Address reprint requests to Woo Jin Kim, M.D.
Department of Rehabilitation Medicine, Haeundae Paik Hospital Inje University 1435 Jwa-dong, Haeundae-gu, Busan
TEL: 82-51-797-3254, FAX: 82-51-797-3250, E-mail: [email protected] 투고일: 2012년 4월 13일, 수정일: 2013년 4월 22일, 게재확정일: 2013년 4월 22일
안와하신경손상에서 임상 신경 감각 검사와 순목 반사 검사의 상관관계
성균관대학교 의과대학 삼성창원병원 재활의학과, 인제대학교 의과대학 해운대백병원 재활의학과�
박영숙∙김우진�
– Abstract –
Correlation Between Infraorbital Blink Reflex Study and Clinical Neurosensory Test for Diagnosing Infraorbital Nerve
Injury Following Orbitozygomatic Complex Fracture
Young Sook Park M.D., Woo Jin Kim, M.D. *
Department of Physical Medicine & Rehabilitation, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine
Department of Physical Medicine & Rehabilitation, Haeundae Paik Hospital, Inje University School of Medicine
*목
목적적:: 안와 협골 복합체 골절 후 안면 통증 및 감각이상이 동반된 환자에서의 안와하 순목 반사 검사 와 임상 신경감각 검사 사이의 연관성에 대해 알아보고자 하였다.
대
대상상 및및 방방법법:: 20명의 안와 협골 복합체 골절이 있는 환자와 16명의 건강한 정상인을 대상으로 임상 신경감각 검사(clinical neurosensory test) 및 안와하 순목 반사 검사(infraorbital blink reflex study)를 시행하였다. 임상 신경감각 검사로는 주관적인 감각 손상 점수 측정과 두점 식별 검사를 시 행하였으며, 감각 손상 점수 측정은 무감각(0점), 감각 이상(1점), 감각 저하(2점), 정상(3점)으로 기 록하였다. 안와하 순목 검사를 대상자 모두 양측에서 시행하여 early response(R1) 과 bilateral late response(R2, contralateral R2) 파형의 잠시를 기록하여 비교하였다.
결
결과과:: 두점 식별 검사 결과는 환자군과 정상인군에서 각각 평균 20.50± 6.11 mm, 8.15± 3.43 mm이었다. 임상 신경감각 검사 의 각 검사 결과에서 주관적 무감각증(0점)을 호소하는 1명을 제외한 19명에서 감각저하(2점)를 보고하였다. 정상인에서의 R1, R2 contralateral R2(cR2) 잠시는 좌측 은 각각 9.88± 1.79 milisecond (msec), 27.62± 4.86 msec, 26.70± 5.15 msec 이었고, 우측 은 9.80± 1.79 msec, 26.91± 4.88 msec, 25.78± 4.73 msec 이었으며 좌우측 차이는 각각 0.61± 0.51 msec, 1.70± 1.10 msec, 1.85± 1.93 msec 이었다. 환자군에서의 R1, R2 및 cR2 잠시는 정상측에서 10.47 ± 2.54 msec, 28.05 ± 3.66 msec, 28.02 ± 4.77 msec 이었고 환측에서 는 11.53± 3.54 msec, 30.73± 6.04 msec, 30.24± 7.99 msec 이었다. 환자군에서의 정상측과 환측간의 R1, R2, cR2 각각에서의 차이는 1.06± 1.00 msec, 2.68± 2.38 msec, 2.22± 3.22 msec 이었다. 정상군의 결과를 기초로 하였을 때, R1 잠시의 정상 범위는 8.07�11.61 msec 이었 으며, R1 잠시의 양측차는 0�1.13 msec, R2 잠시의 양측차는 0�2.8 msec 으로 관찰되었다. 20
– 21 –
INTRODUCTION
Orbitozygomatic complex (OZC) fracture is the second most common facial fracture, following nasal bone fracture.
It occurs in 10.4 out of 10,000 people, and has higher prevalence in younger men.
