유방 보존 수술 후 수술 부위에 방사선 치료를 하는 것이 인정 받고 있는 유방암의 치료법이다. 그러나 유관내 성분 (intraductal component)의 비율이 높은 유방암 환자는 유방 보존 수술 후에 높은 빈도의 국소 재발률을 보이고 있고(1), 대부분의 국소재발은 일차적으로 유방암의 절제가 불충분하 기 때문으로 생각된다. Abner 등, Leborgne 등(2, 3)은 국소 재발로 인하여 재수술을 시행한 경우 국소 재발이 발생하지 않은 환자에 비하여 생존율이 떨어진다고 보고하였고, Veronesi 등, Fisher 등(4, 5)의 연구에서는 국소 재발이 생
존율을 낮추는데 영향이 없다고 보고하였지만, 수술 전에 광 범위한 관내 상피암 성분(Extensive Intraductal Component, 이하 EIC)의 존재 유무를 예측하는 것은 적절한 수술적 절제 를 위하여 필수적이라고 하겠다.
현재 유방 촬영술과 초음파 검사가 유방암의 발견과 진단 의 주 방법이지만, 이들은 암의 퍼진 정도와 EIC 양성 유무 를 진단하는 데 있어서 비교적 낮은 민감도를 보이고 있다 (6). 본 연구에서는 EIC 양성 유방암을 발견하는데 있어서 자 기공명영상(Magnetic Resonance Image, 이하 MRI)와 유방 촬영술, 초음파 각각의 민감도를 비교하고, MRI의 장점과 역 할을 규명하고자 한다.
유방암의 광범위 관내 상피암 성분의 진단에 대한 MRI의 유용성: 유방 촬영술 및 초음파와의 비교1
김태희・강두경・정용식2・임현이3
목적: 광범위한 관내 상피암 성분(extensive intraductal component , EIC) 양성인 유방암은 국소 재발의 중요한 위험인자로 알려져 있지만 유방 촬영술에서 이를 진단하는 것은 어렵다.
EIC 양성 유방암을 진단하는 데 있어서 MRI의 유용성에 대해 알아보고 유방 촬영술, 초음파 의 민감도와 비교해보고자 한다.
대상과 방법: 2003년 3월부터 2004년 7월까지 유방암으로 MRI를 시행한 160명 중 EIC 유
무가 판정된 환자는 90명이었고, 이 중 조기 유방암(병기 I, II기) 환자 83명을 연구 대상으 로 하였다. 영상에서 EIC 양성은 다음과 같이 정의하였다. 1) 유방 촬영술에서 종괴 음영의 바깥에 위치하는 미세 석회화 혹은 종괴 음영 없이 악성 미세 석회화를 보이는 경우, 2) 유 방 초음파에서 종괴 주위에 관상의 저에코 구조가 보이는 경우 혹은 종괴 바깥에 석회화를 동반한 구조적 왜곡(architectural distortion)가 있는 경우, 3) MRI에서 종괴의 주변에 선상 형(linear) 혹은 관상형(tubular)의 조영증강, 분절형(segmental) 혹은 국소형(regional)의 응 집된(clumped) 조영 증강, 그리고 결절(nodular) 혹은 그물모양(reticular)의 조영 증강이 있 는 경우로 하였다. 41명의 환자에서 EIC양성이었고 42명은 음성이었다.
결과: EIC 양성 유방암에 대한 민감도는 유방 촬영술, 초음파, MRI에서 각각 48.6%, 67.5%, 80.5%이고, 특이도는 92.3%, 73.2%, 69.0%였다. 2가지 이상의 영상 기법에서 EIC 양성으 로 판정된 경우의 양성 예측도(positive predictive value)는 78.1%이고, 한가지 영상기법에 서만 EIC 양성으로 판정되거나 세 가지 영상 모두에서 EIC 음성으로 판정되었던 경우의 음 성 예측도(negative predictive value)는 75.0%였다.
결론: 유방 MRI는 유방암의 EIC 존재 유무를 판정하는데 유용하며 유방 촬영술이나 유방 초 음파에 비해 높은 민감도를 보인다. 그러나 특이도는 유방 촬영술에서 가장 높았다. 유방 촬 영술과 초음파, MRI를 같이 활용하면 EIC 양성 유방암을 보다 정확히 진단할 수 있다.
