Anterior (type I) 61 (22.3) 68 (13.8) <0.01
Anterior (type II) 85 (31.1) 60 (12.2) Posterior or lateral 127 (46.5) 363 (73.9) Type of surgery
Elective 154 (56.4) 367 (74.7) <0.01
Emergency 119 (43.6) 124 (25.3)
Conception method
Spontaneous 238 (87.2) 421 (85.7) 0.219
Ovulation induction 2 (0.7) 0
IVF-ET 28 (10.3) 57 (11.6)
Values are presented as mean±standard deviation or number (%).
Abbreviations: CDs, cesarean deliveries; Hgb, hemoglobin; PRCs, packed red blood cells; FFP, fresh frozen plasma; PC, platelet concentration; IVF-ET, in vitro fertilization-embryo transfer.
Table 2. Logistic Regression Analysis of Massive Hemorrhage in Pla- centa Previa Patients
B OR (95% CI) P-value
Previous cesarean section 0.515 1.67 (1.08-2.60) <0.05 Previous cesarean section (≥2)* 1.196 3.31 (1.19-9.21) <0.05 Preoperative Hgb (g/dL) -0.282 0.75 (0.66-0.86) <0.01
Parity 0.210 1.23 (0.97-1.56) 0.081
Multifetal gestation 0.784 2.19 (1.01-4.74) <0.05
Emergent surgery 0.664 1.94 (1.36-2.78) <0.01
Type of previa
Totalis 0.825 2.28 (1.50-3.48) <0.01
Location of placenta
Anterior (type I) 0.751 2.12 (1.36-3.32) <0.01 Anterior (type II) 0.827 2.29 (1.47-3.55) <0.01 Placental adhesion 1.583 4.87 (2.26-10.49) <0.01
Presence of lacuna 0.838 2.31 (1.43-3.74) <0.01
Abbreviations: OR, odds ratio; CI, confidence interval; Hgb, hemoglobin.
*There were 2 patients with history of third cesarean section and 1 patient with fourth cesarean section.
adhesion, and the presence of lacuna were factors included in the probability model. But preoperative hemoglobin and presence of lacuna were not statistically significant. The predictive accuracy of this model was 0.789 (95% CI: 0.723-0.855) (Fig. 1). The P- values of the Hosmer-Lemeshow test of models were >0.05.
The equations for massive hemorrhage among patients with placenta previa by combining variables were as follows:
Probability of massive hemorrhage in placenta previa (AUC 0.782)=ex/1+ex (X=0.890+0.210×parity+0.515×previous c-sec (if 1)+1.196×previous c-sec (if≥2)-0.282×preoperative hemo globin+0.825×placenta previa totalis+0.751×anterior placenta (I)+0.827×anterior placenta (II)+1.583×placental adhesion+0.838×presence of lacuna+0.664×emergent sur- gery+0.784×multifetal gestation)
Probability of massive hemorrhage in placenta previa with history of previous cesarean section (AUC 0.789)=ex/1+ex (X=1.015+0.183×preoperative hemoglobin +1.008× emergent surgery+0.942×anterior placenta (I)+1.314×anterior placenta (II)+0.771×presence of lacuna+2.379×placental adhesion)
Discussion
Placenta previa is known to involve various maternal compli- cations, such as antepartum bleeding, intrapartum and postpartum hemorrhages, blood transfusion, cesarean hysterectomy, septi- of the factors used to generate the probability model for massive
hemorrhage. We excluded uterine myoma and assisted repro- ductive technologies, then applied the other factors to the pro- bability model.
For patients with placenta previa , a history of previous cesa- rean section, the number of previous cesarean sections, preo- perative hemoglobin levels, multifetal gestation, emergent sur- gery, placenta previa totalis, location of the placenta, placental adhesion, the presence of lacuna, and number of parity were included in the probability model. But, number of parity were not statistically significant. The predictive accuracy of this model, as measured by the receiver operating characteristics curve was 0.782 (95% confidece interval [CI]: 0.748-0.816) (Fig. 1).
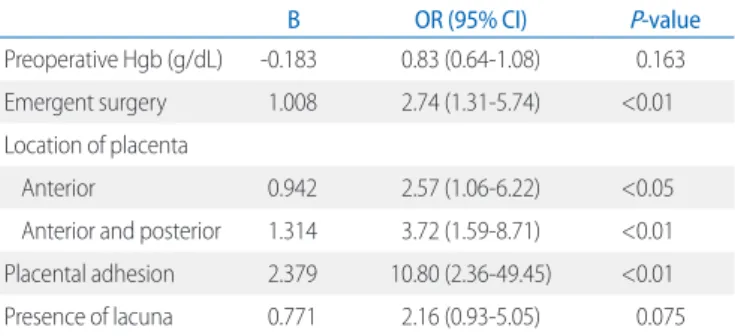
A probability model for placenta previa with previous cesarean section was also made. For patients with placenta previa and a history of previous cesarean section, preoperative hemoglobin level, emergent surgery, location of the placenta, placental
Table 3. Logistic Regression Analysis of Massive Hemorrhage in Pla- centa Previa Patients with Previous Cesarean Section
B OR (95% CI) P-value
Preoperative Hgb (g/dL) -0.183 0.83 (0.64-1.08) 0.163
Emergent surgery 1.008 2.74 (1.31-5.74) <0.01
Location of placenta
Anterior 0.942 2.57 (1.06-6.22) <0.05
Anterior and posterior 1.314 3.72 (1.59-8.71) <0.01 Placental adhesion 2.379 10.80 (2.36-49.45) <0.01
Presence of lacuna 0.771 2.16 (0.93-5.05) 0.075
Abbreviations: OR, odds ratio; CI, confidence interval; Hgb, hemoglobin.