1When fracture line involves infraorbital fissure, infraorbital foramen and infraorbital canal, 58 to 95% of patients experience infraorbital neuropathy (ION) due to nerve compression by bony fragment, hematoma, edema or inflammatory neuropathy.
2Patients with OZC fractures present pain or sensory change in cheeks, upper lips and perinasal areas. Surgeons perform physical exams and diagnose infraorbital neuropathy depending on the subjective symptoms before medical prescription or planning surgical treat- ments. Twenty-four to 50% of patients experience persis- tent sensory change and pain. But depending on the method of examination, chronic change or pain persist- ing more than 6 months was reported to vary from 18.8 to 78.8%.
1Difficulty in comparing the results of different studies is due to various measurement methods used including the two-point discrimination, pressure thresh- olds, pinprick test, masseter silent period, thermography, temperature change measurement with ice cubes using ethyl chloride, and incongruent terminologies used for symptom description, different treatment methods of OZC fractures, and the various degree of infraorbital nerve injury according to the severity of trauma.
2Pel- tomaa and Rihkanen
3compared the surgery group and non-nonsurgery group after OZC fracture by a question- naire on subjective symptoms, and found better outcome in the nonsurgery group suggesting surgery itself may damage the nerve in the process of operation. Also, they considered the surgery to be disadvantageous in terms of
costs and recovery period, thus stating a prospective study comparing outcome of spontaneous recovery with the post-surgery outcome is required in the future. There- fore, decision making on surgical performance for a sur- geon is important and diagnosis of infraorbital nerve injury before the operation is essential for judgment of recovery and prognosis. However, surgeons usually make the decision of surgical treatment based on the patients’ subjective symptoms like dysethesia or pain around the fractured area due to lacking objective ways of examining the infraorbital nerve. Moreover, such clin- ical neurosensory test (CNST) is impossible to carry out in those with impaired mentality and communication dif- ficulties after trauma, making it more difficult for the surgeons deciding whether or not operation is needed, further requiring the development of objective evaluation tools. Ohki and Takeuchi
4evaluated the objectivity of the infraorbital blink reflex (IOR) in 9 controls and 22 patients with maxillary lesions and found absence or delay in ipsilateral R1, delay in R2 latency difference.
They also observed that 77% of 13 patients with lesion in the pathway of the infraorbital nerve confirmed by paranasal CT, demonstrated abnormal infraorbital blink reflex. They concluded that infraorbital blink reflex is an objective method to evaluate the infraorbital nerve injury, and that R1 is more useful than the R2. In the present study, we developed a clinical neurosensory test to test the subjective sensory impairment together with the two point discrimination based on other existing clinical neurosensory testings for nerve injury diagnosis.
5We examined the correlation between the CNST and IOR study to find out the diagnostic significance of IOR in patients with facial pain and dysethesia suspected with infraorbital neuropathy after OZC fracture.
명의 환자 중에서 R1의 이상소견을 보인 사람은 14명으로, 4명에선 무반응, 10명에서는 잠시 지연이 보였다. R2의 이상소견을 보인 9명 중 4명에서는 무반응을 5명에서는 잠시 지연이 관찰됨으로서 총 17명에서 이상소견을 보였다. Pearson's correlation통계 방법을 이용하여 17명에서 두점 식별 검사 점수와 환측에서의 R1 잠시 지연 사이의 의미있는 상관 관계(correlation coefficient 0.64)가 관찰 되었다.
결
결론론:: 두점 식별 검사와 R1 잠시 지연 사이의 의미있는 상관관계가 관찰되며 이는 비정상 안와하 순 목 반사 검사 소견이 안와 협골 복합체 골절이 있는 환자에서 동반된 안와하 신경 병변을 발견하는데 도움이 되며, 따라서 임상에서 이러한 평가 방법의 활용이 권장된다.