1아주대학교 의과대학 영상의학과교실
2아주대학교 의과대학 외과학교실
3아주대학교 의과대학 병리과학교실
이 논문은 2005년 8월 23일 접수하여 2005년 12월 20일에 채택되었음.
대상과 방법
2003년 3월부터 2004년 7월까지 유방암으로 수술 전 MRI 를 시행한 160명 중 EIC 유무가 판정된 환자는 90명이었고, 이 중 조기 유방암(병기 I, II기) 환자 83명을 연구 대상으로 하였다. 83명 중 41명은 EIC 양성이었고 42명은 EIC 음성이 었다. 환자의 연령은 28-83세였고 평균 45.3세였다(Table 1).
International Union Against cancer(UICC)에서 제정한 TNM 분류법에 의한 T stage는 T1a가 4명, T1b는 8명, T1c 는 27명, T2는 42명, T3는 2명이었다. TNM 분류에 의한 clinical stage는 I기 25명, IIA기 40명, IIB기 18명이었다.
50명의 환자는 변형 근치 유방 절제술이나 근치적 유방 절 제술을 시행하였고, 33명의 환자는 유방 보존 수술을 시행하 였다.
유방 촬영술은 DMR mammography(GE Medical System, Milwaukee, WI,U.S.A.)를 사용하였고, 내사외(mediolateral
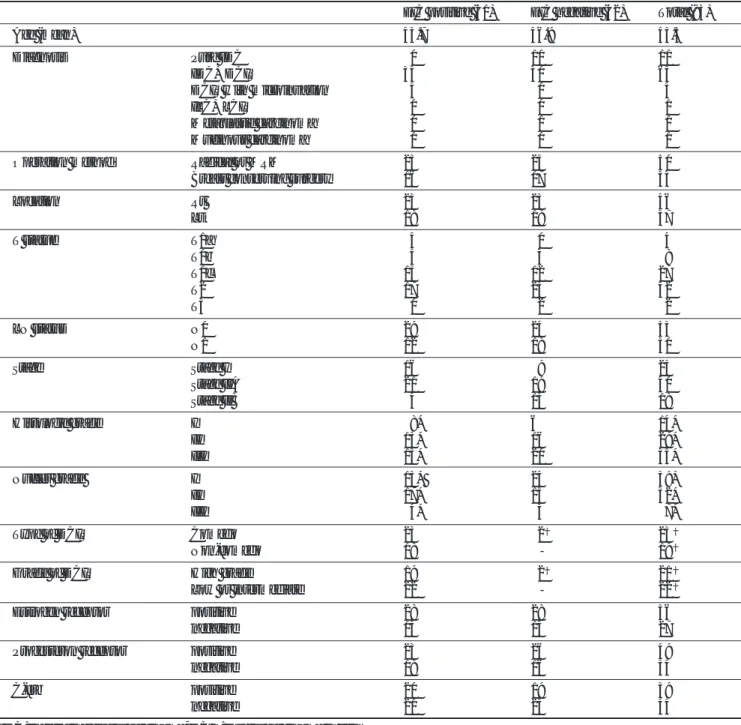
Table 1. Histopathologic Difference Between EIC Positive and EIC Negative Breast Cancer
EIC positive (41) EIC negative (42) Total (83)
Age (mean) 43.7 46.9 45.3
Diagnosis Pure IDC 00 11 11
IDC+DCIS 35 30 65
DCIS with microinvasion 04 00 04
ILC+LCIS 01 00 01
Metaplastic carcinoma 00 01 01
Mucinous carcinoma 01 00 01
Operation method Radical or MRM 25 25 50
Breast conserving surgery 16 17 33
Location Rt 23 23 46
Lt 18 19 37
T statue T1a 04 00 04
T1b 05 03 08
T1c 15 12 27
T2 17 25 42
T3 00 02 02
LN status N0 29 24 53
N1 12 18 30
Stage Stage I 16 09 25
Stage IIA 21 19 40
Stage IIB 04 14 18
Histologic grade I 08* 6 14*
II 13* 16 29*
III 15* 20 35*
Nucler grade I 15* 24 39*
II 17* 15 32*
III 04* 03 07*
Type of DCIS Comedo 23 02 25
Non-comedo 18 0- 18
Grade of DCIS High grade 19 02 21
Low or intermediate 22 0- 22
Estrogen receptor positive 28 28 56
negative 13 14 27
Progesteron receptor positive 23 26 49
negative 18 16 34
C-erb positive 20 19 39
negative 21 23 44
IDC: Infiltrating ductal carcinoma, DCIS: Ductal carcinoma in situ ILC: Infiltrating lobular carcinoma, EIC: Extensive intraductal component
*: except cases with ILC, or DCIS with microinvasion : cases with available pathologic examination
oblique) 촬영과 상하(craniocaudal) 촬영을 기본으로 하고, 필요한 경우에는 추가로 국소 확대 촬영을 시행하였다.