1-specificity
Sensitivity
ROC curve
0.0 0.2 0.4 0.6 0.8 1.0
0.2 0.4 0.6 0.8 1.0
Sensitivity
A B
1-specificity ROC curve
0.2 0.4 0.6 0.8 1.0
0.0 0.2 0.4 0.6 0.8 1.0
Fig. 1. Receiver operating characteristics (ROC) curve analysis for massive hemorrhage in placenta previa (A), and placenta previa with previous cesarean section (B).
cemia, and thrombophlebitis.10 In the cases of massive hemorr- hage, additional treatments like cesarean hysterectomy, uterine artery embolization, uterine artery ligation were done. Further- more, some patients were admitted to ICU as a result of massive hemorrhage, hypovolemic shock, massive blood transfusion and its complications.
Probability models for massive hemorrhage (transfusion of ≥4 units of PRCs or blood loss ≥1,500 mL during cesarean section) in placenta previa and placenta previa with a previous cesarean section were made. In our study, placental location, the presence of lacuna, placental adhesion, emergent surgery, and a history of previous cesarean section were statistically significant factors in both massive hemorrhage probability models.
Higher preoperative hemoglobin decreased the risk of massive hemorrhage (odds ratio [OR] 0.75, 95% CI 0.66-0.86) in massive hemorrhage probability model, but not statistically significant in probability model with a history of cesarean section.
Placental adhesion (placenta accreta) is rare (about 1/2,500) but a known high-risk factor for obstetric hemorrhage, and also causes antepartum and postpartum hemorrhage, uterine perfo- ration, and infection.11 Diagnosing placental adhesion is very important, but not easy to confirm. A number of studies investi- gated diagnosing placental adhesion through ultrasonography.
The presence of placenta previa was present in more than 80%
of the patients with placenta accreta. Multiple vascular lacunae within the placenta, loss of the normal hypoechoic zone between the placenta and the myometrium, decreased retroplacental myometrial thickness (less than 1 mm), abnormalities of the ute- rine serosa-bladder interface, and the extension of the placenta into the myometrium, serosa or bladder are associated with placenta accreta.8,9 Other stuides reported that whether or not the placenta was located at the scar of a previous operation was associated with placenta accreta.12,13
Anterior placentation, a placenta with a longer os-placental edge distance in the anterior wall than in the posterior wall, is known to increase the risk of massive hemorrhage during ace sa rean section for placenta previa.14 In our study, anterior placenta showed higher risk of massive hemorrhage than post- erior or lateral placenta. Furthermore, anterior placenta type II (occupying the posterior lower segment of uterus) showed higher risk than type I.
Number of parity was included in the model. It increased the
risk of massive hemorrhage, but was not statistically significant (OR 1.23, 95% CI 0.97-1.56).
Multiple pregnancy is known to increase the risk of severe postpartum hemorrhage after cesarean delivery.15 Multiple preg- nancy was included in our probability model and increased the risk of massive hemorrhage.
A history of previous cesarean section increases the risk of obstetric hemorrhage.1 In our study both a history of a previous cesarean section and the number of cesarean sections were as sociated with massive hemorrhage. A history of cesarean section is also known to increase the risk of abnormal placental adhesion.2
To diagnose placenta previa totalis and placenta accreta, ul- trasonography is a tool of critical importance. Detailed ultrasono- graphy should be performed for patients with placenta previa.
The probability models for massive hemorrhage made in this study will provide practical help in determining the need to pre- pare blood products and other preoperative preparations like central venous catheter application. Hasegawa et al. reported that advanced maternal age, previous cesarean section, the presence of sponge-like findings in the cervix, and placental location on the scar of a previous cesarean section increased the risk of massive hemorrhage during cesarean section in cases of placenta previa.12,13 Baba et al.16 made a transfusion probability model for patients with placenta previa. The independent risk factors for allogenic blood transfusion they reported were scar covering, previous cesarean section without scar covering, and lacunae. Through our study, we made massive hemorrhage
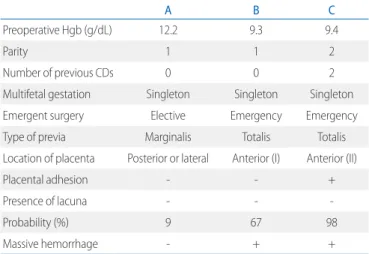
Table 4. How to Apply the Predictive Model to Patients
A B C
Preoperative Hgb (g/dL) 12.2 9.3 9.4
Parity 1 1 2
Number of previous CDs 0 0 2
Multifetal gestation Singleton Singleton Singleton
Emergent surgery Elective Emergency Emergency
Type of previa Marginalis Totalis Totalis
Location of placenta Posterior or lateral Anterior (I) Anterior (II)
Placental adhesion - - +
Presence of lacuna - - -
Probability (%) 9 67 98
Massive hemorrhage - + +
Abbreviation: Hgb, hemoglobin; CDs, cesarean deliveries.
probability model including hemoglobin levels, parity number, multifetal gestation, emergent surgery, location of the placenta, the presence of lacuna, placental adhesion, placenta previa totalis, and the number of previous cesarean.