주
주요요어어:: 안와하 순목 반사 검사, 안와하 신경 손상, 안와 협골 복합체 골절, 임상시험감각검사
SUBJECTS AND METHODS
1. Subjects
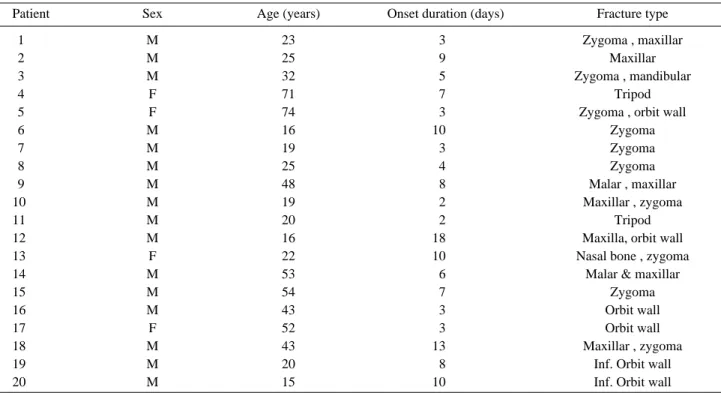
Twenty patients with suspected infraorbital nerve injury following OZC fracture were electromyographi- cally evaluated. The causes of OZC in all of the patients were traumatic. The fracture lesions include zygoma, orbit wall, maxilla, mandible, nasal bone, and malar bone. Sixteen patients were with left OZC fracture while 4 patients were with right OZC fractures. For the patient group, mean duration from onset to initial evaluation was 7.9± 4.0 days, with mean age of 34.5 ± 18.8 years, 16 males and 4 females (Table 1.) Sixteen healthy sub- jects were recruited for the control group, with mean age of 31.4 ± 9.6 years and comprised of 12 males and 4 females. Patients with head trauma, symptoms of facial nerve palsy, severe swelling and bilateral OZC fractures were excluded.
2. Methods
1) Clinical neurosensory test (1) Sensory impairment score
The sensory impairment was tested with a scoring sys- tem we use in our laboratory. Scores for normal, hypoes- thesia without discomfort, dysethesia with discomfort
and anesthesia are 3, 2, 1 and 0, respectively. The patients were asked to indicate the area of the face with most prominent subjective sensory change or impairment on the scoring sheet. Following the subjective sensory impairment scoring, four sites, 1, 2, 3, and 4 indicating right lower eyelid, left lower eyelid, right upper lip area, and left upper lip area, were stimulated by the examiner with cotton swab to grade the degree of sensory change.
The cotton swab was lightly brushed on the skin without applying any pressure, to test the sensory response to light touch. Despite lower eyelid, upper lip area and nasal vestibule being the infraorbital sensory innervated area, nasal vestibule was not included in the sensory test because of the curvature, making it difficult to test with the cotton swab. Upper lip area was defined as the midway between the center of the outer margin of the upper lip to the base of nose. Lower eyelid area was confined to 2cm below the centre of the lower rim of the eye. To avoid desensitization by repetitive touch, each site was tested only once, and the patients were asked to compare with the normal side. Sensory impairment scoring for all four sites were checked and the area with most prominent sensory change was recorded.
(2) Two point discrimination exam
The two point discrimination was performed on cheeks and upper lip area with the subjects’ eyes closed in both
Table 1. Demographic Data of Patients
Patient Sex Age (years) Onset duration (days) Fracture type
1 M 23 3 Zygoma , maxillar
2 M 25 9 Maxillar
3 M 32 5 Zygoma , mandibular
4 F 71 7 Tripod
5 F 74 3 Zygoma , orbit wall
6 M 16 10 Zygoma
7 M 19 3 Zygoma
8 M 25 4 Zygoma
9 M 48 8 Malar , maxillar
10 M 19 2 Maxillar , zygoma
11 M 20 2 Tripod
12 M 16 18 Maxilla, orbit wall
13 F 22 10 Nasal bone , zygoma
14 M 53 6 Malar & maxillar
15 M 54 7 Zygoma
16 M 43 3 Orbit wall
17 F 52 3 Orbit wall
18 M 43 13 Maxillar , zygoma
19 M 20 8 Inf. Orbit wall
20 M 15 10 Inf. Orbit wall
– 23 –
the control and the patient groups. Like the sensory impairment scoring, nasal vestibule was excluded due to irregular surface curvatures. Site for the two-point discrimination evaluation was determined by the result of above sensory impairment scoring to light touch. The two point discrimination was measured using the Lafayette Aesthesiometers A929-2 (Sammons Preston).