유방 초음파는 Sequoia (Acuson, Siemens Company, Mountain View, Calif, U.S.A.)의 8-13MHz 선형 탐촉자를 사용하여 종괴의 범위와 유관내 확장 정도를 평가하였다.
MRI는 1.5T 초전도형 MR기기 (Signa Horizon, GE Medial System, Milwaukee, WI, U.S.A.)로 시행하였다. 모든 환자들 은 엎드린 자세에서 이중 유방 코일을 사용하였고 암이 있는 쪽의 유방을 촬영하였다. 반복시간(repetition time)은 11.0 msec, 에코시간(echo time) 4.2 msec, 영상범위(field of view) 18 cm, 절편두께(slice thickness) 2.0 mm로 하였다.
저자들은 MRI 촬영시 환자의 월경 시기는 고려하지 않았 다.
종괴의 위치를 파악하기 위해서 축면 T1 강조영상을 시행 하였고, 낭성 병변을 감별하기 위하여 시상면 지방억제 T2 강조영상을 시행하였다. 조영제[gadolinium diethylenetriamine pentaacetic acid(Magnevist: Shering Inc, Korea)]를 주기 전 과 1 mmole/kg을 주입한 후 역동적 영상을 2분, 4분, 6분에 각각 3차원 axial fat-suppressed FMP SPGR (spoiled gradient recoiled) sequence로 촬영하였고, 지연기에서도 시 상면 지방억제 T1 강조영상을 얻었다.
모든 역동적 영상(dynamic images)은 감산 영상을 얻었고, 관심 영역에서 시간에 따른 조영의 정도를 시간-강도 곡선 으로 구하였다. 감산 영상(subtraction image)는 조영제 주입
Table 2. Comparison of Mammography, Ultrasonography and MRI For Detection of EIC in Cases with Invasive Breast Cancer Diagnostic method Sensitivity (%) Specificity (%) PPV (%) NPV (%) Accuracy (%)
MMG 48.6 92.3 85.0 66.7 71.6
US 67.5 73.2 71.1 69.8 70.4
MRI 80.5 69.0 71.7 78.4 74.7
All combined 71.4 81.1 78.1 75.0 76.4
EIC: extensive intraductal component, MMG: mammography US: ultrasonography, MRI: magnetic resonance image PPV: positive predictive value, NPV: negative predictive value
Fig. 1. 47-year-old women with ductal carcinoma in situ with microinvasion.
A. Mammogram shows regional distributed pleomorphic mi- crocalcifications (arrow) without mass density at upper portion of the right breast.
B. Sonogram shows tubular and nodular hypoechoic structure
(arrow) with numerous hyperechoic foci representing calcifications and architectural distortion.
C. MR axial subtraction image using contrast-enhanced 3D-FMP-SPGR sequence shows clumped, regional enhancement at right breast. All three diagnostic methods reveal positive findings of EIC.
A
B
C
후 2분 영상에서 조영제를 주입하기 전 영상을 뺀 것이다.
MRI영상은 병변의 형태와 역동적 영상지표에 관하여 전향적 으로 분석하였고 BIRAD에 따라서 기술하였다.
EIC 양성으로의 판정은 다음과 같은 영상 소견으로 정의하 였다. 1) 유방 촬영술에서 종괴 음영의 바깥에 있는 미세 석 회화 혹은 종괴 음영 없이 악성 미세 석회화를 보이는 경우, 2) 유방 초음파에서 종괴 주위에 관상의 저에코 구조가 보이 는 경우 혹은 종괴 바깥에 석회화를 동반한 구조적 파괴 (architectural distortion)가 있는 경우, 3) MRI에서 종괴의 주변에 선상형(linear) 혹은 관상형(tubular)의 조영증강, 분 절형(segmental) 혹은 국소형(regional)의 응집된(clumped) 조영 증강, 그리고 결절(nodular) 혹은 그물모양(reticular)의 조영 증강이 있는 경우로 하였다.