Table 4 shows how to apply the probability model to placenta previa patients. In patient A, probability of massive hemorrhage through our model is 9%. In this case, excessive preparations could be avoided. Otherwise, probability of patient B and C is 67% and 98%. In these cases, intravenous access with a large cannula should be proceeded and central venous catheter should be considered. Enough blood products should also be ready for an immediate massive hemorrhage.
This study was limited by the nature of retrospective cohorts.
Some factors were based only on the review of medical records.
Besides, some factors like type of surgery are ambiguous as the predictive factor for massive hemorrhage. These factors are excluded. For more precise probability model, further study is required.
The probability models constructed in this study will provide help in screening patients at high risk for massive hemorrhage.
If it is possible to predict the probability of massive hemorrhage, preoperative preparations including the application of a central venous catheter, consultation with an anesthesiologist, and pre- paring enough units of PRCs or cryoprecipitate could be accom- plished before the critical hemorrhage. Conversely, excessive preoperative preparations for low-risk patients could be avoided.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
References
1) Allahdin S, Voigt S, Htwe TT. Management of placenta praevia and accreta. J Obstet Gynaecol 2011;31:1-6.
2) Choi SJ, Song SE, Jung KL, Oh SY, Kim JH, Roh CR. Antepartum risk factors associated with peripartum cesarean hysterectomy in women with placenta previa. Am J Perinatol 2008;25:37-41.
3) Dahlke JD, Mendez-Figueroa H, Maggio L, Hauspurg AK, Sperling JD, Chauhan SP, et al. Prevention and management of postpartum hemorr- hage: a comparison of 4 national guidelines. Am J Obstet Gynecol 2015;
213:76.e1-10.
4) Kocaoglu N, Gunusen I, Karaman S, Ergenoglu AM, Firat V. Management of anesthesia for cesarean section in parturients with placenta previa with/without placenta accreta: a retrospective study. Ginekol Pol 2012;
83:99-103.
5) Pacheco LD, Saade GR, Costantine MM, Clark SL, Hankins GD. An update on the use of massive transfusion protocols in obstetrics. Am J Obstet Gynecol 2016;214:340-4.
6) Trikha A, Singh PM. Management of major obstetric haemorrhage.
Indian J Anaesth 2018;62:698-703.
7) Finberg HJ, Williams JW. Placenta accreta: prospective sonographic diagnosis in patients with placenta previa and prior cesarean section. J Ultrasound Med 1992;11:333-43.
8) Berkley EM, Abuhamad AZ. Prenatal diagnosis of placenta accreta: is sonography all we need? J Ultrasound Med 2013;32:1345-50.
9) Comstock CH, Bronsteen RA. The antenatal diagnosis of placenta accreta. BJOG 2014;121:171-82.
10) Gibbins KJ, Einerson BD, Varner MW, Silver RM. Placenta previa and ma- ternal hemorrhagic morbidity. J Matern Fetal Neonatal Med 2018;31:
494-9.
11) Yang JI. The Prenatal sonographic diagnosis of placenta adhesion dis- orders. Korean J Ultrasound Obstet Gynecol 2011;13:97-103.
12) Hasegawa J, Matsuoka R, Ichizuka K, Mimura T, Sekizawa A, Farina A, et al. Predisposing factors for massive hemorrhage during cesarean section in patients with placenta previa. Ultrasound Obstet Gynecol 2009;34:
80-4.
13) Hasegawa J, Nakamura M, Hamada S, Matsuoka R, Ichizuka K, Sekizawa A, et al. Prediction of hemorrhage in placenta previa. Taiwan J Obstet Gynecol 2012;51:3-6.
14) Baba Y, Matsubara S, Ohkuchi A, Usui R, Kuwata T, Suzuki H, et al. Anterior placentation as a risk factor for massive hemorrhage during cesarean section in patients with placenta previa. J Obstet Gynaecol Res 2014;40:
1243-8.
15) Butwick AJ, Ramachandran B, Hegde P, Riley ET, El-Sayed YY, Nelson LM.
Risk factors for severe postpartum hemorrhage after cesarean delivery:
case-contral studies. Anesth Analg 2017;125:523-32.
16) Baba Y, Ohkuchi A, Usui R, Suzuki H, Kuwata T, Matsubara S. Calculating probability of requiring allogeneic blood transfusion using three preo- perative risk factors on cesarean section for placenta previa. Arch Gy- necol Obstet 2015;291:281-5.