The area with the lowest scoring was measured at the point where the subject felt the tips of both needles simultaneously, and set as the threshold in mm. For the patients group, the test was performed on the injured side. The area with most prominent sensory change was colored for the sensory impairment scoring. According to this indicated area, the two point discrimination was carried out at either the lower eyelid or the upper lips.
In cases of most prominent paresthesia or hypoesthesia at nasal vestibule, the two point discrimination was performed at both the lower eyelid and upper lips, the two values were summed up then averaged, and recorded as the two point discrimination distance. As for the normal group, the side on which two point discrimination was tested was randomly selected. The distance was measured in lower eyelid area in 8 control subjects and upper lip area was selected in the rest 8 control subjects.
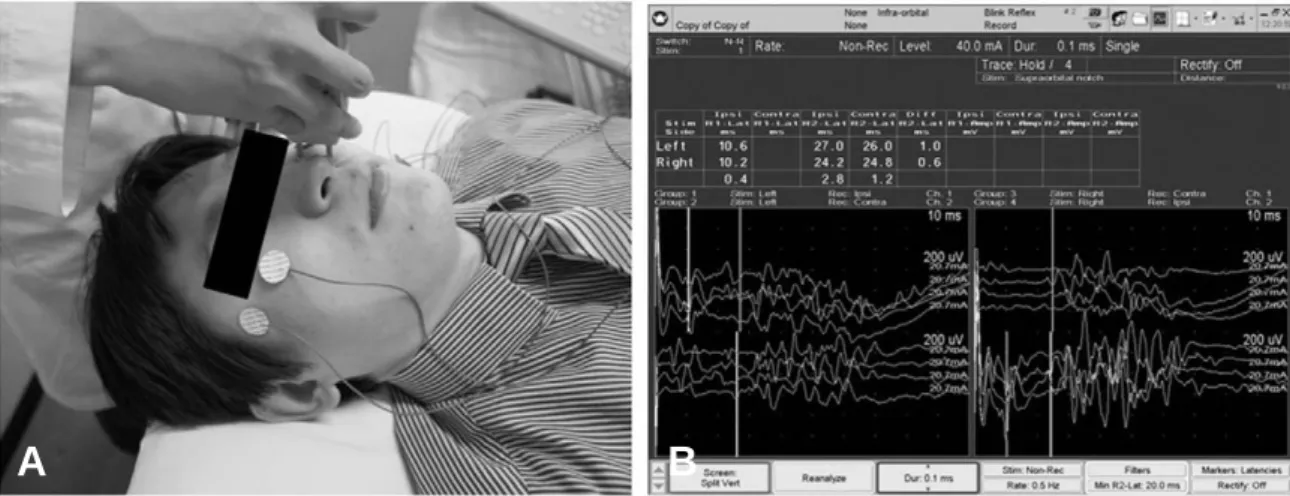
2) Infraorbital blink reflex study
The blink reflex is an eyelid closure in response to an exteroceptive-nociceptive stimulus, consisting of an ipsilateral early component (R1) followed by ipsilateral and contralateral late components (R2 and cR2). Sub- jects were asked to close their eyes in supine position.
Active electrodes were placed over the orbicularis oculi muscle, at the lower eyelids bilaterally, and reference electrode was placed on bilateral temples, lateral to the eye. Stimulating electrodes were pasted on the skin just above infraorbital foramen. Ground electrode was placed on either chin or forehead. Stimulation intensity was 20- 25 mA with duration of 0.1 ms at frequency of 0.5 Hz.
Nicolet Viking Select (Biomedical, Viasys Neurocare, USA) was used with following settings : sensitivity of 200uV/division, sweep speed of 10 msec/division, filter at 20-200 Hz (Fig. 1).