MRI 소견과 조직 슬라이드의 병리학적 상관은 본원 해부 병리과에서 조직 처리과정을 통하여 이루어졌다. 수술 시에 모든 조직은 해부학적 위치를 정확히 기술하였고 7-10 mm 간격으로 축면으로 잘랐다. 종괴의 크기, EIC의 양성 유무, 유 관내 성분의 아형을 평가하기 위하여 병리 보고서를 검토하 였다. Schnitt(7)에 의한 EIC 양성의 정의는 다음과 같다. 1) 관내 상피암(Ductal Carcinoma in situ, 이하 DCIS)이 원발 성 종양의 25% 이상을 이루면서 주변 정상조직에 DCIS성분 이 존재하거나 2) 국소적인 침윤을 동반한 DCIS가 우세한 경 우이다. 유관내 구성성분(intraductal component)에 따른 조
직학적 아형은 크게 면포성 (comedo-type)과 비면포성 (noncomedotype)이 있다.
EIC 양성 유무에 대한 유방 촬영술과 유방 초음파, MRI에 서 각각의 민감도, 특이도, 정확도, 양성예측도, 음성예측도를 계산하였다. 카이스퀘어(Chi square) 검증법으로 통계학적 분 석을 시행하였고 p 값이 0.05 이하이면 통계학적으로 의미가 있는 것으로 보았다.
결 과
조기 유방암으로 확진된 83명 중 41명의 환자에서 EIC양 성이었고 42명은 음성이었다. 세 가지의 영상기법에서 EIC 발견의 민감도와 특이도, 정확도, 양성 예측도, 음성예측도는 표 2와 같다. MRI의 민감도는 유방 촬영술이나 유방 초음파 보다 통계적으로 의미 있게 높았지만(p < 0.05), 특이도는 유 의하게 낮았다(p < 0.05).
양성 예측도는 유방 촬영술에서 가장 높았으나 MRI나 초 음파와 의미 있는 차이는 보이지 않았다. 음성 예측도는 MRI 에서 가장 높았으나 의미 있는 차이는 없었다. 세 가지 영상 기법을 모두 종합하였을 때 EIC에 대한 가장 높은 정확도 (76.4%)를 보였다(Fig. 1).
MRI 검사에서 41명의 EIC 양성 환자 중 33명에서 조영 증 강 영상 초기에 병변을 찾을 수가 있었고 초음파에서는 27명
Fig. 2. 48-year-old women with invasive ductal carcinoma with EIC
A, B. Mediolateral and craniocaudal views of mammogram show spiculated hyperdense mass (arrow) with architectural dis- tortion at right upper outer breast with enlarged axillary lymph node. Microcalcifications are not present within or adjacent to the mass.
C. Sonogram shows ill-defined and irregular shaped hypoechoic mass at right breast.
D. Subtraction MRI image shows linear ductal enhancement extending from main tumor at right breast. Although mammography and sonography cannot reveal positive finding of EIC, MRI diagnoses EIC of the breast cancer.
A B
C
D
에서 병변을 찾을 수 있었다. 유방촬영이나 초음파에서는 발 견할 수 없었으나 MRI에서 선형의 조영증강을 보인 병변은 2예였으며(Fig. 2), 유방촬영이나 초음파 검사에서는 발견할 수 있었으나 MRI에서 조영증강이 되지 않아 찾을 수 없었던 경우는 1예였다(Fig. 3). MRI에서 분절 형태의 선상형 조영 증강을 보였던 2개의 병변은 조직학적으로 유관 과다형성 (ductal hyperplasia)과 섬유낭종성 변화(fibrocystic disease) 로 확인되어 위 양성이었던 경우였다(Fig. 4).
유방 촬영술과 MRI로는 15개의 EIC 양성 병변을 찾을 수 있었고 MRI에서는 발견되었지만 유방 촬영술에서 발견하지 못한 병변은 11개였다. 이 11개의 병변 중 8개(71%)가 조 직학적으로 비면포암종이었다. 면포암종인 경우에는 EIC 양 성 유무를 진단하는데 세 가지 영상기법 모두에서 비교적 높 은 일치도를 보여주었다.