3. Statistics
The two point discrimination distance and infraorbital blink reflex parameters were correlated to examine the relationship between the two point discrimination and R1 latency, side to side difference of R1 and R2 latency
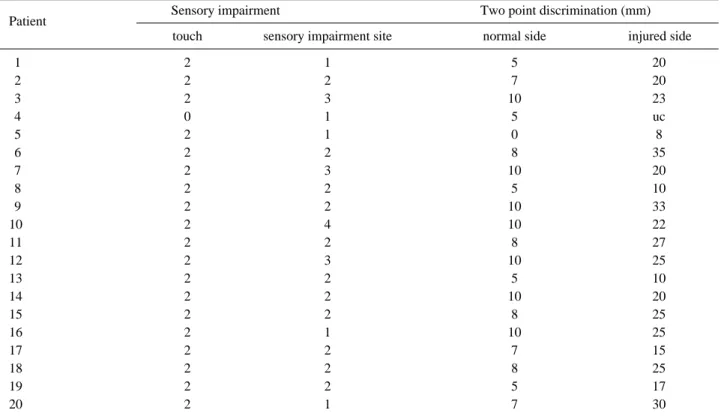
Table 2. Results of Clinical Neurosensory Test
Patient Sensory impairment Two point discrimination (mm)
touch sensory impairment site normal side injured side
1 2 1 5 20
2 2 2 7 20
3 2 3 10 23
4 0 1 5 uc
5 2 1 0 8
6 2 2 8 35
7 2 3 10 20
8 2 2 5 10
9 2 2 10 33
10 2 4 10 22
11 2 2 8 27
12 2 3 10 25
13 2 2 5 10
14 2 2 10 20
15 2 2 8 25
16 2 1 10 25
17 2 2 7 15
18 2 2 8 25
19 2 2 5 17
20 2 1 7 30
touch ; 3, normal, 2, hypoesthesia without discomfort, 1, dysethesia with discomfort and 0, anesthesia. sensory impairment site ; 1, right lower eyelid 2, left lower eyelid 3, right upper lip area and 4, left upper lip area ; uc, uncheckable.
of infraorbital reflex study by the Pearson’s correlation analysis using SPSS for Window version 18.0, with significance value set at P < 0.05. For computation of significance of CNST items, uncheckable response was excluded.
RESULTS
1. Clinical neurosensory test
1) Sensory impairment score
On the sensory impairment score, score 0 was recorded in one patient, score 2 was recorded in 19 patients.
Results for the light touch test at four sites are; 5 patients at site 1, 11 patients at site 2, 3 patients at site 3, and the rest 1 patient at site 4. The most common sensory impairment site was site 2, the left lower eyelid area (Table 2).
2) Two point discrimination exam
In the patients group, range of the two point discrimi- nation distance is 0 to 10 mm on the normal side, and 8 to 30 mm on the injured side. The mean two point discrimination test results of the control and patients
groups on the injured side were 7.4 mm and 21.58 mm, respectively. The two point discrimination could not be measured in one patient with anesthesia (Table 2).
2. Infraorbital blink reflex study
Mean and standard deviation of R1, R2 and cR2 latency for the control group were 9.88 ± 1.79 msec, 27.62 ± 4.86 msec, and 26.70 ± 5.15 msec on left side, and 9.80
± 1.79 msec, 26.91 ± 4.88 msec, and 25.78 ± 4.73 msec on right side. The average values of the right and left of R1, R2 and cR2 latencies were, 9.84 ± 1.79 msec, 27.27
± 4.87 msec and 26.24 ± 4.94 msec, respectively (Table 3). The side to side differences of mean R1, R2, and cR2 latencies in the control group were 0.61 ± 0.51 msec, 1.70 ± 1.10 msec and 1.85 ± 1.93 msec, respectively (Table 4).
Mean latency of R1, R2 and cR2 for the patients group were 10.47 ± 2.54 msec, 28.05 ± 3.66 msec, and 28.02
± 4.77 msec on the normal side, and 11.53 ± 3.54 msec, 30.73 ± 6.04 msec, and 30.24 ± 7.99 msec on the injured side (Table 3). The side to side differences of mean R1, R2, and cR2 latencies in the patient group were 1.06 ± 1.00 msec, 2.68 ± 2.38 msec, and 2.22 ±
Table 3. Results of Blink Reflex of Control and Patients
Ipsilateral R1 (ms) Ipsilateral R2 (ms) Contralateral R2 (ms)
Control 19.84±1.79 27.27±4.87 26.24±4.94
Patient (normal) 10.47±2.54 28.05±3.66 28.02±4.77
Patient (injured) 11.5 3±3.54 30.73±6.04 30.24±7.99
Values are mean± standard deviation
Fig. 1. (A, B, C, D) Stimulation of infraorbital nerve: active electrodes on bilateral lower eyelids, reference electrode on bilateral temples, ground electrode on chin, with stimulation above infraorbital foramen (A). Waveform of the infra- orbital blink reflex from a normal patient (B).
A B
3.22 msec, respectively (Table 4).
Based on the results from control subjects, the normal range of R1 latency, the side to side difference of R1 latency and R2 latency were elicited. The normal range of R1 latency ranged from 8.07 to 11.61 msec. The side to side difference of R1 latency ranged from 0 to 1.13 msec, while side to side difference of R2 latency ranged from 0 to 2.8 msec.
3. Correlation between the two point discrimi- nation and the infraorbital blink reflex study
Correlation between the two point discrimination score and the side to side difference of R1 latency was observed to be significant with correlation coefficient of 0.64, demonstrating prolongation of R1 latency as distance of two point discrimination gets larger in those 17 patients by Pearson’s correlation (p< 0.05). Due to lacking variability of subjective sensory impairment scoring results (1 anesthesia, 19 hypoesthesia), the subjective sensory impairment score of the CNST was excluded from statistical analysis with the IOR parameters.
DISCUSSION
Generally, evaluations for infraorbital nerve injury in the OZC fracture patients are based on the subjective symptoms such as hypoesthesia, throbbing pain, itching sense, tenderness and physical examinations. The causes of above symptoms include soft tissue edema, nerve traction or contusion, or rupture. Depending on the injury mechanism and compressed region, individual fascicles within the infraorbital nerve can be variously affected, thus region of sensory abnormality can vary within its territory eliciting sensory change in upper lips, perinasal, and part or whole cheek.
Trigeminal nerve, the largest cranial nerve, is comprised of ophthalmic nerve, maxillary nerve and mandibular nerve. It innervates sensory of most of the face, oral and tongue, motor of temporalis, masseter, tensor palate, mylohyoid, anterior belly of digastric muscles. The factors making the diagnosis of trigeminal nerve injury difficult
are 1) sensory nerve travels mostly within intracranial and through foramen and out to the skin at its end, 2) deep location of the motor nerves within the facial mus- cles thus making both the stimulation and recording of the action potentials difficult, and 3) trigeminal nerve innervated facial muscles are adjacent to those innervated by the facial nerve, its stimulation induces high amplitude stimulus artifact.
6The blink reflex (BR) is mediated via the trigeminal sensory afferent fibers and their central connections in the trigeminal and facial brainstem nuclei at the level of the lower pons and medulla oblangata. It can be elicited by electrical stimulation of the supraorbital or infraorbital nerves and inconsistently by electrical stimulation of the mental nerve. In clinical neurophysiology, BR is an essential tool for assessment of trigeminal neuralgia, brainstem lesions, and facial nerve palsy.
7In the previ- ously mentioned study by Ohki and Takeuchi, out of 13 patients with abnormality in their afferent pathway in CT, 10 patients showed abnormal BR. They suggested that lesions along this pathway impaired these afferent path- ways of the BR. Also, all patients with abnormal BR showed abnormal R1, while R2 was shown to be abnor- mal in only 40%.
4This means R1 has higher probability to become abnormal than R2, and the latencies on both sides were not always abnormal together. This may be why R1 and R2 pass through different characteristic nerve fibers, although they both share the same root of the infraorbital nerve. The R1 fibers are concerned with tactile sensation, whereas those of R2 are involved with pain and temperature sensation. The different kinds of nerve fibers are thought to have a different susceptibility to lesions. In our study, 14 (70%) out of 20 patient with abnormal R1 response and 9 (45%) with abnormal R2 response were observed, paralleling with the results of above study.