고 찰
광범위한 관내 상피암 성분은 유방 보존 수술 후 수술 경 계면에 암세포 양성인 주요한 원인이 되며, 높은 국소 재발률 과 연관이 있다(7, 8). 미세한 유관내 확장 범위는 수술 시 에 알 수가 없기 때문에 수술 경계면에 암세포가 남아있을 수 있고, 이로 인한 국소 재발률은 5.5-27.9%로 보고되었다(5, 9). 유방 보존 수술 후에 국소 재발이 발생하면 보존된 유방 은 모두 제거하게 되므로 수술 전에 유방암의 유관내 확장 정 도를 정확하게 평가하는 것은 유방 보존 수술의 적합성과 유
방 절제 범위를 결정하는 데 필수적이라고 하겠다.
관내 상피암(DCIS) 혹은 EIC 양성 유방암은 유방 촬영술 에서 미세 석회화로 나타나는 경우가 많고(10), 이는 유방 촬 영술에서 유방암의 범위를 평가하는데 도움을 준다. 범위가 3 cm 이상의 미세석회화를 가진 병변은 3 cm 미만의 병변보 다 EIC 양성일 가능성이 90% 대 54%로 더 높다(10).
유방 촬영술의 EIC 양성 유무의 발견율은 41-83%로 다 양하게 보고되었고(11), 이번 연구에서는 EIC 양성인 병변에 대한 유방 촬영술의 민감도는 48.6%로 유방 초음파나 MRI 의 민감도보다 낮았다. 유방 촬영술에서는 미세석회화가 유일 한 EIC 양성의 증거가 되기 때문에 미세석회화가 없는 병변 일 경우에는 유방 촬영술의 가치는 떨어지므로(12), 본 연구 에서도 암 침범을 진단하는데 유방 촬영술의 민감도가 MRI 에 비해 떨어지리라는 것을 예측할 수 있다.
조직학적으로 DCIS는 면포암종과 비면포암종으로 분류된 다. 일반적으로 면포암종이 비정형 세포를 갖는 경우가 많고, 면포성괴사(comedonecrosis)는 유방 보존 수술 후에 국소 재 발과 연관이 깊은 것으로 알려졌다(13). 이번 연구에서는 면 포암종의 모든 DCIS가 유방 촬영술에서 미세석회화를 보여 주었고, MRI에서 EIC 양성의 소견을 보여주었다.
Tsunoda-Shimazu 등(14)은 초음파의 효율성이 병변의 특 성이나 검사자의 기술, 기계의 공간 해상력 등에 많이 좌우되 는 점이 있지만 비교적 EIC 병변을 잘 발견할 수 있다고 하 였다. Satake 등(15)은 초음파로 암 침범을 진단할 때 민감 도와 특이도, 정확도는 각각 89%, 76%, 85%로 보고하였는
Fig. 3. 48-year-old woman with with invasive ductal carcinoma with EIC
A. Mammogram shows segmentally distributed irregular linear shaped calcifications (arrow) at right breast.
B. Sonogram shows tubular hypoechoic structure (arrow) ex- tending from the main tumor, and reveals calcifications within the main tumor
C. Subtraction MRI image shows spiculated and round shaped enhancing mass at right breast. The mass doesn’t have positive findings of EIC in MRI.
A B
C
데, 이번 연구에서 초음파의 민감도는 67.5%로 MRI 80.5%
에 비하여 낮았다.
Boetes 등(12)은 MRI가 유방암의 크기를 평가하는 데 유 방 촬영술이나 초음파보다 정확하다고 하였고, 다른 연구 결 과에서도 MRI가 유방암의 침범을 비교적 정확하게 규명할 수 있다고 하였다(6, 16-18). 또한, Malur 등(19)은 MRI가 초 음파나 유방 촬영술에 비하여 암 침범을 더 정확하게 발견한 다고 보고하였고, 본 연구에서도 MRI의 EIC에 대한 민감도 는 80.5%로 나타났고 이는 초음파나 유방 촬영술에 비하여 높은 수치였다. 따라서 MRI는 유방 보존 수술을 계획하는 데 EIC의 범위를 좀 더 정확하게 알려줄 수 있기 때문에 수술 범위나 수술 방법을 정하는데 유용한 추가적인 정보를 제공 해 주고 있다.
선상형 혹은 분절형의 조영 증강을 보이는 경우 DCIS를 진 단하는데 도움이 되며, Neubauer 등(20)은 한쪽 유방에서만 관찰되는 분절 형태의 조영 증강이 가장 흔하고 특징적인 DCIS의 영상 소견이라고 하였다. 또한, DCIS의 시간에 따른 조영 증강 패턴과 형태를 함께 분석한 결과 조영 증강을 보 이는 DCIS의 61%가 한쪽 유방에서 분절 형태의 조영 증강 을 보였으며 동시에 plateau 혹은 wash out 형태를 보였다.
이러한 조영 증강 MRI의 기본이 되는 이론은 혈관 생성 이 론이다(21). 유방암에서는 모세혈관의 투과도가 증가하고 간
질 공간(interstitial space)이 넓어진다(22). Folkman 등 (23) 은 쥐를 통한 실험에서 혈관 생성이 몇 개의 과증식 섬 (hyperplastic island)에서 시작되며 이는 발암 과정에서 중요 한 단계라고 하였다. 따라서 유관 과다형성(ductal hyperplasia) 과 같은 섬유낭성 변화(fibrocystic change)에서는 조영 증강 이 약할 것이라고 추측할 수 있고 이로써 유방암과 감별 할 수 있다.
DCIS의 조영증강 패턴은 아직 정확히 밝혀지지 않았지만, 양성 병변과 같은 곡선에서 악성 병변의 곡선까지 다양하게 보일 수 있으며, high grade일수록 악성 병변과 비슷한 조영 증강 패턴을 보이고 있다.
관내 상피암에서 어떤 요소가 액와 림프절 전이, 혹은 생존 율과 관계가 있는지에 관해서 많은 연구가 있었다. Silverberg 등(24)은 유관내 성분(intraductal component)이 많을수록 림 프절 전이가 적고 더 좋은 예후를 보인다고 하였다. 이들은 10% 이상의 침윤이 있는 경우 액와 림프절 전이가 50% 혹 은 그 이상으로 나타난다고 하였고, 일반적으로 침윤이 많고 유관내 확장이 적을수록 림프절 전이가 증가한다고 하였다.
Satake 등(15)은 EIC 양성인 유방암은 심한 침윤성 암에 비 하여 림프절 전이나 원격 전이가 적다고 하였다.
또한, Jing 등(25)은 c-erbB-2의 과다 발현이 EIC양성인 경우에서 더 많이 관찰되며 이러한 경우 종양에 의한 림프 혈 Fig. 4. 43-year-old women with invasive ductal carcinoma with
EIC negative.
A, B. Mediolateral and craniocaudal views of mammogram show spiculated hyperdense mass (arrow) with architectural dis- tortion at right upper outer breast.
C. Sonogram shows spiculated irregular shaped hypoechoic mass at right breast.
D. Subtraction MRI image shows linear ductal enhancement ex-
tending from main tumor at right breast. Despite histopathologic finding reveals intraductal component adjacent the invasive tu- mor, intraductal component within the invasive lesion is less than 10% in total tumor volume.
A B
C
D
관의 혈전증이나 정맥으로의 침윤이 더 많다고 하였다. 하지 만, 본 연구에서는 EIC양성인 경우와 음성인 경우에서 차이 가 없었다.
결론적으로 MRI는 유방암의 유관내 성분을 발견하는데 유 용하다. 하지만, 종괴의 크기가 너무 작거나 종괴 주변에 섬 유낭성 변화가 심한 경우에는 유관내 확장 (intraductal spread)의 범위를 평가하기가 어렵다. 따라서 세 가지 영상기 법을 모두 사용하여 EIC 양성 유무를 평가하는 것이 유방 보 존 수술을 시행한 후 국소 재발을 줄이는 데 도움이 될 것이 다.