Due to limitations in objective evaluation and making accurate diagnosis of the infraorbital nerve abnormality electromyographically, additional various quantitative measures such as two-point discrimination, pressure thresholds, pinprick test, masseter silent period, gross assessment with sharp and blunt instruments, thermog-
– 25 –
Table 4. Latency Difference of Control(Side to side) and Patients(normal to injured side)
Ipsilateral R1 (ms) Ipsilateral R2 (ms) Contralateral R2 (ms)
Control 0.61±0.51 1.70±1.10 1.85± 1.93
Patient 1.06±1.00 2.68±2.38 2.22± 3.22
Values are mean± standard deviation
raphy, and gross temperature assessments with ethyl chloride, ice, or warmed gutta percha are used in many studies together with the electromyography.
8-11The two point discrimination is a frequently used measurement tool for altered facial sensation after injury and surgery.
8In a study in which trigeminal neuropathy in patients with sensory abnormalities after oral and maxillofacial intervention were compared with healthy group, using cold, warm, and mechanical detection thresholds and pain thresholds, significant difference was observed.
Using Quantitative Sensory Testing (QST), abnormalities and recovery of the trigeminal nerve were monitored, and QST was found to be a useful non-invasive assess- ment method for sensory nerve function (A
β-, A
δ- and C-fiber) in patients with suspected trigeminal neuropathy in the orofacial region.
12It is still controversial what kind of nerve fibers are responsible for R1 and R2. Recently, it was suggested that R1 is mediated by A
β‚ fibers, while R2 is mediated by A
β‚ and A
δfibers. The fibers in descending order of thickness are Aα, A
β, A
δ, and C. The thicker the fibers, the more susceptible to compression or inflammation; the fibers related to R1 may be more fragile. These facts suggest why R1 becomes abnormal more frequently.
4Benoliel et al
1performed neurosensory testings such as calibrated nylon monofilaments, electrical stimulation, heat detection thresholds and response to pin prick to compare the neurosensory testing modalities at immediately after, 1 month and 6 months after operation in zygomatic fracture patients according to the surgical method. 78% and 30% of patients exhibited altered elec- trical and fine mechanical threshold ratios, respectively, whereas 18.8% exhibited pinprick hyper- or hypoalgesia and 24% showed significant altered heat threshold at the 6 month recall. Thermal and painful stimuli are thought to be transduced by thin unmyelinated (C) and thin myelinated (A
δ) fibers. Mechanical and electrical stimuli selectively activate thick myelinated fibers (A
β). The results indicate that the thin nociceptive fibers recover to a larger extent than the mechanoreceptors. Relating the above results to our study, considering the two point dis- crimination as a modality that activates pain, prolonged R1 latency together with increased two point discrimina- tion distance represent injury to both thick myelinated A
βfibers as well as the thin A
δand C fibers.
For patients without consciousness or with poor coop- eration, objective evaluation other than NST is required and in recently published reports, infraorbital blink reflex study demonstrated significant correlation com-
pared to the radiological findings in patients with infra- orbital nerve injury.
Conscious patients with isolated facial fractures and no other injuries are able to undergo NST of the peripheral branches of the trigeminal nerve, followed by prompt reduction and fixation of the fractures and any associated nerve injury. Factors affecting spontaneous recovery of the infraorbital nerve function after facial fractures include gender, age, fracture displacement, fracture site, type of fracture treatment, and interval between injury and fracture repair.
13Persistent symptoms more than 6 months is reported to be between 18.8% and 78.8%
though it may differ depending on the testing methods.
1In those with persisting symptoms after surgical manage- ment, sometimes can be confused with complications following the operation, increasing the necessity of pre- operation evaluation of infraorbital nerve injury for both the patient and surgeon to predict recovery and prognosis.
However, this study is limited in several ways.