참 고 문 헌
1. Holland R, Connolly JL, Gelman R, Mravunac M, Hendriks JH, Verbeek AL, et al. The presence of an extensive intraductal com- ponent following a limited excision correlateds with prominent residual disease in the remainder of the breast. J Clin Oncol 1990;
8:113-118
2. Abner AL, Recht A, Eberlein T, Come S, Shulman L, Hayes D, et al. Prognosis following salvage mastectomy for recurrence in the breast after conservative surgery and radiation therapy for early- stage breast cancer. J Clin Oncol 1993;11:44-48
3. Leborgne F, Leborgne JH, Ortega B, Dolan R, Zubizarreta E. Breast conservation treatment of early stage breast cancer: patterns of failure. Int J Radiat Oncol Biol Phys 1995;31:765-775
4. Veronesi U, Banfi A, Salvadori B, Luini A, Saccozzi R, Zucali R, et al. Breast conservation is the treatment of choice in small breast cancer; long-term results of a randomized trial. Eur J Cancer 1990;
26:668-670
5. Fisher B, Redmond C, Poisson R, Margolese R, Wolmark N, Wickerham L, et al. Eight-year results of a randomized clinical trial comparing total mastectomy and lumpectomy with or without ir- radiation in the treatment of breast cancer. N Engl J Med 1989;320:
822-828
6. Gilles R, Zafrani B, Guinebretiere JM, Meunier M, Lucidarme O, Tardivon AA, et al. Ductal carcinoma in situ; MR imaging- histopathologic correlation. Radiology 1995;196:415-419
7. Schnitt SJ, Connolly JL, Harris JR, Hellman S, Cohen RB.
Pathologic predictors of early local recurrence in stage I and II breast cancer treated by primary radiation therapy. Cancer 1984;
53:1049-1057
8. Boyages J, Recht A, Connolly JL, Schnitt SJ, Gelman R, Kooy H, et al. Early breast cancer: predictors of breast recurrence for patients treated with conservative surgery and radiation therapy. Radiother Oncol 1990;19:29-41
9. Lagios MD, Margolin FR, Westdahl PR, Rose MR.
Mammographically detected duct carcinoma in situ, Frequency of local recurrence following tylectomy and prognostic effect of nu- clear grade on local recurrence. Cancer 1989;63:618-624
10. Stomper PC, Connolly JL. Mammographic features predicting an extensive intraductal component in early stage infiltrating ductal carcinoma. AJR Am J Roentgenol 1992;158:269-272
11. Healey EA, Osteen RT, Schnitt SJ, Gelman R, Stomper PC, Connolly JL, et al. Can the clinical and mammographic findings at
presentation predict the presence of an intensive intraductal com- ponent in early stage breast cancer? Int J Radiat Oncol Biol Phys 1989;12:1217-1221
12. Boetes C, Mus RD, Holland R, Barentsz JO, Strijk SP, Wobbes T, et al. Breast tumors: comparative accuracy of MR imaging relative to mammography and US for demonstrating extent. Radiology 1995;197:743-747
13. Solin LJ, Yeh IT, Kurtz J, Fourquet A, Recht A, Kuske R, et al.
Ductal carcinoma in situ (intraductal carcinoma) of the breast treated with breast conserving surgery and definitive irradiation.
Cancer 1993;71:2532-2542
14. Tsunoda-Shimazu H, Ueno E, Tohno E, Itai Y. Ultrasonographic evaluation for breast conservative therapy. Jpn J Breast Cancer 1996;11:649-655
15. Satake H, Shimamoto K, Sawaki A, Niimi R, Ando Y, Ishiguchi T, et al. Role of ultrasonography in the detection of intraductal spread of breast cancer: correlation with pathologic findings, mammogra- phy and MR imaging. Eur Radiol 2000;10:1726-1732
16. Mumtaz H, Hall-Craggs MA, Davidson T, Walmsley K, Thurell W, Kissin MW, et al. Staging of symptomatic primary breast cancer with MR imaging. AJR Am J Roentgenol 1997;169:417-424 17. Hiramatsu H, Enomoto K, Ikeda T, Mukai M, Furukawa J,
Kikuchi K, et al. The role of contrast enhanced high resolution MRI in the surgical planning of breast cancer. Breast Cancer 1997;4:285-290
18. Drew PJ, Chatterjee S, Turnbull LW, Read J, Carleton PJ, Fox JN, et al. Dynamic contrast enhanced magnetic resonance imaging of the breast is superior to triple assessment for the pre-operative de- tection of multifocal breast cancer. Ann Surg Oncol 1999;6:599-603 19. Malur S, Wurdinger S, Moritz A, Michels W, Schneider A.