Because of small number of patients included, greater number of patient would further verify the validity of IOR. From the results above, it is difficult to conclude that either the two point discrimination or R1 latency are definitive methods for diagnosis of the infraorbital nerve injury as our study failed to find the significance of each testing modalities. Further study correlating each of the R1 latency and the two point discrimination with imaging studies, CT for example, would further verify specificity of each modalities, and may thus offer a guideline for the treatment of ION. Also correlating the R2 response with the two point discrimination for their diagnostic sensitivity for assessing smaller fibers, would further expand clinical utility of blink reflex for enabling better prediction of recovery and prognosis by both the surgeons and patients.
Nevertheless, this study has proved the clinical utility
of infraorbital blink reflex study, especially the R1
latency, in displaying the degree of nerve injury in
numerical value. This provides quantitative measurement
of the neuropathy at follow up of the patients. Significant
correlation between the R1 latency and the two point dis-
crimination test indirectly indicate the clinical usefulness
of the two point discrimination for reflecting infraorbital
nerve injury, enabling simple use and diagnosis of infra-
orbital nerve injury in clinical setting. For unconscious
patients who cannot cooperate when asked or tested with
CNST, the infraorbital blink reflex study would be an
alternative method with superior objectivity.
– 27 –
CONCLUSION
Two point discrimination and infraorbital blink reflex study in orbitozygomatic complex (OZC) fracture patients before surgical treatment is helpful in detecting accompaniment of infraorbital nerve injury, and thereby making decisions on surgical treatment and predicting prognosis. It may also provide useful information on changes in patients’ status and explanation or discrimi- nation of post-surgical complications.
REFERENCES
1. Benoliel R, Birenboim R, Regev E, Eliav E: Neurosensory changes in the infraorbital nerve following zygomatic fractures. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005: 99: 657-665.
2. Vriens JP, van der Glas HW, Bosman F, Koole R, Moos KF: Information on infraorbital nerve damage from multi- testing of sensory function. Int J Oral Maxillofac Surg 1998: 27: 20-26.
3. Peltomaa J, Rihkanen H: Infraorbital nerve recovery after minimally dislocated facial fractures. Eur Arch Otorhino- laryngol 2000: 257: 449-452.
4. Ohki M, Takeuchi N: Objective evaluation of infraorbital nerve involvement in maxillary lesions by means of the blink reflex. Arch Otolaryngol Head Neck Surg 2002:
128: 952-955.
5. Zuniga J, Meyer R, Miloro M: The Accuracy of clinical neurosensory testing for nerve injury diagnosis. J Oral
Maxillofac Surg 1998: 56: 2-8.
6. Park HR, Lee YS, Jang KE, Lee SJ: Electrodiagnostic study for the trigeminal nerve. J of Korean Acad of Rehab Med 1992: 16: 431-437.
7. Bernard JM, Pereon Y: Nerve stimulation for regional anesthesia of the face: use of the blink reflex to confirm the localization of the trigeminal nerve. Anesth Analg 2005: 101: 589-591.
8. Essick GK, Phillips C, Turvey TA, Tucker M: Facial altered sensation and sensory impairment after orthognath- ic surgery. Int J Oral Maxillofac Surg 2007: 36: 577-582.
9. Essick GK, Phillips C, Zuniga J: Effect of facial sensory re-training on sensory thresholds. J Dent Res 2007: 86:
571-575.
10. Sakavicius D, Juodzbalys G, Kubilius R, Sabalys GP:
Investigation of infraorbital nerve injury following zygo- maticomaxillary complex fractures. J Oral Rehabil 2008:
35: 903-916.
11. Schmid D, Messlinger K, Belmonte C, Fischer MJ:
Altered thermal sensitivity in neurons injured by infraor- bital nerve lesion. Neurosci Lett 2011: 488: 168-172.
12. Yekta SS, Koch F, Grosjean MB, Esteves-Oliveira, Ghas- semi A, Riediger D, et al: Analysis of trigeminal nerve disorders after oral and maxillofacial intervention. Head Face Med 2010: 6: 24.
13. Fogaca WC, Fereirra MC, Dellon AL: Infraorbital nerve injury associated with zygoma fractures: documentation with neurosensory testing. Plast Reconstr Surg 2004: 113:
834-838.