Comparison of written reports of mammography, sonography and magnetic resonance mammography for preoperative evaluation of breast lesions, with special emphasis on magnetic resonance mam- mography. Breast Cancer Res 2001;3:55-60
20. Neubauer H, Li M, Kuehne-Heid R, Schneider A, Kaiser WA. High grade and non-high grade ductal carcinoma in situ on dynamic MR mammography: characteristic findings for signal increase and mor- phological pattern of enhancement. Br J Radiol 2003;76:3-12 21. Weidner N, Folkman J, Pozza F, Bevilacqua P, Allred EN, Moore
DH, et al. Tumor angiogenesis: a new significant and independent prognostic indicator in early-stage breast carcinoma. J Natl Cancer Inst 1992;84:1875-1887
22. Revel D, Brasch RC, Paajanen H, Rosenau W, Grodd W, Engelstad B, et al. Gd-DTPA contrast enhancement and tissue differentiation in MR imaging of experimental breast carcinoma. Radiology 1986;
158:319-323
23. Folkman J, Watson K, Ingber D, Hanahan D. Induction of angio- genesis during the transition from hyperplasia to neoplasia. Nature 1989;339:58-61
24. Silverberg SG, Chitale AR. Assessment of significance of propor- tions of intraductal and infiltrating tumor growth in ductal carcino- ma of the breast. Cancer 1978;32:830-837
25. Jing X, Kakudo K, Murakami M, Nakamura Y, Nakamura M, Yokoi T, et al. Intraductal spread of invasive breast carcinoma has a positive correlation with c-erb B-2 overexpression and vascular invasion. Cancer 1999;86:439-448
J Korean Radiol Soc 2006;54:543-550
Address reprint requests to : Doo Kyung Kang, M.D., Department of Diagnostic Radiology, Ajou University, College of Medicine 5 Wonchon-dong, Youngtong-gu, Suwon 442-719, Korea.
Tel. 82-31-219-5114 Fax. 82-31-219-5862 E-mail: [email protected]
Usefulness of Breast MRI for Diagnosing an Extensive Intraductal Component of Breast Cancer: Comparison with
Mammography and Ultrasonography
1Tae Hee Kim, M.D., Doo Kyung Kang, M.D.,Yong Sik Jung, M.D.2, Hyunee Yim, M.D.3
1Department of Diagnostic Radiology, Ajou University, College of Medicine
2Department of General Surgery, Ajou University, College of Medicine
3Department of Pathology, Ajou University, College of Medicine
Purpose: An extensive intraductal component of breast cancer is a principal risk factor for local recurrence, and this is difficult to diagnose with performing only mammography. We investigated the usefulness of breast MRI for evaluating an extensive intraductal component of breast cancer, and we compared this modality with mammography and ultrasonography (US).
Materials and Methods: From March 2003 to July 2004, 90 patients underwent breast MRI among all the pa- tients who were suffering with breast cancer and for whom an EIC was ultimately revealed to be present or not. A total 83 patients with stage I and II breast cancer were finally included in this study. EIC positivity was defined according to the imaging data as follows: 1) microcalcifications beyond the tumor shadow or malig- nant microcalcifications without a tumor mass on mammography, 2) tubular hypoechoic structures adjacent to the tumor or architectural distortion with calcifications beyond the tumor on US, and 3) linear or ductal en- hancement, segmental or regional clumped enhancement, and spotty nodular or reticular enhancement adja- cent to the tumor on MRI. EIC was present in 41 patients and this finding was negative in 42 patients. The re- sults were then compared those results from mammography and US.
Results: The sensitivities of detecting EIC by mammography, US and MRI were 48.6%, 67.5% and 80.5%, re- spectively, and the corresponding specificities were 92.3%, 73.2% and 69.0%, respectively. In the cases that were suspected to be EIC positive on more than two imaging modality, the positive predictive value (PPV) was 78.1%. In cases that were suspected of being EIC positive on just one imaging modality, the negative predic- tive value (NPV) was 75.0%.
Conclusion: Breast MRI provides good information about an EIC of breast cancer and it is a more sensitive study than mammography and US, yet the specificity for the detection of EIC is highest on mammography. A combined evaluation by mammography, US and MRI is the most accurate way to diagnose an EIC of breast cancer.
Index words :Breast
Magnetic resonance (MR) Ultrasound (US)
Mammography